
Abstract
Abstract
Background:
Operative maneuvers to increase mesenteric length during ileal pouch-anal anastomosis (IPAA) are frequently utilized in adults, but limited data exist on the need for their use in children.
Materials and Methods:
A retrospective chart review of children (age <18) considered for IPAA creation at two affiliated tertiary referral centers from 2007 to 2017 was conducted, and patient factors, operative details, and 30-day postoperative complications were abstracted. Body mass index (BMI) was normalized to BMI percentile-for-age-and-sex and classified as underweight (BMI <5th percentile), healthy weight (5th ≤ BMI percentile <85th), or overweight/obese (BMI ≥85th percentile). Maneuvers were identified from operative notes. Univariate analysis and multivariable logistic regression were performed to determine independent factors associated with the use of maneuvers.
Results:
A total of 94 patients underwent attempt at IPAA creation, which was successful in 91 (97%). Fourteen (15%) of 91 patients were classified as overweight or obese. The 3 failures occurred secondary to inability to reach in 3 patients, with specific mention of patients' obesity in 2 and pouch ischemia in 1. Sixty (66%) patients required maneuvers to lengthen the mesentery. Overweight/obese patients required maneuvers more often than nonoverweight/obese patients (93% versus 61%, P = .03). There were no differences in 30-day maximum Clavien-Dindo scores between patients with and without maneuvers performed (P = .83). Being overweight/obese was an independent risk factor for requiring maneuvers (odds ratio: 9.3, 95% confidence interval: 1.1–82.8) after adjusting for age, sex, height, operative stage, and surgeon.
Conclusion:
Surgeons should be prepared to perform mesenteric lengthening maneuvers when operating on pediatric patients to ensure minimal tension on the IPAA, and more so when operating on obese children. Whether these maneuvers have an impact on long-term pouch function is undetermined.
Introduction
Obesity rates are high in children in high-income countries, including those with medically refractory ulcerative colitis (UC) and familial adenomatous polyposis (FAP). Although one might expect a chronic illness such as UC to decrease weight gain or body mass index (BMI), studies have found that 1 in 3 children with UC are overweight/obese, similar to the general population.1,2 Many of these patients will require colectomy for medical failure or dysplasia, and most will desire restoration of intestinal continuity in the form of ileal pouch-anal anastomosis (IPAA).
IPAA has been shown to be a safe and effective procedure with good functional outcomes in pediatric populations.3–5 The experience of laparoscopic IPAA in children has shown that the procedure is safe, feasible, and achieves comparable outcomes with open approaches with shorter hospital stays.6,7 The success of the procedure, however, depends on surgeon's technical experience and patient selection. These factors affect the utilization and conduct of the procedure—not every patient is offered IPAA, some attempts at IPAA fail, and some operations are more difficult than others. While the adult literature has associated age, technical factors, and obesity as risk factors for failure of IPAA formation, no studies in the pediatric population have examined technical or patient factors related to difficulty in creating a tension-free anastomosis.
The reason for IPAA failure and difficulty is often [if not always] inadequate mesenteric length to accommodate the anastomosis. Surgeons employ a number of maneuvers to increase mesenteric length to avoid this problem, including mobilization of the small bowel mesentery, creation of mesenteric windows, high ligation of the ileocolic pedicle, and ligation of terminal pouch vessels.6,8 These maneuvers are employed with some variability among surgeons, but knowledge and expertise in each of them are necessary when tension is present on the IPAA. 9 Therefore, our aim was to determine (1) how often advanced maneuvers are utilized in pediatric patients, (2) what factors are associated with the need for these maneuvers, and (3) if they have any impact of 30-day postoperative outcomes.
Materials and Methods
After approval from the Mayo Clinic Institutional Review Board, we reviewed pediatric patients (age <18 years at operation) with a diagnosis of FAP, indeterminate colitis, and UC considered for IPAA at the Mayo Clinic Rochester or the Mayo Clinic Florida campuses between January 1, 2007 and December 31, 2017. Both institutions are large, academic tertiary referral hospitals.
Patient cohort
We reviewed the hospital records of all patients who underwent either subtotal colectomy or total proctocolectomy over the study period, and determined whether they were considered for IPAA. Reasons for withholding IPAA were determined from consultation notes and operative notes from gastroenterology and pediatric surgery. Patients who underwent subtotal colectomy but who were not offered IPAA due to a suspicion of Crohn's disease were excluded. Redo IPAA operations were also excluded from the analysis.
Primary and secondary outcomes
The primary outcome of this study was whether maneuvers were utilized in the creation of IPAA. Secondary outcomes included operative times, readmission 30 days after discharge, and 30-day postoperative complications.
Variables
Patient demographics, including age, sex, and BMI at the time of the IPAA attempt, were obtained from the medical chart. BMI was normalized to BMI percentile-for-age-and-sex and classified as underweight (BMI <5th percentile), healthy weight (5th ≤ BMI percentile <85th), or overweight/obese (BMI ≥85th percentile). Operative reports were reviewed by 2 authors (M.T. and J.Y.), and details on lengthening maneuvers were recorded. Four pediatric surgeons and 10 colorectal surgeons performed the operations reviewed. Maneuvers included creation of mesenteric windows, high ligation of the ileocolic pedicle, ligation of the superior mesenteric artery, and additional mobilization of the small bowel mesentery after a failed test of pouch length (Fig. 1). Thirty-day postoperative outcomes including readmission, ileus, infectious complications, and reoperation were also collected.
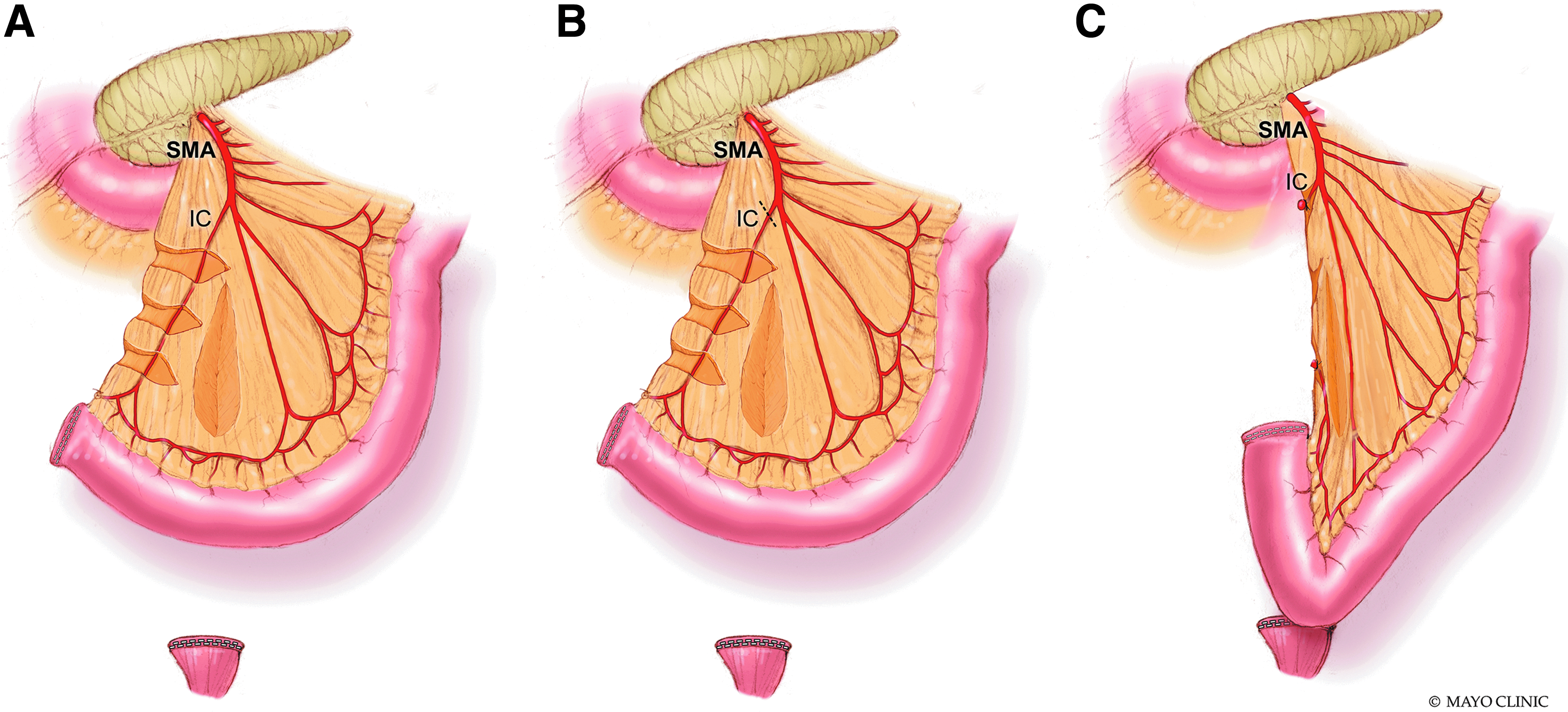
Maneuvers to increase mesenteric length during IPAA.
Statistical analysis
Continuous variables with normal distribution were summarized with mean and standard deviation, whereas nonparametric continuous variables were summarized with medians, interquartile ranges, and ranges. Categorical variables were summarized with frequency counts and percentages. Patient characteristics and outcomes were compared based on whether maneuvers were employed at the time of IPAA creation using chi-square tests for categorical variables, independent t-tests for continuous normally distributed variables, and Wilcoxon rank sum for continuous nonparametric variables. A test for trend of the probability of maneuver utilization was performed across BMI categories.
Multivariable logistic regression was performed to assess independent factors affecting the need for operative maneuvers. Covariates were selected based on relevance to mesenteric length (age, sex, height, and BMI) and significance on univariate analyses. Given the small number of operations performed by each colorectal surgeon, we grouped these surgeons and compared them with individual pediatric surgeons to account for differences in dictation practice. We created two multivariable models for odds of maneuvers being utilized. Both models incorporated age, sex, height, operative stage, and operating surgeon. In the first model, overweight/obese versus neither was modeled as a binary variable. In the second, BMI percentile-for-age-and-sex was modeled as a continuous variable. The multivariable analysis results were expressed as odds ratios (ORs) with 95% confidence intervals (CIs) calculated using likelihood-ratio tests. Statistical significance was set at P < .05. All data analyses were performed using STATA® 15.1 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
Results
Of 103 patients, 52 underwent total proctocolectomy with attempted IPAA, 51 underwent subtotal colectomy with IPAA attempted at a second operation, and 9 did not undergo an attempt at IPAA creation. Reasons for not attempting IPAA included growth concerns (n = 4), ongoing medical evaluation (n = 2), patient preference (n = 2), and obesity (n = 1) (Fig. 2). The diagnostic indication for IPAA creation was UC in 63 (67%), FAP in 25 (27%), indeterminate colitis in 5 (5%), and total colonic Hirschsprung's disease in 1 (1%). One UC patient had a concurrent diagnosis of juvenile polyposis, and 1 FAP patient had concurrent Hirschsprung's disease.
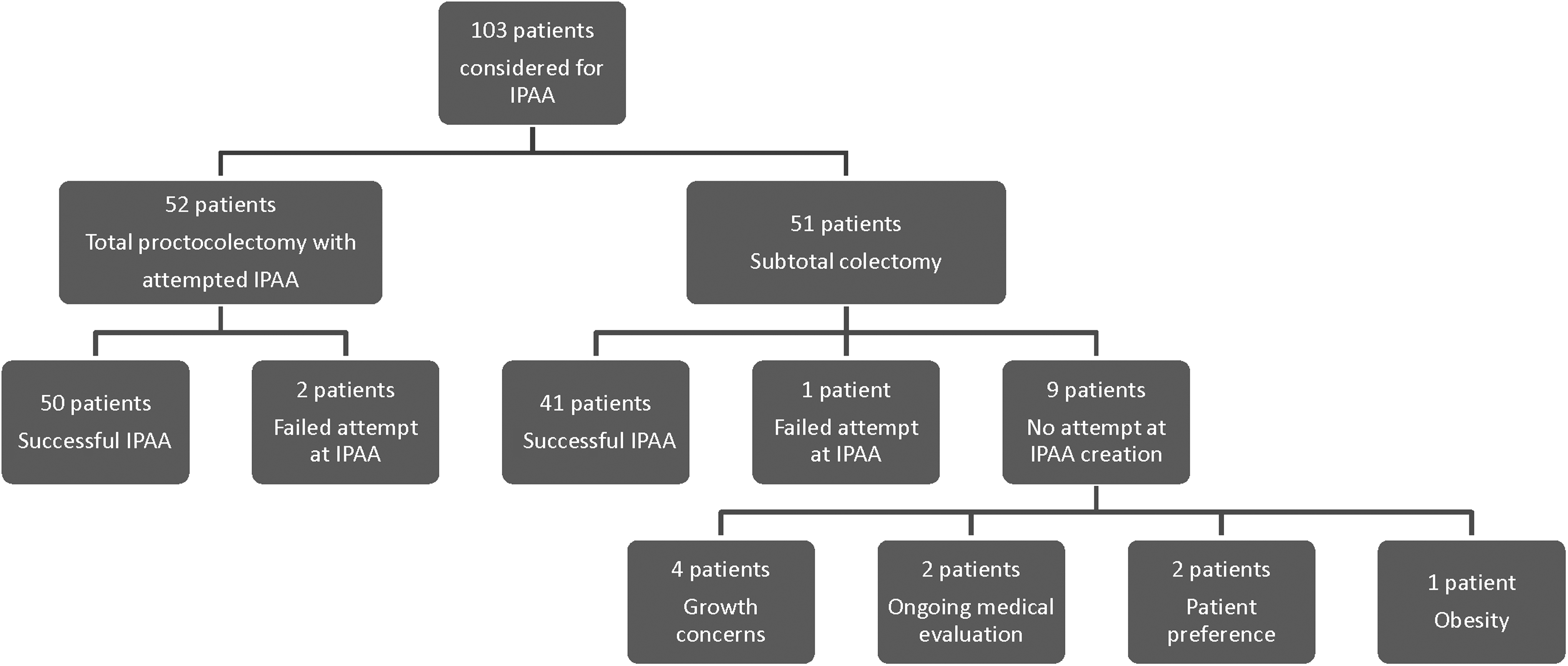
IPAA status for patients undergoing subtotal colectomy. IPAA, ileal pouch-anal anastomosis.
Of 94 patients who underwent attempt at initial IPAA creation, 91 (97%) had successful IPAA creation and 3 (3%) failed to reach. Two of these patients had FAP and underwent ileorectostomy instead. Operative reports in these patients have specific mention of patients' obesity (BMI percentiles: 88, 98) as the reason for inability to reach. The other patient had UC and underwent diversion after intraoperative pouch ischemia. There was no mention of obesity as the reason for the pouch ischemia, but BMI percentile for age and sex was 82.
In the 91 patients with successful IPAA, median age was 15 (range: 1.5–17) and 52 (57%) were female. IPAA creation was performed as part of a three-stage operation in 32 (35%), a two-stage operation in 29 (32%), one-stage operation in 21 (23%), and a modified two-stage operation, an IPAA without diversion performed after subtotal colectomy, in 9 (10%). A laparoscopic approach was successful in 75 (82%) with 4 (4%) conversions to open, and 12 (13%) planned open procedures. Seventy-one patients (78%) were normal weight, 14 were overweight or obese (15%), and 6 (7%) were underweight. The distribution of patients by BMI percentile-for-age-and-sex is shown in Figure 3.
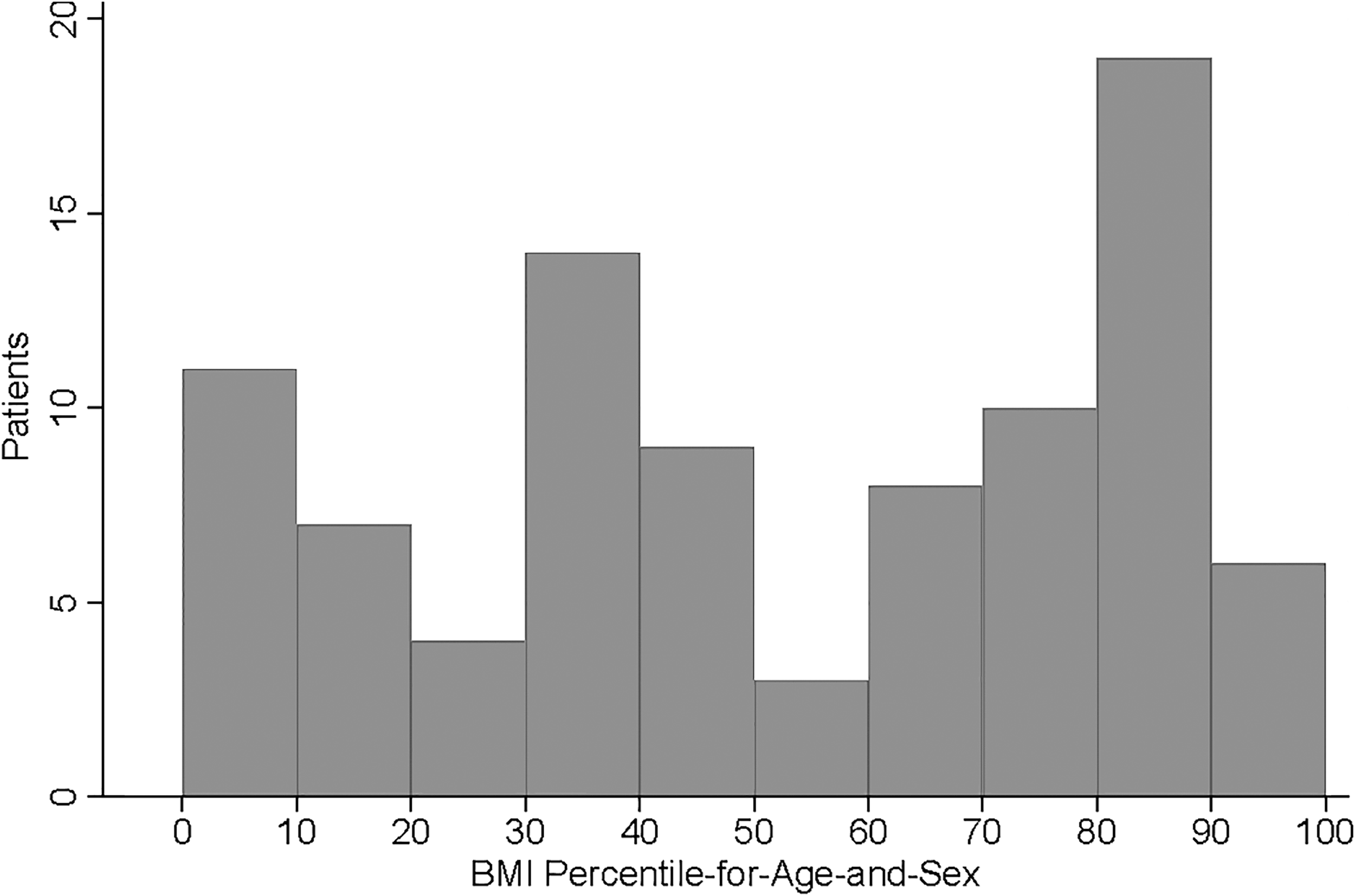
Number of patients across BMI deciles-for-age-and-sex. BMI, body mass index.
Sixty (66%) patients required maneuvers to lengthen the mesentery, and 26 (29%) required more than one maneuver. Maneuvers required included additional mobilization after a failed test of pouch length in 44 (48%), creation of mesenteric windows in 31 (34%), and artery ligation in 5 (5%). Among the 14 overweight/obese patients, 13 (93%) required maneuvers to lengthen the mesentery compared with 47 (61%) of 77 patients who were neither overweight nor obese (P = .03). On univariate analysis, there were no differences between patients who did and did not have maneuvers dictated in operative reports by age, sex, diagnosis, stage at IPAA creation, or surgeon specialty. Children who had maneuvers performed were significantly more likely to be overweight or obese than those without maneuvers performed (22% versus 3%, P = .021). There was also significantly higher median BMI percentile-for-age-and-sex for patients in the maneuvers group compared with those without maneuvers dictated (70 versus 35, P < .001) (Table 1). A positive trend for requirement of maneuvers existed across increasing BMI classification of underweight, normal, and overweight/obese (P = .02).
Univariate Associations for Utilization of Maneuvers
BMI, body mass index; FAP, familial adenomatous polyposis; IPAA, ileal pouch-anal anastomosis; IQR, interquartile range; UC, ulcerative colitis.
Being overweight/obese remained an independent risk factor for maneuvers (OR: 9.3, 95% CI: 1.04–82.75) after adjusting for age, sex, height, operative stage, and operating surgeon (Table 2). Area under the receiver operator characteristics curve was 0.78. For every 10 U increase in BMI percentile-for-age-and-sex, the odds of maneuvers being performed increased 1.34 times (OR: 1.34, 95% CI: 1.11–1.62) (Table 3). Increasing BMI percentile was associated with greater risk of maneuvers being performed (Fig. 4). Area under the receiver operator characteristics curve was 0.80.
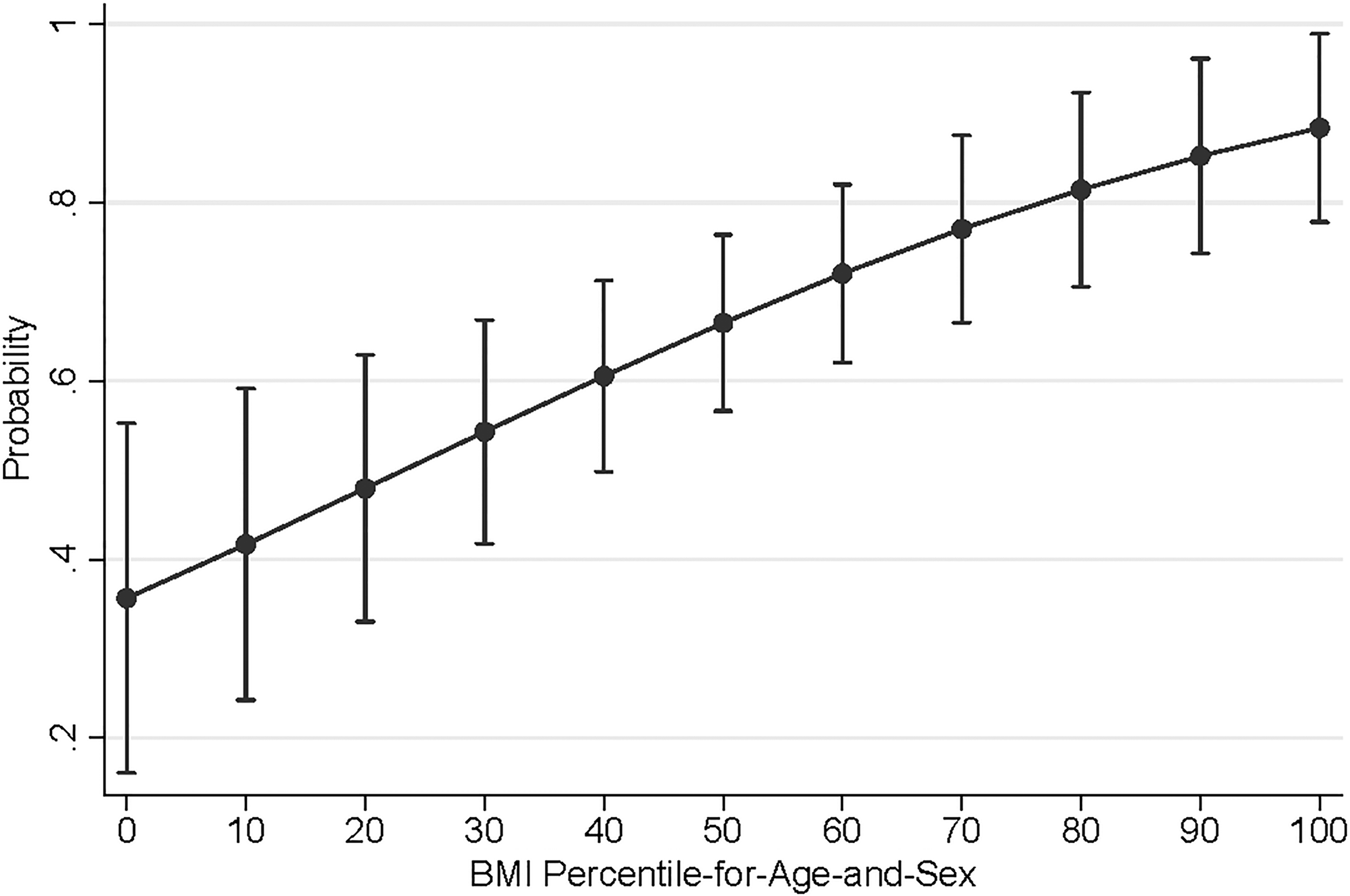
Adjusted probability of lengthening maneuvers.
Multivariable Model for Need for Maneuvers with Overweight/Obese as Binary Predictor
Multivariable Model for Need for Maneuvers with Body Mass Index Percentile-for-Age-and-Sex as Continuous Predictor
BMI, body mass index.
Despite maneuvers being necessary in the majority of patients, no difference was noted in operative times for completion of proctectomy operations, American Society of Anesthesiologists (ASA) score, operative blood loss, hospital length of stay, or 30-day maximum Clavien-Dindo scores (Table 4). Reoperation rates were 13% for patients with and 10% for patients without lengthening maneuvers performed (P = .73). Similar rates of reoperation were present for overweight/obese patients versus for normal or underweight children (8% versus 12%, P = .66). Only 2 (14%) of 14 overweight/obese patients experienced complications, compared with 30 (39%, P = .13) of 77 normal or underweight patients with no difference in maximum Clavien-Dindo scores (P = .45).
Operative Details and Complications for Those With and Without Lengthening Maneuvers
ASA, American Society of Anesthesiologists; IPAA, ileal pouch-anal anastomosis; IQR, interquartile range.
Discussion
Lengthening maneuvers are required in the majority of pediatric patients undergoing IPAA, and, in our series, overweight and obese patients were at even greater risk of requiring these advanced techniques when performing IPAA. Obesity further contributed to failure of pouch reach altogether resulting in permanent ileostomy or conversion to ileorectostomy in 2 patients. Fortunately, performance of advanced maneuvers did not adversely impact 30-day outcomes or long-term pouch failure. Surgeons need to be aware of the challenges of IPAA in overweight/obese patients.
Obesity has been shown to influence the operative timing and complexity in adults, and we have now demonstrated how it impacts operative complexity in pediatric patients. 10 Obesity was responsible for 2 of 3 failed IPAA attempts in our study. This is similar to studies in adults, which have cited obesity as key risk factor for both withholding IPAA and IPAA abandonment.11,12 In a study of 1175 adult patients who underwent proctocolectomy for UC, authors cited obesity as the sole reason for not offering IPAA in 18% of patients. Furthermore, they found that chance of an unsuccessful pouch rose from 2.0% at a BMI of 30 to 5.7% at a BMI of 35 and 15.0% at a BMI of 40. 12 The 2 FAP patients in our study converted to ileorectostomy due to obesity have a more significant lifelong health burden. Ileorectostomy for FAP mandates routine endoscopic surveillance, which must be emphasized in the obese population since obese individuals have disparate rates of health care for chronic conditions and cancer screening.13,14
It is critical to avoid postoperative complications and poor long-term functional outcomes by creating a tension-free anastomosis; and as we have shown, mesenteric lengthening is often necessary. Need for mesenteric lengthening in adults series has varied, with reported rates as low as 25% to as high as 77%.12,15 Surgeons employ a stepwise approach to minimize tension on the IPAA. 6 If the apex of the pouch reaches 3–4 cm below the inferior border of pubis after small bowel mobilization, this is considered adequate. If length is inadequate, creation of mesenteric windows, high ligation of the ileocolic artery, or ligation of the distal superior mesenteric artery can be considered (Fig. 1). Additional maneuvers have been described by Chu et al. such as preservation of the right colon marginal artery and the right branch of the middle colic artery with subsequent division of the right colic, ileocolic, and distal superior mesenteric arteries. 9 While this approach has been estimated to achieve >10 cm of length, it must be considered before colectomy. While maneuvers no doubt add additional complexity to the operation, they did not appear to significantly prolong operative times or result in more complications in our series. Still, operative times tended to be longer where maneuvers were needed for stage I and II operations—and this nearly approached significance. One explanation for such a trend is that a foreshortened mesentery increases the difficulty of both colectomy and IPAA; and the combination of both difficulties produced more pronounced difference in operative time. There could also be some mesenteric lengthening at the time of colectomy and subsequent stretching before IPAA for modified two- and three-stage patients.
While our study showed a significant association between maneuver utilization and children with increased BMI, it failed to show a difference in reoperation or complication rates between overweight/obese children and normal or underweight children. In contrast, Dukleska et al. reviewed 260 pediatric IPAA patients in the Pediatric National Surgical Quality Improvement Program (NSQIP-P) and found obesity to be an independent risk factor for reoperation on multivariable regression. 16 Their classification of obesity as BMI ≥30 is imperfect, in that it fails to account for the fluidity in height and weight growth during school age and adolescence. It is likely that their categorization of obesity underestimated the prevalence in the patient population; and thus it is unclear whether exclusion of additional patients would bias results away from the null. Their discussion points to obesity's association with and the technical challenges posed by foreshortened mesentery, reflected in our own findings of an association between maneuver utilization and obesity. On the one hand, our work showed that additional maneuvers due to foreshortened mesentery did not appear to increase the odds of reoperation or complications in general. On the other hand, the small number of events and obese/overweight patients may make our study underpowered to see the difference in complication rates between overweight/obese and normal/underweight children.
This study has several limitations. First, this is a retrospective review with a number of referred patients, limiting our ability to detect patients readmitted or with complications treated outside our system, though these patients are frequently transferred back or notify us of their complications. Second, there are a small number of patients in our overall study, and an even smaller number of overweight/obese patients. Common practice at our institution is to require obese children to lose weight before undergoing IPAA as it is a modifiable risk factor that affects risk of IPAA failure and operative complexity. Therefore, there may be some selection bias among those who remained overweight/obese at the time of surgery. Third, dictating practices vary between surgeons. Maneuver utilization by surgeon specialty was not different on univariate analysis, but this approached statistical significance. The most plausible explanation for this is differing dictation practices. Across the 14 different surgeons performing the represented operations, maneuvers may have been performed by surgeons yet not dictated. There remains, however, the possibility that colorectal surgeons have a different rate of maneuver utilization. Finally, BMI percentile-for-age-and-sex is an imperfect surrogate for obesity in children and may not reflect visceral obesity. BMI [and even BMI percentile-for-age-and-sex] in children can be misleading—A 2014 study found that shorter stature and higher muscle mass in children can lead BMI to slightly overestimate adiposity. Furthermore, reduced muscle mass due to low levels of physical activity or chronic illness leads BMI to underestimate adiposity in a substantial proportion of children. 17
Conclusion
IPAA is a technically challenging procedure that is further complicated by childhood obesity. Increasing BMI was associated with higher probability of lengthening maneuver utilization in children. Surgeons need to be prepared to perform mesenteric lengthening maneuvers when operating on all pediatric patients, particularly in overweight and obese pediatric patients to ensure minimal tension on IPAA. Whether these maneuvers have an impact on long-term pouch function is undetermined and deserves further study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.