
Abstract
Background:
Common bile duct (CBD) injury is one of the most serious complications of laparoscopic cholecystectomy and carries an incidence of 0.3%–0.7%. Recently indocyanine green (ICG) fluorescent cholangiography (FC) has been used as an adjunct to identify the biliary tract during adult laparoscopic cholecystectomy, allowing intraoperative identification of biliary anatomy. The objective of this article is to show its successful use in pediatric laparoscopic cholecystectomies.
Method:
From July 1, 2017, to November 30, 2018, surgeons at John R. Oishei Children's Hospital and Women and Children's Hospital of Buffalo have been utilizing ICG-FC as an adjunct in patients undergoing laparoscopic cholecystectomy. Thirty-one patients undergoing laparoscopic cholecystectomy had 1 mL of dilute ICG (2.5 mg) injected intravenously in the operating room (OR) before trocar placement.
Demographics, intraoperative details, and subjective surgeon data were recorded for elective laparoscopic cholecystectomy cases involving ICG. We hypothesize that use of ICG-FC in the pediatric and adolescent patient population is a safe, reliable, and reproducible adjunct for identification of the biliary tree. Secondary outcomes were to identify rate of biliary anatomy identification, utilization ease, and operative times while using ICG technology in pediatric patients.
Results:
ICG-FC was used in 31 pediatric laparoscopic cholecystectomies performed by 5 surgeons at our institution. Ages ranged from 6 to 18 years. In all cases, the cystic duct–CBD junction was visualized while performing dissection of the triangle of Calot. No intraoperative complications occurred.
Conclusions:
ICG-FC provides a noninvasive real-time visualization of the extrahepatic biliary tree in children and adolescents. We demonstrate that ICG-FC can successfully be used as an adjunct in pediatric patients and has the potential to facilitate with the dissection and minimize risk of bile duct injuries during pediatric laparoscopic cholecystectomies.
Introduction
Various methods have been described to help better identify the biliary tract anatomy intraoperatively with the goal of reducing the incidence of common bile duct (CBD) injury. 1 Bile duct injury incidence is 0.3%–0.7%.1–6 This prompted surgeons to search for reliable adjuncts and methods to safely avoid bile duct injury while performing a pediatric laparoscopic cholecystectomy. The adult literature highlights the use of indocyanine green-fluorescent cholangiography (ICG-FC) and its validity as a safe and easy to perform and interpret adjunct during minimally invasive surgery while visualizing the important structures of the extrahepatic biliary tract.7–11
Materials and Methods
Patients
Patients undergoing laparoscopic cholecystectomy by 5 surgeons at John R. Oishei Children's Hospital from July 1, 2017, to November 30, 2018, had their laparoscopic cholecystectomy performed with the use of ICG-FC technology. Inclusion criteria were patients <19 years old with a history of symptomatic biliary disease (chronic cholecystitis, symptomatic cholelithiasis, and biliary dyskinesia) as well as acute cholecystitis and cholangitis. Patients who were pregnant, breast feeding, cirrhotic patients, or those allergic to iodine or shellfish were excluded. The study was approved by the Institutional Review Board.
Operative technique
As a source of fluorescence, ICG was injected intravenously in the operating room (OR) after anesthesia induction and before surgical incision. ICG comes in a vial of 25 mg and must be diluted with 10 mL of sterile water, and then 1 mL of the solution is injected intravenously. The timing of ICG injection was selected because our pediatric patients typically do not have an IV cannula placed until they are in the OR suite. In addition, ICG is excreted into the bile within minutes after intravenous injection, reaching a maximum absorption peak within 2 hours. 12 Patients were monitored for any signs of allergic reaction to the dye.
Using the Stryker Infrared Fluorescence (IRF) Imaging System (Stryker Endoscopy, San Jose, CA), ICG-FC was performed. This is an investigational endoscopic illumination and imaging system for high-definition visible light and near-IRF imaging. We routinely use a 5 mm 30° AIM™ laparoscope, an IRF light source, light cable, camera control unit, camera head, a coupler, and surgical display unit. Surgical laparoscopic cholecystectomy was performed by obtaining the critical view of safety. 13 Throughout the operation during the dissection, the surgeon switched between standard camera views to those with ICG-FC to more definitively identify the biliary tree anatomy. Use of ICG-FC to detect the cystic duct (CD), common hepatic duct (CHD), CD–CHD junction, right and left hepatic duct junctions, and accessory hepatic ducts was relatively easy and did not require any additional ports or instrumentation in contrast to if the surgeon were to perform a conventional intraoperative cholangiogram (IOC) (Fig. 1). The CD was clipped using Weck® Teleflex® clip appliers with two clips proximal from CBD take off and one to two clips distally. The cystic artery was slowly cauterized using hook electrocautery and the gallbladder was then removed from the gallbladder fossa with hook electrocautery and removed from the body using an endocatch bag. The liver bed was then examined for hemostasis. The ICG-FC view was then obtained and the anatomy reidentified, confirming that the CBD and CHDs were uninjured.
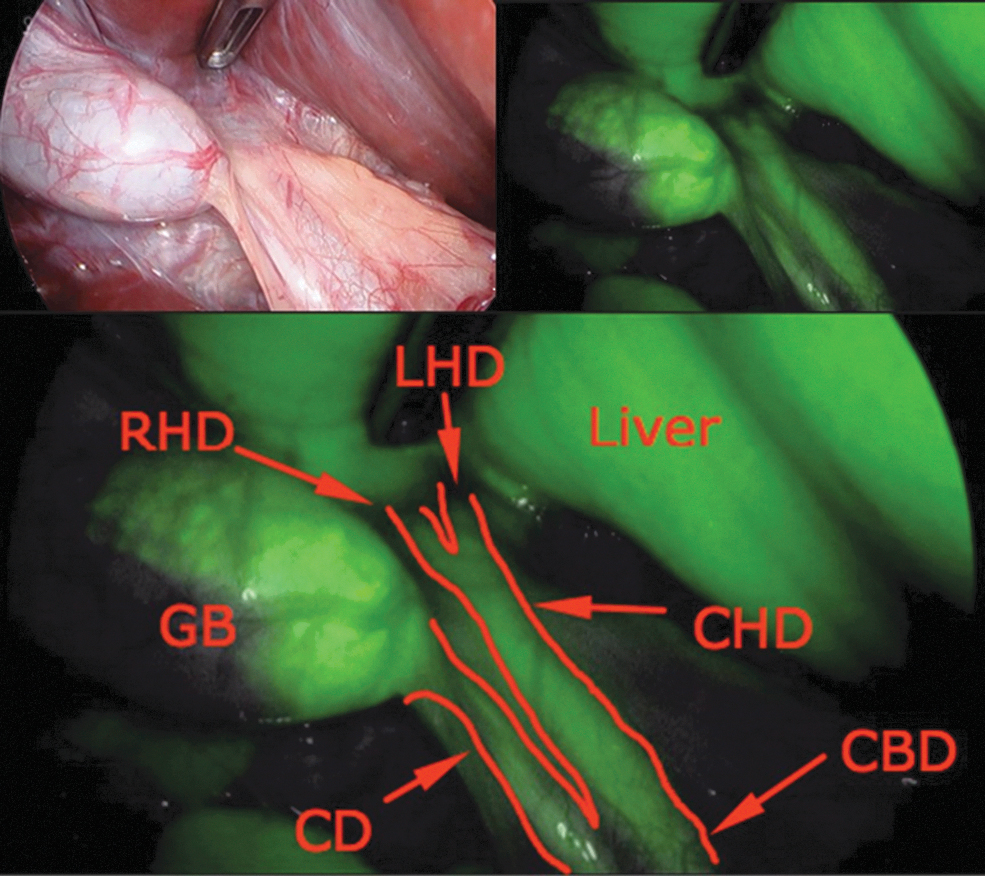
Laparoscopic view (top left), ICG-FC view (top right), and ICG-view with labels (bottom). CBD, common bile duct; CD, cystic duct; CHD, common hepatic duct; FC, fluorescent cholangiography; GB, gallbladder; ICG, indocyanine green; LHD, left hepatic duct; RHD, right hepatic duct.
Data collection
Demographics, intraoperative details, and subjective surgeon data were recorded for laparoscopic cholecystectomy cases using ICG-FC. ICG-FC use was confirmed by billing charges, anesthesia documentation, and operative dictation.
Results
Thirty-one pediatric patients had a laparoscopic cholecystectomy with ICG-FC between July 1, 2017, to November 30, 2018, at John R. Oishei Children's Hospital and Women and Children's Hospital Buffalo based upon billing codes, anesthesia, and operative record confirmation. Forty-two patients met inclusion criteria, however, only 31 were included in the study. Eleven patients were excluded due to inadequate documentation regarding ICG-FC use.
Mean age and BMI were 15 years and 26.4 kg/m2, respectively. Based upon their BMI, 1 patient was underweight (<18.5 kg/m2), 16 patients were ideal weight (≥18.5–24.9 kg/m2), 9 were overweight (≥25–29.9 kg/m2), and 4 were obese (≥30 kg/m2). Of the obese children, 2 were classified as morbidly obese (BMI >40 kg/m2). In total, 83.8% of patients were females and 16.1% were male. Indications for surgery included biliary dyskinesia (13), symptomatic cholelithiasis/biliary colic (6), choledocholithiasis (4), prior acute cholecystitis treated nonoperatively (3), biliary hyperkinesia (3), cholangitis (1), and chronic cholecystitis (1).
There were no associated complications, no major complications, and no patients experienced an allergic reaction to ICG injection. Of the 5 surgeons from our institution performing laparoscopic cholecystectomies, none reported bile duct injury within the past 5 years, with or without ICG-FC. While utilizing ICG-FC, none of the surgeons identified CBD stones, nor was this the goal of this study. This technology is not well suited for identifying CBD stones as the distal portion of the CBD is obscured by pancreas and duodenum and much of the distal bile duct is not exposed during routine cholecystectomy. Unless a stone is obstructive, the ICG will flow around the stone and may not create a shadow to be visualized.
We believe that ICG-FC is time efficient and easy to perform. The average OR time of the 31 cases completed with ICG-FC was 105 minutes and the average patient length of stay was 18 hours. This was compared with cases performed by the same 5 surgeons before their use of ICG-FC over a similar time period of 17 months, February 1, 2016, through June 30, 2017. The average time of laparoscopic cholecystectomy was 121 minutes for 68 cases. When surgeons performed laparoscopic cholecystectomy utilizing IOC, the average surgical time was 164 minutes for 10 cases, compared with 105 minutes that it took to perform laparoscopic cholecystectomy with ICG-FC.
When comparing same day surgical cases, the average cost per case for the ICG laparoscopic cholecystectomy cases is $6,820, whereas the average cost per case for laparoscopic cholecystectomy cases without ICG is $6,697. Inpatient surgical cases have other associated costs that may skew data, therefore, we chose to look at cost for same day surgical cases.
Based upon review of the operative reports, ICG-FC successfully visualized the CBD and the hepatic duct in all 31 patients.
Discussion
In 1995, Strasberg described the critical view of safety as a way to reduce injury while performing laparoscopic cholecystectomy. 8 Additional adjuncts such as IOC and intraoperative ultrasound have been used to identify and intraoperatively manage CBD stones. Surgeons have identified themselves as “routine” or “selective” IOC performers pending their daily practice habits. The disadvantages of conventional radiographic IOC include radiation exposure, higher costs, requirement of performing an incision resulting in increased incidence of bile duct injuries, and prolonged operative time.9–11
ICG is excreted into the bile and that protein-bound ICG emits light with a peak wavelength at ∼830 nm when illuminated with near-infrared light.12,13 ICG-FC has several potential advantages over radiographic IOC. ICG-FC has shown promising results in delineating biliary anatomy, even before dissection of Calot's triangle, without requiring a ductotomy or insertion of catheters for injection of contrast material into the biliary tree,11,14 potentially leading to decreased risk of biliary tract injury.
An additional advantage of ICG-FC is that it does not require radiation exposure of traditional IOC and no longer requires assistance of a radiation technician. This is beneficial to the pediatric population wherein we try to limit radiation exposure.
Although ICG-FC is helpful in identifying biliary tract anatomy, it should not be used and is not reliable for identifying stones in the biliary ductal system. The surgeons agree that if there is intraoperative concern for CBD stones, a fluoroscopy cholangiogram should be obtained.
ICG-FC does carry small risk of anaphylactoid reactions after ICG injection. These reactions have been reported at ∼0.003% at doses in excess of 0.5 mg/kg; however, literature suggests that the reaction is a dose-dependent pseudoallergic mechanism, rather than a true immune mechanism. 15 Our institution adheres to the general recommendation that ICG not be used for patients with a shellfish allergy or iodine contrast sensitivity. In all cases, the single dose of 2.5 mg was adequate in all age groups to delineate the biliary tree. In addition, there is still continued risk of injury to biliary structures despite the use of ICG-FC. Although ICG-FC may improve safety when performing pediatric laparoscopic cholecystectomy, it is important that surgeons still continue to rely on basic surgical principals for identification of the biliary structures so as not to be misled by ICG-FC.
Primary aims of this study were to evaluate the safety, feasibility, reliability, and reproducibility of ICG-FC in the identification of extrahepatic biliary anatomy during laparoscopic cholecystectomy in the pediatric population. Secondary aims were to assess the benefits of using ICG technology specifically with regard to operative time and complication rates. Our results of this study are congruent, although we believe that we would need further investigation with a larger sample size to make a definitive conclusion. In adults, Dip et al. showed that the variable cost of using an IOC to that of using ICG-FC was an average cost of $778 for IOC, compared with $14.10 for ICG-FC (p = 0.001). 14 Dip et al. additionally showed that ICG-FC saves costs by decreasing OR time and time under anesthesia. In our comparison groups, when cases were limited to same day surgical patients, we found that cases with ICG-FC cost slightly more than those without ICG-FC. These results do not take into account whether or not an IOC is performed; therefore further analysis is warranted.
Our study is not without limitations. Since we are the first to publish data on utilization of ICG-FC in the pediatric population, we are limited by a small sample size from a single institution. We believe that ICG-FC technology is an effective adjunct while performing laparoscopic cholecystectomy and that the technology is easy to use and improves operative time and costs.
Conclusions
We recommend use of ICG-FC as an adjunct to performing pediatric laparoscopic cholecystectomy. ICG-FC is a noninvasive real-time visualization of the extrahepatic biliary tree in both pediatric and adult patients. Although ICG-FC may improve safety while performing pediatric laparoscopic cholecystectomy, surgeons must still continue to rely on basic surgical principals for identification of the biliary structures so as not to be misled by ICG-FC. Use of ICG-FC as an adjunct provides an additional safety stop on a procedure that continues to have risks of biliary injuries. We plan to implement this technology on future cases and collect further data.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.