
Abstract
Abstract
Background:
Most residents do not have a defined program for simulation training in video surgery in Brazil. The training takes place for the most part in vivo or in short courses. The goal of this article is to describe and evaluate a set of exercises using low-cost materials, created by the residents themselves, to enable basic skills training in video surgery.
Materials and Methods:
Seven exercises were elaborated aiming to simulate main maneuvers performed in video surgery. The residents were guided by a written and video description showing the execution of the exercises, performed the exercises, and answered a questionnaire. After 3 weeks of free training, the residents performed the exercises and answered the questionnaire again.
Results:
Seven residents started the study; however, 6 completed the two steps. Among the participants, 83% received in vivo video surgery training, and only 2 (33%) received some supervised simulation training in minimally invasive surgery before this time. All participants considered the set of seven exercises representative of the actual skills in video surgery. There was no difficulty in acquiring the materials or in assembling them to carry out the training. All the participants had a shorter training time than initially proposed, on average 1 day/week for 20 minutes.
Conclusions:
A simple set of exercises can be elaborated by the residents themselves and make feasible the simulated training in video surgery even without the availability of sophisticated and expensive materials. The presence of a tutor and the scheduling of exclusive training seem necessary for more satisfactory results.
Introduction
The increase in the use of minimally invasive surgery has made the training of specific skills in video surgery essential for the training of a surgeon. Progressively, pediatric surgery procedures have been performed by endoscopic techniques, with several publications showing similar or superior results to the conventional technique.1–7
The simulation allows the learning and training of the skills in video surgery in a controlled environment, being recently considered a foundation for the training of the surgeon in minimally invasive techniques. Its use results in a better performance of the surgeon in the procedures, collaborating for greater safety and better results to the patient. 8
Training boxes with different exercises and models that use synthetic or natural materials, as well as sophisticated realistic simulation programs, are examples of resources available for simulated training. However, simulation in video surgery seems to be insufficient or even absent in most pediatric surgery residency programs in Brazil, often due to the high cost of the material necessary to enable this kind of training in a simulated environment. Most residents have little theoretical and practical training in video surgery during their preparation. When training is performed, it occurs predominantly in vivo, and in few procedures when compared with conventional techniques.9–11
The lack of learning and training, with repetition of specific movements in a safe simulation environment, implies a significant increase in the operative time, exposing the patients to a greater risk of injuries, operative and postoperative complications, and, consequently, the costs of the service.9,10,12–14
The goal of this article is to describe and evaluate a set of simple exercises, created by the residents themselves, using materials of low cost, for training of basic skills in video surgery, in addition to evaluating the pediatric surgery residents' adherence to the proposed training program.
Materials and Methods
The study was carried out at the Hospital Pequeno Príncipe (HPP)—Curitiba, Paraná, Brazil, with the participation of 7 residents linked to the Pediatric Surgery Service of this same hospital and supervision of members of the pediatric surgeons group.
A simple set of equipment was used, such as an Everfocus analog security camera adapted to a Perimed “black box” and LCD AOC® television, laparoscopic forceps (grasping, Maryland, needle holders, and scissors), and disposable materials, typical of the hospital environment.
This set in the room of the department of pediatric surgery remained with available and unrestricted access to the surgeons' assistants and residents to carry out the proposed exercises.
Seven exercises were developed by the resident group to simulate maneuvers representative of the basic skills of video surgery, using simple materials available at the hospital. The seven exercises are described in text form in Table 1, illustrative images in Figure 1, and illustrative videos.*

Illustrative photos of the seven proposed exercises (1—space depth, 2—video surgery knot, 3—sliding knot ready, 4—extracorporeal sliding knot, 5—stitches, 6—bag glove finger, 7—circular incision with scissors).
Description of Proposed Exercises
After signing a consent and confidentiality agreement, the participants performed the seven exercises in a self-applied way with detailed description in text and video. They filled out a questionnaire about the specific training in video surgery that they had until then, what kind of resources they used for learning their current abilities in surgery residency with or without the use of simulation, in addition to their opinion about the proposed exercises, time to execute them, degree of difficulty, and time that they intended to have for training before the next stage of the study (3 weeks).
After 3 weeks of individual training, they performed the same seven exercises self-applied anew and filled out the same questionnaire about their opinion about the proposed exercises, time of exercise execution, and degree of difficulty.
The participants were repeatedly reminded to perform with precision, care, and delicacy the proposed exercises, without any concern for time or competition between them.
The data were arranged and analyzed in a descriptive way, in graphs and tables. Statistical analysis used Google® cloud programs (mean, median, standard deviation, minimum, and maximum).
The research was reviewed and authorized by the research ethics committee of the HPP, CAAE: 02771318.3.0000.0097.
Results
Of the 7 residents of pediatric surgery who started the study, 6 completed all steps.
Among the participants, 83% answered in the initial questionnaire that they had received in vivo video surgery training during the medical residency programs they participated in, and only 33% of them received some specific simulation training supervised in video surgery during the same period. Simulation training without supervision or complementary courses outside the residence program were performed by 83% and 50% of the participants, respectively.
Other forms of learning and training in video surgery used by the participants were media resources and telemedicine (websites, online, or shared videos). Eighty-three percent of the participants constructed some knowledge in video surgery from these instruments.
In the analysis of the exercises, the seven exercises prove to be easy to understand through explanations by text and video. All participants evaluated the seven exercises as representative of the technical skills required in video surgery. The exercises 2—knot, 3—sliding knot, and 4—extracorporeal sliding knot were considered the most representative. The exercises that required more skills for execution were the exercises 2—knot, 5—stitches, and 7—incision with scissor exercise, the latter being considered the most difficult by the participants.
The main results are summarized in Table 2.
Main Results
The values are represented in minutes:seconds.
Respectively, 1 and 2 participants could not perform the exercises 2—knot and 7—incision with scissors exercises in the pretest. After 3 weeks of training, all of them presented a subjective overall improvement in performance as shown in Figure 2, and were able to perform all seven exercises.
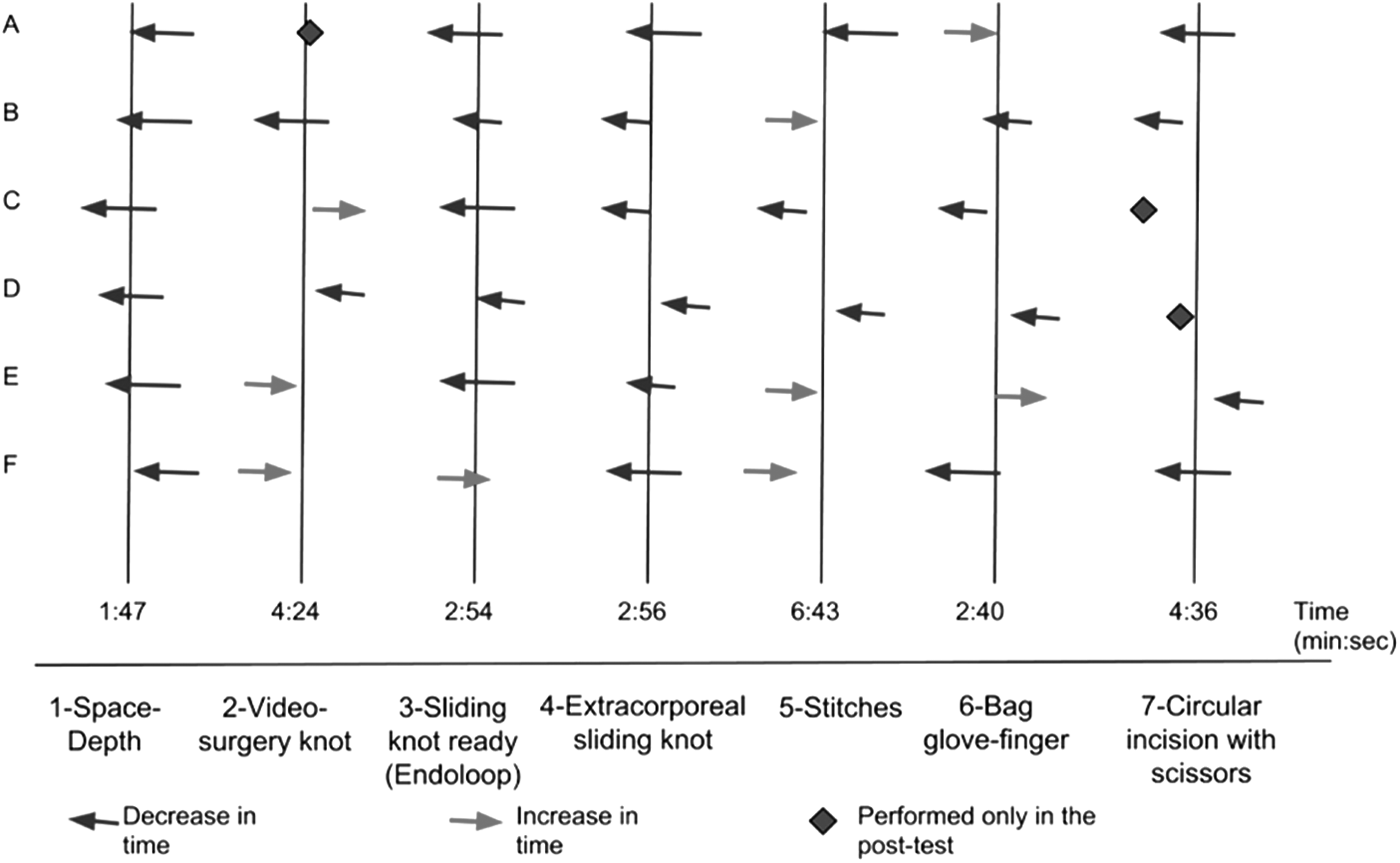
Illustration of the candidate times in relation to the time averages of each exercise.
The participants planned to devote on average 2–3 days/week, 30 minutes/day for the next 3 weeks after the first step, but the training time was free, independent, not protected during the residence program, and without a tutor surgeon supervision. That is probably why all participants engaged less training time than initially proposed, on average 1 day/week for 20 minutes.
There were no reports of difficulties in acquiring the materials or assembling them to accomplish the exercises.
Discussion
All participants classified the set of exercises as representative of the actual skills and technical difficulties of video surgery. This uniform opinion suggests that this set of seven exercises can be used for individual training, and may compose an initial simulated training program in video surgery for pediatric surgery residents of this service. The construction of exercises with common materials and accessible in the routine of the hospital made possible and facilitated the simulated training in video surgery, even with few financial resources.
Three forms of simulation for video surgery learning are currently used in the literature: exercises in “black box” training, as in this study, training in animals or corpses, and training in devices with virtual reality programs. Among these options, Zendejas et al., in a meta-analysis carried out in 2013, found that the “black boxes” are the simplest and cheapest models with learning results equal to or above the other forms cited.
Only 33% of residents in this group received supervised simulation training in video surgery during residency programs before the moment of this study. The low percentage can illustrate how the simulation has been underutilized for teaching surgery in our country. In most pediatric surgery residency programs in Brazil, there appears to be no simulation program that allows the resident to understand and exercise the technical skills of video surgery before they are used directly in patients. One of the factors most pointed to this deficiency and the financial issue is the lack of specific materials designed for simulation and lack of time of the residence preceptors designed for this purpose.
In services with a medical residency where the simulation is present, there seems to be no supervisor to teach, supervise, and evaluate the acquisition of these skills in video surgery. The high utilization of individual initiatives among the participants reinforces this hypothesis. Simulation training without supervision (83%), complementary courses outside the residency program (50%), and telemedicine resources (83%) were the alternatives reported by residents to fill this gap in the teaching of video surgery.
Simulated education should be the basis for training in video surgery, since it allows better knowledge of operative times, learning and training of the technical skills required for the procedure. 8 Therefore, it is especially important in the surgical procedures for low-incidence diseases, such as congenital malformations, minimally invasive neonatal surgery specific to pediatric surgery, and including fetal surgery recently.9,10,13,15,16
Specific models for simulation of the treatment of esophageal atresia, duodenostomy, pulmonary lobectomy, and diaphragmatic hernia repair through video surgery have been performed and described in the literature. Short courses at specific congresses or simulation centers are useful for adding knowledge and learning some skills, but not for consolidating them effectively and safely in the long run, which requires continued training. Lack of continued training over the course of months rapidly regresses the skills learned. Therefore, continuous simulated training in video surgery is the best way to maintain the proficiency of these skills.9,10,15
Low-cost simulation models have been described to stimulate simulation training in specific skills and specific procedures, including telementoring technology as an option to help a less experienced learner from a remote location. 17
Data show that simulation is most effective when within a 6-month-to-1-year program based on training and assessments with present monitoring and well-defined objectives in a competency-based education model. Programs organized in this way seem to be associated with better learning, improved performance, and greater retention of acquired skills.8,13,14
All participants spent less training time than planned and recorded on the first questionnaire. The main factors considered to justify the low time spent in the proposed training were the great amount of activities in the day life of the residence and the lack of an exclusive schedule for the exercises within the medical residency program. The absence of a preceptor dedicated to directly supervising the training also seems to have contributed to a lesser adhesion of the residents.
This study represented a joint effort of preceptors and residents to improve the learning and skills in video surgery through the simulation. The set of seven exercises created by the residents and the methodology of their employment allowed the Pediatric Surgery Service of the HPP to begin planning to introduce a simulation program in video surgery, to evaluate the level of knowledge in video surgery of the residents, and to know the limitations to this training.
All the residents indicated a subjective improvement in the execution of the exercises in the interval of 3 weeks, even though they did not perform the training as initially planned. This perception served as an incentive and aroused the interest of the residents and of the pediatric surgery team in advancing progressively in the field of training and simulation, through elaboration of new exercises, investment in other materials, and structure for the teaching–learning of pediatric video surgery.
The impact of this study was subjectively evaluated by residents as an initial step for a simulation program. An objective instrument should be created for assessment and document specific skills before and after training for various periods of time. A structure evaluation could show how much the set of seven exercises proposed can contribute for performance improvement in future studies.
Conclusion
A simple series of exercises with low-cost materials can be easily elaborated and make an initial video surgery simulation program feasible without the need for large financial investments and sophisticated equipment for this purpose.
The presence of a tutor and the scheduling of exclusive hours for the simulated training seem to be necessary for more satisfactory results.
A study with a larger number of participants, longer follow-up time, and an objective instrument for assessment of specific skills are necessary to evaluate whether there is a real improvement in residents' performance after training with this series of exercises, as well as to compare it with other video surgery simulation exercises already described in the literature.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.