
Abstract
Abstract
Introduction:
Although laparoscopic inguinal hernia repair in children has gained popularity in the last decades, this approach remains uncommon in preterm infants. The aim of this study was to compare the characteristics and the outcomes of indirect inguinal hernias in term and preterm infants.
Material and Methods:
From January 2002 to November 2015, all charts of the pediatric patients who underwent laparoscopic indirect inguinal hernia repair in one single institution within the first 6 months of life were revised. The data of 156 patients were analyzed retrospectively. Patients were divided in two groups: group I, including the preterm patients, and group II, including the term patients.
Results:
A total of 90 preterm infants and 66 term infants were included. In the group I, preoperative diagnosis was right-sided inguinal hernia in 20% of patients, left sided in 22.2%, and bilateral in 57.5%; while in the group II, preoperative diagnosis was right-sided inguinal hernia in 42.4% of infants, left sided in 15.2%, and bilateral in 42.4% (P = .01). In group I intraoperative diagnosis was right-sided inguinal hernia in 10% of patients, left sided in 16.7%, and bilateral in 73.3%; while in the group II, intraoperative diagnosis was right-sided inguinal hernia in 25.8% of infants, left sided in 12.1%, bilateral in 60.6%, and there was no hernia in one patient (P = .02). However, there was no statistically significant difference in the correct intraoperative diagnosis between both groups (P = .59). No statistical significance was observed between the two groups regarding postoperative complications.
Conclusions:
Bilateral inguinal hernia is more frequent in preterm infants compared to term infants, whereas the incidence of right-sided inguinal hernia is higher in term patients. Laparoscopic inguinal hernia repair in preterm infants seems to be safe and effective.
Introduction
Indirect inguinal hernia repair is one of the most common surgical procedures performed in preterm infants. 1 Its incidence varies from 0.8% to 5% in term patients and rises to 30% in preterms.1,2 The majority of the cases are operated during the first year of life. 3 Although laparoscopic inguinal hernia repair in children has gained popularity in the last decades, this approach remains uncommon in preterm infants, and there are only a few reports in the literature.4–6 The aim of this study was to compare the characteristics and the complication rates of laparoscopic inguinal hernia repair in term and preterm infants <12 months of age.
Materials and Methods
Between January 2002 and November 2015, we retrospectively analyzed 156 patients that underwent laparoscopic inguinal hernia repair within the first 12 months of life. Patients were divided into the following two groups according to their gestational age: preterm group and term group. Prematurity was defined as <37 weeks of gestational age. Corrected age was calculated for preterm infants and was defined as the chronological age minus the number of weeks of those born with <40 weeks. The exclusion criteria were as follows: patients with unknown gestational age and children without preoperative diagnosis of inguinal hernia.
Patient demographics, clinical presentation, intraoperative findings, and postoperative complications were evaluated in both groups. The diagnosis of inguinal hernia was clinical. Patients admitted in neonatal unit were usually operated before neonatal discharge. If patients presented with incarceration, an attempt of reduction was made, if successful, surgical repair was performed about 2–3 days later. Irreducible hernias were operated on immediately. Indications for laparoscopic repair were as follows: bilateral inguinal hernia, unilateral inguinal hernia associated with umbilical hernia, doubtful diagnosis, and recurrence after either laparoscopic or open repair. Incarcerated and irreducible hernias were performed by laparoscopy.
All patients underwent laparoscopic inguinal hernia repair under general anesthesia. They were placed in supine position in a Trendelenburg position to mobilize the bowel by gravity and improve visibility in the surgical field. We performed a transperitoneal approach using three ports. Local anesthesia was realized with 0.25% bupivacaine in every incision. In males, we also infiltrated saline solution with a percutaneous needle under the peritoneum with the aim to separate the peritoneum from the spermatic cord (Fig. 1). Open inguinal rings were closed with 3/0 Prolene in a purse-string suture. If a contralateral hernia or processus vaginalis was noted, it was repaired at the same time. Recurrence is defined as a persistent hernia after previous ipsilateral hernia repair.
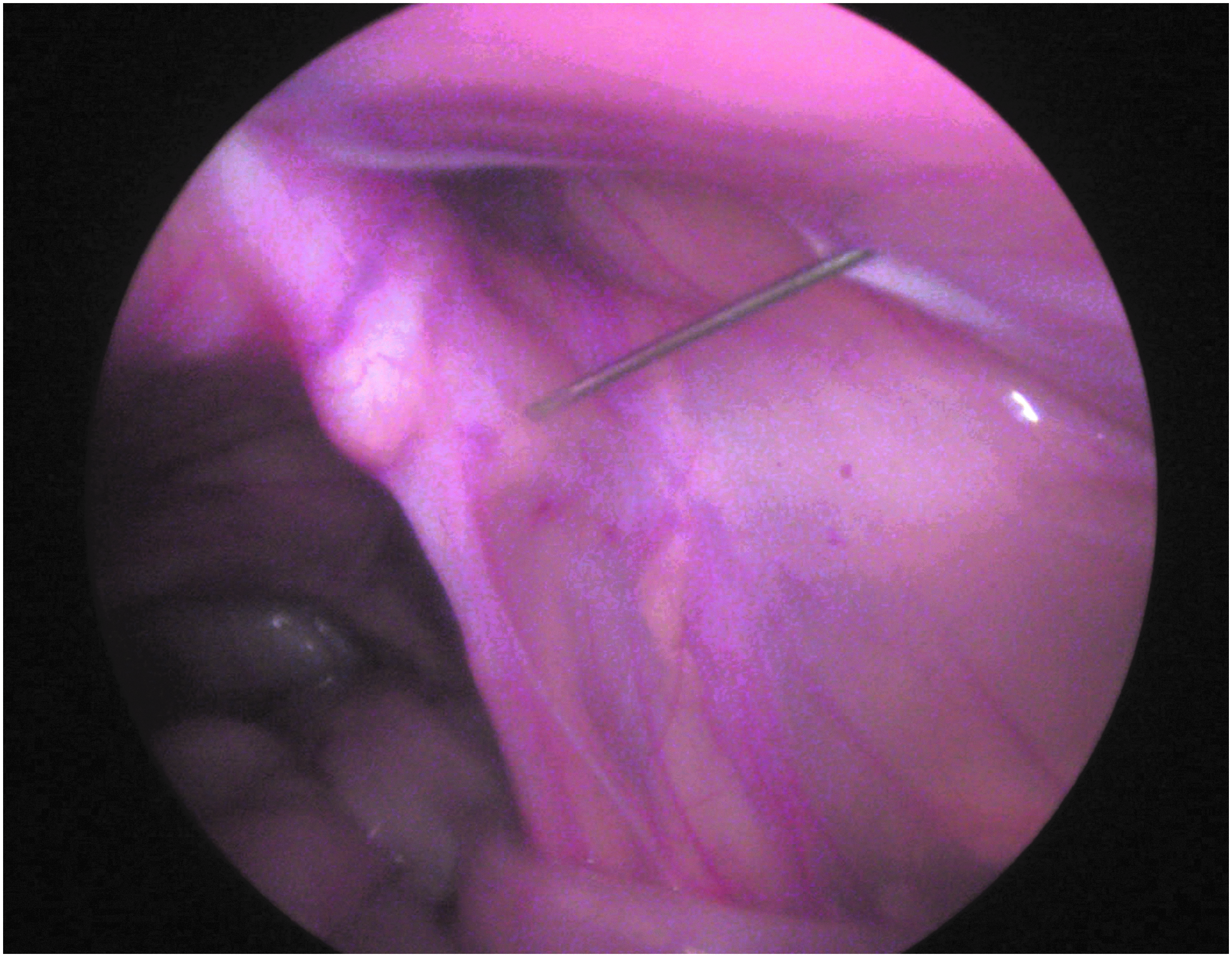
Infiltration of the peritoneum.
SAS® 9.3 software was used for all statistical analyses. Because of the small samples, nonparametric tests were used to compare the groups. Continuous variables were compared using Wilcoxon rank-sum test, and categorical variables were compared using Pearson chi-square test. A P value <.05 was considered statistically significant.
Results
There were 90 (57.7%) patients in preterm group and 66 (42.3%) patients in term group. The incidence of hernia repair was significantly higher in males than in females in both groups. In preterm group, mean gestational age at birth was 30.7 weeks (range 24–36 weeks), and mean birth weight was 1.5 kg (range 0.4–3.8 kg); while in term group, mean gestational age was 38.2 weeks (range 37–41 weeks), and mean birth weight was 2.9 kg (range 1.6–3.6 kg). Demographic comparisons are shown in Table 1.
Demographic Comparisons Between Preterm and Term Patients
We found statistically significant differences in the preoperative clinical diagnosis between both groups (P = .01). Among the 90 preterm patients, preoperative diagnosis was right-sided hernia in 18 (20%) patients, left-sided hernia in 20 (22.2%), and bilateral hernia in 52 (57.8%). However, in the term group, 28 (42.4%) had a right-sided hernia, 10 (15.2%) a left-sided hernia, and 28 (42.4%) a bilateral hernia. Ten children (six preterm and four term) presented with hernia recurrence after having undergone open inguinal hernia repair (seven unilateral and three bilateral). Umbilical hernia was diagnosed in 60 (66.7%) patients in preterm group and in 31 (47%) patients in term group (P = .02).
No significant differences were observed in incarcerated hernias between both groups. Episodes of incarceration in the right side were identified in 14 (15.6%) patients in preterm group and in 9 (13.6%) patients in term group (P = .81), while the diagnosis of left-sided incarcerated hernia was made in 10 (11.1%) patients in preterm group and in 7 (10.6%) patients in term group (P = .70). Three patients underwent emergency hernia repair due to a nonreducible hernia. Eighteen children underwent surgery after hernia reduction.
In preterm group, mean age at operation was 125.9 days (range 32–445 days), mean corrected age was 62.9 days (range 0–365 days), and mean body weight was 4.3 kg (range 1.6–8.8 kg). In term group, mean age at operation was 138.8 days (range 16–351 days), and mean body weight was 6.3 kg (range 3.1–10.5 kg). Based on the intraoperative findings, there were also statistically significant differences in the diagnosis between both groups (P = .02). Indirect inguinal hernia occurred on the right side in 9 (10%), on the left side in 15 (16.7%), and bilaterally in 66 (73.3%) preterm patients. However, in term group, 17 (25.8%) had a right-sided hernia, 8 (12.1%) had a left-sided hernia, 40 (60.6%) had bilateral hernia, and 1 patient had no hernia (1.5%). Preoperative and intraoperative diagnoses are reported in Table 2. A total of 156 laparoscopic herniorrhaphies were performed in preterm group, while 105 laparoscopic herniorrhaphies were performed in term group. No significant differences were observed in the correlation between preoperative diagnosis and intraoperative findings in both groups (P = .59). Preoperative diagnosis coincided with intraoperative findings in 66 (73.3%) preterm patients and in 45 (68.1%) term patients.
Preoperative and Intraoperative Diagnosis in Both Groups
With regard to intraoperative findings, six Amyand's hernias (five preterm and one term) were found. All the patients were male. There were five right sided and one left sided associated with bowel malrotation (Fig. 2). No appendectomy was performed. All the procedures were completed by laparoscopy except for one irreducible hernia, which required conversion to open surgery due to the difficulty to reduce the hernia. Intestinal lesions such as edema or hematomas were observed in the 11.1% of the patients that underwent laparoscopic repair during the admission after the hernia reduction. Intraoperative complications were similar in both groups (P = .16). Of the 156 inguinal hernias operated in preterm group, 2 (1.28%) cases had a minimal bleeding in the inguinal ring with spontaneous resolution, while this complication was observed in 3 (2.85%) of the 105 inguinal hernias operated in term group.

Left Amyand's hernia.
The mean operative time was significantly longer in preterm group (58.0 minutes) compared to term group (55.3 minutes) (P < .01). The mean length of stay in preterm and term group was 2.6 ± 6.3 days and 0.65 ± 0.9 days, respectively (P < .01). There were no significant differences between the two groups in the rate of postoperative complications. Port-site infection and recurrent umbilical hernia occurred in 2 (2.3%) and 3 (3.4%) preterm patients, respectively. No port-site infection or umbilical port-site hernia was observed in term group (P = .75 and P = .39, respectively). One (1.3%) male patient of the 76 males in preterm group had a transient hydrocele. No hydroceles were observed in term group (P = .99). Of the 156 inguinal hernias operated in preterm group, 5 (3.2%) hernias presented with recurrence postoperatively, while this complication was found in 1 (0.9%) hernia of the 105 inguinal hernias operated in term group (P = .46). All the recurrences were repaired laparoscopically in average 22.7 months (range 2–57 months) after the first surgery. No patient developed a metachronous hernia or testicular atrophy in a minimum follow-up of 30 months. We have found 7 cases of high testes in 5 patients (2 preterm and 3 term), and we have performed 178 repairs in male patients. Therefore, our rate of high testes was 3.9%. However, high testes and testicular ectopia had been preoperatively observed in three and one patient, respectively. There were two right sided, one left sided, and two bilateral. The mean age of these patients at previous operation was 5.9 months. Orchiopexy was performed in all of the cases at a mean follow-up of 28.7 months.
Discussion
Pediatric hernias are almost always indirect, resulting from the persistence of the processus vaginalis. Because the processus vaginalis usually closes between 36 and 40 weeks of gestation and the frequent presence of diseases associated with an increased intra-abdominal pressure, premature patients have a higher chance of developing inguinal hernias. 1 The true incidence of inguinal hernia is unknown. The rate of inguinal hernia repair varies from 0.8% to 5% in term infants and rises to 30% in preterm infants.1,2 It has been demonstrated that the incidence rate is highest during the first year of life and then decreases as age increases. 3 Sex distribution has a significant male predominance,2,3 as seen in our study.
Although the majority of the studies in the last decades have focused on the laparoscopic approach, scientific community is still debating the best approach for inguinal hernia repair in children. 4 One of the main advantages of laparoscopy resides in that it can be used as a diagnostic tool. Patent processus vaginalis and contralateral hernias are found in a significant number of patients, especially in the youngest age group.4–6 We agree with other authors that there are statistically significant differences in the presentation and laterality of inguinal hernia between term and preterm patients. 5 In our series, the majority of the preterm patients presented with a primary bilateral hernia as it was reported previously.5,6
Another benefit of laparoscopic surgery is the possibility to repair these contralateral patent processus vaginalis, to avoid a future metachronous hernia. The risk of developing a metachronous hernia is reported as 10.5–14.3% in patients who underwent open inguinal repair within the first year of life and it rises to 28% in preterm infants.2,7 After laparoscopic treatment, no metachronous contralateral hernia was found in our series. Although not all patent processus vaginalis will develop into a clinical hernia, 1 current levels of evidence do not show any increase in morbidity from the treatment of contralateral hernia or processus vaginalis when diagnosed by laparoscopy. 8 Therefore, we recommend repairing hernias or processus vaginalis, even if asymptomatic.
Surgical inguinal hernia repair is recommended because of the risk of incarceration, which seems greater in premature patients.4–8 In our series, although the incidence of incarceration was slightly higher in preterm group (26.6% versus 24.2%), there was no significant difference in the rate between both groups. Similar results have been published previously.5,9 Complications of incarceration include bowel strangulation or necrosis, as well as testicular or ovarian compromise. 8 Laparoscopic approach seems to have a lower rate of complications in emergency cases. 10 In addition, it allows the evaluation of bowel viability.4,10 However, distended bowel and irreducible hernias may create technical difficulties in laparoscopic treatment. 10
Although minimally invasive surgery is significantly known to be a safe procedure in newborns, laparoscopic approach for inguinal hernia repair in this population is still up for debate. 6 In contrast to open surgery, there are a lot of laparoscopic techniques for inguinal hernia repair. Therefore, comparisons between studies are hampered by the procedure disparity. 10 In general, laparoscopic treatments reduce iatrogenic injury to the spermatic cord as they avoid dissection of hernial sac. 10 Open herniorrhaphy in neonates is a technically demanding procedure due to the thin vessels and vas deferens and the fragile hernia sac. 11 It has been suggested that laparoscopic inguinal hernia repair in neonates is technically less demanding than open surgery.3,11 We agree with other authors that laparoscopic repair is also a technically demanding procedure, as a purse string suture must be done in a small space. 12 Laparoscopic approach is considered the gold standard in the treatment of recurrence after open repair as it avoids the adhesions of previous operation and it may look for the cause of recurrence.4,10
Inguinal repair in neonates and infants seems to be associated with a high risk of postoperative complications. 2 However, several studies have reported a low rate of complications after laparoscopic inguinal hernia repair in preterm patients.11,12 The superiority of laparoscopic surgery over the classic approach continues to be debated. Wound infection rate seems less with laparoscopic repair due to the small size of the incisions and the scar localization outside the diaper area.4,11 It has been suggested that the recurrence rate following laparoscopic repair may be higher compared to open surgery. 8 However, in preterm patients, recurrence rate after open approach ranges from 2.3% to 9%,7,13 and recurrence rate after laparoscopic surgery ranges from 1.3% to 4.4%.6,11,12 In our series, there were no significant differences between preterm and term group in the incidence of postoperative complications. Our rates of complications are comparable to those reported in the literature.11,12
The rate of cryptorchidism and testicular atrophy seems to be higher after open repair than after laparoscopic approach.4,14 Nagraj et al. 15 have reported a rate of 2.7% of high testes requiring orchiopexy after open inguinal hernia repair. However, their rate was calculated taking into account all inguinal hernia repairs, including girls. 15 Pini Prato et al. 2 made the same mistake and they have reported a rate of 0.5%. 2 Our rate was 3.9%, taking into account only repairs in male patients. Therefore, the comparison between these rates is not valid because the reports are not prepared according to similar criteria. As reported by Esposito et al., the majority of our patients presented high testes preoperatively, and we decided to correct them at 12–18 months of age. 11 We have also agreed with Nagraj et al. that it is not clear if high testes after laparoscopic inguinal hernia repair are a consequence of prematurity or surgical manipulation. 15 In addition, the manipulation of spermatic cord in our technique is minimal due to the hydrodissection. Our data suggest that laparoscopic inguinal hernia repair in term and preterm infants seems to be safe and effective. However, prospective randomized studies will be necessary to verify this question. Strict formulas should be mandatory to compare the rate of complications.
Footnotes
Disclosure Statement
No competing financial interests exist.