
Abstract
Abstract
Introduction:
Children with pectus carinatum (PC) are particularly vulnerable to psychosocial effects of poor body image, even though they may not experience physical symptoms. Nonoperative treatment with orthotic bracing is effective in PC correction. We describe our experience with dynamic compression bracing (DCB) for PC patients and their satisfaction with bracing.
Materials and Methods:
Prospective institutional data of patients undergoing DCB from July 2011 to June 2018 were reviewed and analyzed for those who entered the retainer mode after correction, defined by a correction pressure of <1 psi. A telephone survey was conducted regarding their bracing experience and satisfaction with the outcome on a scale of 1–10.
Results:
Of 460 PC patients, 144 reached the retainer mode. Median time to retainer mode was 5.5 months. There was no statistically significant relationship between initial correction pressure or carinatum height and time to retainer mode (P = .08 and P = .10, respectively). Fifty-seven percent were compliant with brace use, and median time to retainer mode in this subset was significantly shorter than noncompliant patients (3.5 months versus 10 months, P < .001). Fifty-three percent responded to the survey 13 months [interquartile ratios 3, 33] after the last clinic visit. The main barrier to compliance with wearing the brace was discomfort (37%), while the main motivation for compliance was appearance (58%). All endorsed bracing as worthwhile, with 94% reporting a satisfaction rating of 8 or greater for the correction outcome.
Conclusion:
DCB is effective in achieving correction of PC in compliant patients. Regardless of time to retainer mode, patients reported high satisfaction with bracing.
Introduction
Pectus carinatum (PC) is an anterior chest wall deformity characterized by outward displacement of the sternum and/or ribs. 1 There are two major subtypes, chondrogladiolar and chondromanubrial, with the former being much more common than the latter. 2 While physiologic cardiac and respiratory symptoms are seen infrequently, some children can experience shortness of breath with exercise as well as reduced endurance.1,2 However, what seems to have the greatest impact on quality of life for patients with PC is the psychosocial effect leading to poor body image and low self-esteem.3,4 However, these have been shown to improve with correction of the defect. 5
Over the past 2 decades, there has been a shift from open repair of PC with excision of costal cartilages and sternal division to nonoperative management with compression bracing.6–8 This has been largely motivated by the morbidity of the operation, which has led to operative treatment of only the most severe cases of PC, leaving many patients untreated, but still affected by psychosocial effects that accompany the diagnosis.2,6,9
The concept of bracing is based on relative flexibility of the chest wall in children, allowing reshaping of the sternum and ribs by external compression.10–12 Proof of concept exists with the success of the Nuss procedure for pectus excavatum, which is, in reality, an internal brace. As bracing has gained popularity, it has now become the primary method of treatment, 8 and bracing protocols and techniques continue to evolve as we seek the optimal bracing program for PC patients.
In July 2011, we established the Center for Pectus Excavatum and Pectus Carinatum, providing comprehensive care for patients with all forms of chest wall deformities. 13 While there are variations in the types of braces and protocols used worldwide, we have had successful outcomes with dynamic compression bracing (DCB), as described by Martinez-Ferro et al. in 2008.9,14 We now describe the largest series of PC patients treated with DCB (who reached correction and completed our bracing program) in an effort to further elucidate the optimal bracing protocol that is associated with a successful outcome.
Materials and Methods
Following IRB approval (No. 15090404), we reviewed our prospectively collected data on PC patients treated with DCB at our Pectus Center from July 2011 to June 2018. Patients were included if they were older than 10 years of age and less than 18 years of age when they began bracing and had at least 4 months of follow-up.
Patients were braced with a DCB from Pampamed (Buenos Aires, Argentina) and underwent the bracing protocol we have previously described. 14 In brief, at the initial fitting, a pressure of initial correction (PIC), defined as the pressure needed to completely flatten the carinatum, was obtained and an initial treatment pressure was set to a tolerable psi, usually <2.5 psi, to minimize skin complications from external compression. Patients were instructed to wear the brace 23 hours per day, removing the brace for sports or bathing. They were also given instructions on an exercise program. They were brought back in 1 month and every 6–8 weeks thereafter for reevaluation and brace adjustments.
Between our previous report and this current one, only a single change was made to the existing bracing protocol, which consisted of defining the achievement of correction as reaching a correction pressure of <1.0 psi, instead of <0.5 psi. This was changed due to patients' reports of no improvement in appearance of the defect or physical symptoms by reaching a lower correction pressure of <0.5 psi. Recurrence was defined as a correction pressure of >1.0 psi after previously achieving correction. If patients had a recurrence in retainer mode, the patients returned to 23 hours of brace wear per day and continued clinical follow-up until they achieved correction. Once achieving correction again, they returned to reduced wear time with continued clinical follow-up.
Data collected included demographic information, PC description, relevant medical history, symptomatology, complications, time to retainer mode, compliance with bracing, and follow-up. Compliance was defined as adherence to the instructed wear time by wearing the brace at least 19 hours a day and at least 6 days a week.
We then conducted a telephone survey to assess patient experience with bracing. The survey consisted of questions regarding reinstitution of bracing at home and the number of weeks the DCB was worn, subjective personal observation of recurrence, limitations experienced when using the brace, motivations for bracing, whether the bracing program was worthwhile, and overall satisfaction with the outcome of bracing graded on a scale of 1–10.
Descriptive statistics were performed with categorical variables reported in percentages and continuous variables reported as medians with interquartile ratios (IQR). The outcomes of interest were time to retainer mode, limitations and motivations with wearing the brace, and satisfaction with correction outcome. The Mann–Whitney test for comparisons and a linear regression model for age, PIC, carinatum height, and months to retainer mode were performed using STATA® (StataCorp 2017, Stata Statistical Software: Release 15, College, Station, TX; StataCorp LLC), in which a P value <.05 was considered statistically significant.
Results
Of the 460 patients who have undergone DCB at the Pectus Center during the 7-year study period, 144 (31%) have achieved complete correction of the PC defect, entered retainer mode, and had at least 4 months of clinical follow-up. The majority of patients were male (91%) and the median age at initiation of bracing was 14 years [IQR 13, 15]. Additional demographic information is summarized in Table 1. The most common presenting symptom was pain at the site of the defect in 39.7% of patients. This was followed by respiratory symptoms described as shortness of breath, difficulty taking deep breaths, and/or exercise intolerance in 21.4%. No patient described cardiac symptoms such as palpitations, tachycardia, or bradycardia.
Patient Demographics for Those Who Completed Bracing
Values shown in brackets are frequencies or mediums (interquartile ratios).
Chondrogladiolar carinatum was the most common type of PC present in 98.6%, whereas chondromanubrial carinatum was present in only 1.4%. The defect was asymmetric in 52.4% of patients, with 33.6% located to the right of the midline. Median height of the carinatum was 2 cm [IQR 1.5, 3] and median PIC was 3.7 psi [IQR 2.9, 4.6]. There was a statistically significant relationship between the PIC and height of the carinatum, as seen in Figure 1 (P < .001, with a regression coefficient of 0.32, CI 0.15–0.49). Although we found no statistically significant relationship between the height of the carinatum and age (P = .46), we did find a statistically significant relationship between PIC and age (P = .02, with a regression coefficient of 0.18, CI 0.04–0.33).

Correlation of height of carinatum and initial correction pressure (P < .001, b = 0.32).
The median time to complete correction and transition to retainer mode was 5.5 months [IQR 3, 10]. We found no statistically significant relationship between PIC or height of the carinatum and time to retainer mode (P = .08 and P = .10, respectively). However, time to retainer mode increased with age, as seen in Figure 2 (P = .01, regression coefficient 1.28, CI 0.35–2.21). Fifty-seven percent of patients were compliant with brace use as instructed at each clinic visit. There was no statistically significant relationship between PIC or height of the carinatum and compliance (P = .52 and P = .58, respectively). We also found no statistically significant relationship between age and compliance (14 years [IQR 13, 14] compliant versus 14 years [IQR 13, 15] noncompliant, P = .09). The time to retainer mode was significantly shorter in compliant patients versus noncompliant patients (3.5 months [IQR 2, 6] versus 10 months [IQR 6, 13], P < .001).
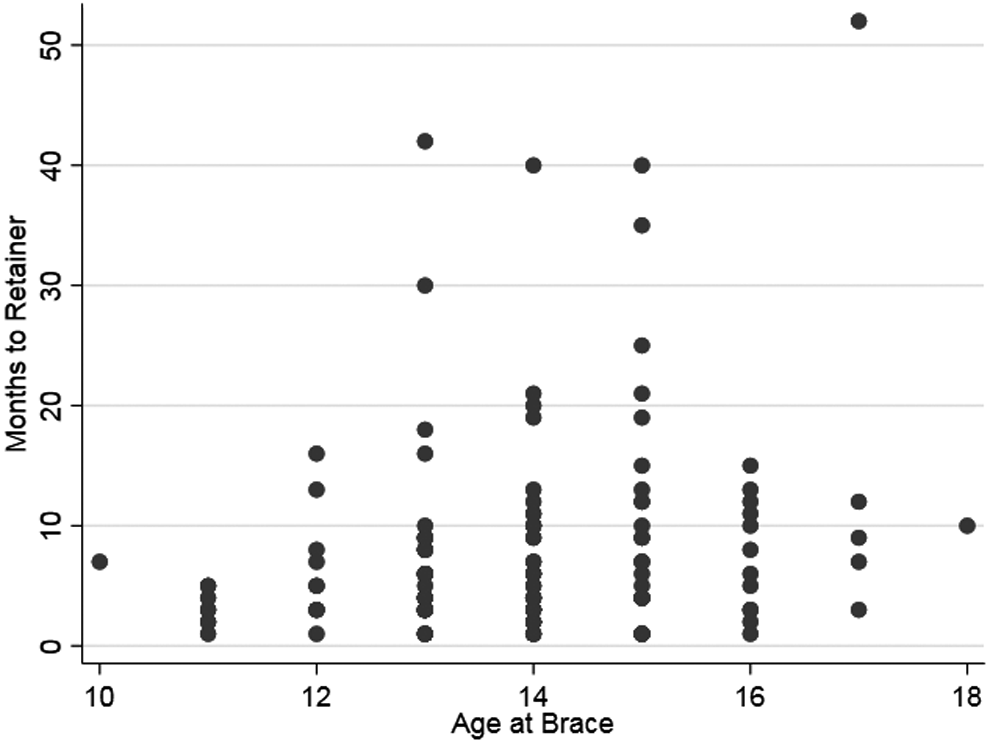
Correlation of time to retainer mode and age (P = .02, b = 0.18).
Median follow-up after entering retainer mode was 15 months [IQR 5, 21.5]. This was greater for compliant patients compared with noncompliant patients (16 months versus 14 months, P = .03). While 40% of patients had recurrence after reaching retainer mode, there was no statistically significant difference in recurrence when comparing compliant patients with noncompliant patients (P = .35). The median follow-up was longer in patients with recurrence (17 months [IQR 10, 25] versus 12.5 months [IQR 4, 21], P = .03). The only factor that was predictive of recurrence was PIC (Table 2).
Factors Associated with Recurrence of Pectus Carinatum
Complications of bracing consisted of skin changes such as erythema, acne, or breakdown without signs of infection in 13.9%, problems with fit such as tightness or pain in 13.9%, mechanical issues requiring readjustment and/or part replacement in 8.3%, and new onset or worsening of existing rib flaring in 4.9%. The majority of patients (59%) experienced no problems while bracing.
We attempted to contact all 144 patients for the telephone survey and 53% responded. Time from last follow-up clinic visit to completion of the survey was 13 months [IQR 3, 33]. Forty-two percent of patients reported wearing their brace after their last follow-up clinic visit. The median time of continued brace wear after follow-up was 10 weeks [IQR 6, 14]. Twenty-four percent of patients reported that they have noticed a minor recurrence, defined by reappearance of a small protrusion of the chest and/or recurrence of initial presenting symptoms before bracing. Seventy-six percent reported no recurrence of the defect or initial presenting symptoms.
When asked about limitations experienced while bracing, 38% reported discomfort with the brace, 14% reported feeling embarrassed to wear the brace in a public setting, 7% reported both discomfort and embarrassment, and 1% reported mechanical problems with the brace such as loose screws, broken clasps, or bending of the brace that prevented proper wear. Forty-two percent experienced no limitations with bracing. When asked about specific motivations for bracing, 59% sited physical appearance as their main motivation, while physiologic symptoms were the main motivation in 21%, and parental influence in 6.9% of patients. Fifteen percent of patients endorsed no specific motivation, but thought it should be treated because it was abnormal. All patients reported that going through the bracing program was worthwhile, with 94% of patients reporting a satisfaction score of 8 or greater on a scale of 1–10.
Discussion
In our study population, the median time to retainer mode was 5.5 months, but was dependent on compliance with brace use. We found that compliant patients had a significantly shorter time to retainer mode compared with noncompliant patients (3.5 months versus 10 months, P < .001). Our patient survey identified factors that may affect compliance, such as discomfort when wearing the brace and embarrassment when wearing the brace in public. Despite these limitations to brace use, we also discovered that 94% of patients were very happy with the correction outcome after bracing. This adds to the existing literature that external compressive bracing is effective in the treatment of PC.6,9–10,12,14–19
While several brace designs exist, the most well studied, and the one we use, is the DCB, which has been shown to be safe and effective in several studies.6,14 Despite this consensus, there is still debate over patient selection for bracing, the amount of daily wear, duration of treatment, and predictors of success and recurrence. Furthermore, data on long-term outcomes following completion of a bracing program are lacking in the existing literature.
DCB is performed with a modifiable brace adjusted based on a quantifiable variable (PIC) that allows adjustment of the brace with progression of treatment and growth of the patient.9,17 The PIC has become a variable of interest in several studies.9,10,14,17 In 2008, Martinez-Ferro et al. published their initial results using the DCB system in 208 patients, measuring the PIC in the last 107 patients and excluding those with PIC >7.5 psi. They found that patients with a high PIC had a longer duration of treatment. In another study that included 14 patients with PIC >7.5 psi, 8 patients achieved flattening of the sternum with the remaining 6 still in active treatment. 10 In our previous report, we found a low PIC to be a predictive factor for successful resolution of the carinatum defect. 14
In this current study, we found a statistically significant relationship between PIC and age, which was consistent with our finding that older children took longer to reach retainer mode. This confirms other authors' observations, where older age groups had higher PICs and lower correction rates, which may be due to increasing stiffness of the thoracic cage with age.8,9,18 Interestingly, our analysis of the PIC and time to retainer mode did not reach statistical significance, indicating that although PIC may play a significant role in correction of the defect, it is not the only factor contributing to the success or failure of DCB.
One factor that we know affects outcomes of bracing is patient compliance. This has been shown in several studies, with some claiming that compliance is the most important factor for success.12,20–22 In our study, 57% of patients were compliant with brace wear as instructed at each clinic visit. These patients took significantly less time to reach correction and enter retainer mode, on the order of a 6-month difference between the two groups. We found no statistically significant relationship between age, PIC, or height of the carinatum and compliance. Therefore, while PIC may be important for achieving correction of the defect, compliance may determine the time it takes to reach retainer mode.
In our follow-up survey, we found that the greatest limiting factor to brace wear was discomfort with the brace in almost 38% of patients. Most reported that the discomfort was mild and only in the initial weeks of bracing or when sleeping with the brace in place. This limiting factor is similarly reported in other studies.23,24 Although it seems to be common among patients, it does not seem to be a major limitation that prevented them from completing therapy, as most reported the resolution of discomfort within the first month of bracing. This is supported by literature reporting that pain or discomfort experienced with bracing does not have an influence on compliance.22,24
There is a paucity of data related to recurrence rates and factors that affect recurrence after bracing, mostly due to the lack of long-term follow-up studies. In this study, we report a recurrence rate of 40% once in retainer mode after reaching initial complete correction. These recurrences were defined objectively by a measured correction pressure of >1.0 psi. Most recurrences were mild, resulting in correction pressures just over 1.0 psi and none returning to their original PIC. When recurrence was diagnosed, patients were instructed to return to wearing the brace for 23 hours per day until their next follow-up appointment. Once they achieved correction again, usually by their next appointment 6–8 weeks later, they returned to the reduced brace wear time. Interestingly, there was no statistically significant relationship between recurrence and compliance. However, there was a statistically significant relationship between PIC and recurrence, with a higher PIC observed in patients with recurrence.
There was no difference in age or height of the carinatum in patients with recurrence versus those without. Bracing duration was significantly longer in patients with recurrence, as indicated by the longer follow-up period after reaching retainer mode in this group. Compliant patients also had significantly longer follow-up than noncompliant patients. These findings suggest that not only does PIC play a role in achieving correction but that it might also play a role in maintaining correction, whereas compliance may shorten the time to achieve correction, but not necessarily duration of treatment.
Since compliance is the main determinant of success, some authors are exploring variations of this protocol in an attempt to improve compliance rates. A recent report proposed a less intensive protocol where daily wear was only 8–12 hours per day. 25 Although the brace used was a noncustom fitted brace and not a dynamic compression brace, 15 patients of 32 with adequate follow-up were successful in achieving correction at a median of 9.6 months with a 93.8% compliance rate. 25 While they were successful in achieving high compliance, time to correction was greater compared with our study. They did not comment on duration of bracing, so it is not known whether the decreased daily wear time contributes to longer overall duration of treatment or if there is no difference. This could be elucidated in future studies with longer follow-up.
In our follow-up survey, 24% of patients reported a mild visual recurrence of the carinatum defect, which was easily treated with limited self-bracing. Regardless, all patients surveyed reported DCB as worthwhile and 94% of patients rated their satisfaction with the outcome greater than 8 on a 1–10 scale.
There are limitations to our study. First, these data are from a single site, evaluating a limited subset of PC patients who have completed bracing. The smaller subset likely drove some analyses toward insignificance. For example, the relationship between PIC or carinatum height and time to retainer mode approached statistical significance with P values of .08 and .10, respectively, so it is likely that these would reach significance with more patients in the study. However, this is the largest reported series of PC patients who achieved correction with DCB.
Another limitation is the subjective measure involved with determining correction of the defect with bracing. We used a correction pressure of <1.0 psi as an objective measure to determine correction and the ability to transition to retainer mode. However, retainer mode was not entered unless there was also mutual agreement between the patient and provider that the chest was in a subjectively acceptable neutral position. This means that if the patient did not find the chest appearance acceptable, even with a correction pressure of <1.0 psi, the patient did not have to enter retainer mode. This could have affected the time to retainer mode, duration of bracing, and length of clinical follow-up.
A well-known limitation with bracing for PC is the issue of compliance with brace use. As in many other studies, we found compliance difficult to accurately measure and it was reliant on patient reporting, which is potentially fraught with bias. Efforts are being made to better monitor and incentivize compliance with real-time data monitoring, and while preliminary results of these systems are encouraging, studies in a large patient population have yet to be done. 26
Nevertheless, we found that DCB for PC is effective in achieving early correction in compliant patients. Regardless of time to retainer mode and duration of treatment, patients reported high satisfaction with their outcome. Expectations and possible outcomes should be communicated to patients and treatment should align with their own goals.
Footnotes
Acknowledgments
The authors would like to thank clinical research coordinators, Yara Duran and Pete Muenks, for their assistance with this study.
Disclosure Statement
No competing financial interests exist.