
Abstract
Abstract
Background and Aim:
Training programs for developing laparoscopic suturing skills range from dry-box training to virtual simulator training. There are advantages and disadvantages to each training method; however, which training is best for medical students and young surgeons is unclear. The aim of this study was to compare the proficiency of medical students in acquiring laparoscopic suturing skills after various routes of short-term training: via a video, an expert teacher, or a virtual simulator.
Materials and Methods:
Seventeen medical students were registered and divided randomly into three groups: group receiving personal training while watching a training video (video group), group receiving training under the guidance of an expert (teaching group), and group receiving personal training with a virtual simulator (virtual group). The students practiced laparoscopic suturing and tying skills for 1 hour. Following their training, they performed the evaluation task of three sutures and ties using a laparoscopic fundoplication simulator. We developed a 1-year-old infant body model (body weight 10 kg) based on computed tomography data and established a pneumoperitoneum body model based on a clinical situation.
Results:
The path length of the assistant forceps in the virtual group tended to be longer than in the other groups. The average acceleration of the assistant forceps in the virtual group was faster than in the other groups (P = .04). There were no significant differences in the other evaluation parameters.
Conclusion:
A long-term and combination training study should be performed to develop the best method for training medical students and inexperienced young surgeons.
Introduction
Less operative scarring, early recovery, and cosmetic benefits are the great merits of endoscopic surgery, and this technique has benefited pediatric patients who are in the growth stage. In addition, because only a small incision can be used in pediatric patients given their small body size, endoscopic operations with their expanded field of view provide better visualization than open operations. 1 Furthermore, the small incision used with endoscopic surgery keeps any disturbance of the growth or development to a minimum. 2
However, it is difficult to master the technique of endoscopic surgery. Training programs for developing endoscopic suturing skills range from the dry-box training to virtual reality (VR) simulator training. Pearson et al. 3 reported the first VR simulator. There are advantages and disadvantages to each training method.4,5 However, only a few studies have focused on which method is the most useful for medical students and young surgeons, especially for trainees in pediatric surgery who will be asked to perform operations in the tiny body cavity of small patients.
Our research group developed several novel models of pediatric surgery and reported their utility.6–8 The laparoscopic fundoplication model 6 is useful for helping trainees acquire skills in suturing and knot-tying in small cavities. The quality of suturing can also be evaluated in this model, so trainees can polish their technique based on an objective evaluation. However, this model is at present used only for research, and most trainees must practice with the usual dry-box trainer or a VR simulator.
The present study compared the proficiency of medical students in acquiring laparoscopic suturing skills using the novel pediatric fundoplication model after short-term training using a video, an expert teacher, or a virtual simulator. The aim of this study was to evaluate which training method was most useful for helping trainees hone their laparoscopic suturing skills in small spaces.
Materials and Methods
Laparoscopic fundoplication model with a surgical skill validation system
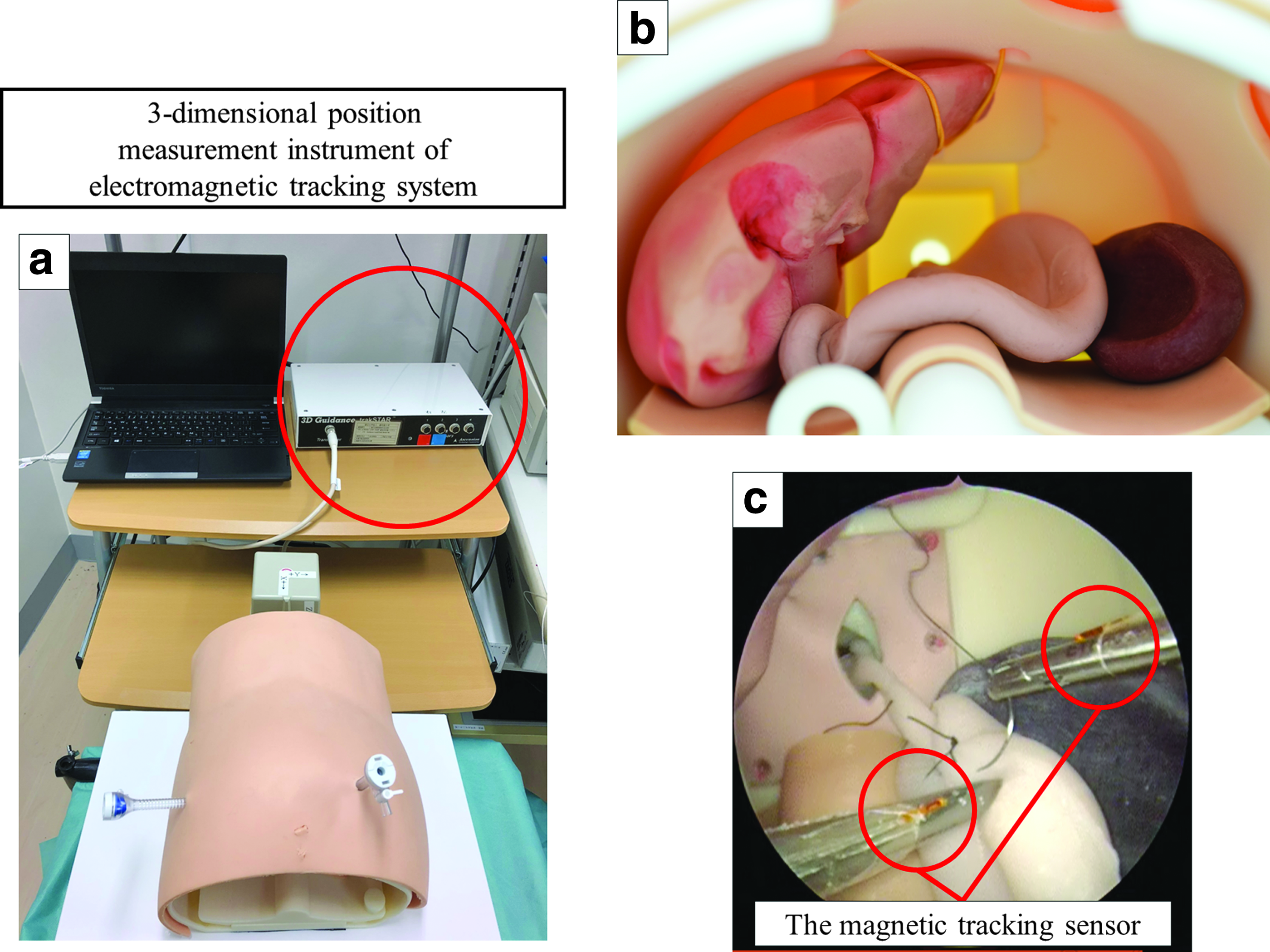
We developed a 1-year-old infant body model (body weight 10 kg) based on computed tomography data and reproduced the pneumoperitoneum body model based on a clinical situation, 6 as shown as Figure 1. A synthetic skin covers the pneumoperitoneum model. The stomach was made of styrene and the liver and spleen were made of urethane.
Study participants
Seventeen medical students (sixth-year medical school students in Japan) who had no previous experience in training to perform laparoscopic suturing were registered and divided randomly into three groups: those receiving personal training while watching a training video (video group), those receiving training under the guidance of an expert (teaching group), and those receiving personal training with a virtual simulator (virtual group).
Curriculum
A box trainer (Endowork Pro II; MC Medical, Tokyo, Japan) was used for training in the video group and teaching group. The video group received training while watching a training video made by an expert laparoscopic pediatric surgeon about suturing and making a square knot using a “C” loop. The teaching group received the same suturing and knot-tying training under the guidance of an expert in person. The expert gave comments and advised the participants as needed. The virtual group received the same suturing instruction using a VR simulator, LapVR (CAE Healthcare, Sarasota, FL). The students in each group practiced laparoscopic suturing and tying skills for 1 hour.
Skill evaluation task
Following their training, the students were required to perform three suture ligatures for the construction of the Nissen wrap using intracorporeal knot tying. 6 The operative field of the task was reproduced based on the clinical situation. Two trocars were placed on the right and left side of the umbilicus through a covered skin. The abdominal esophagus of the stomach model was constructed through the hole of the thoracic side and fixed. The spleen was fixed in the same location as in a clinical situation. The left lobe of the liver was retracted with V-shaped suturing. A 30° scope of 5 mm in diameter was fixed using an arm connected to the Storz SD system (Karl Storz, Tuttlingen, Germany). The students used the needle holders in both hands in their training and the Nissen task. The suture material was 3–0 ETHIIBOND (ETHICON Endo-Surgery, Cincinnati, OH).
The assessment points
The assessment points in this study were as follows, improving upon the methods previously reported from our study group6,9–11:
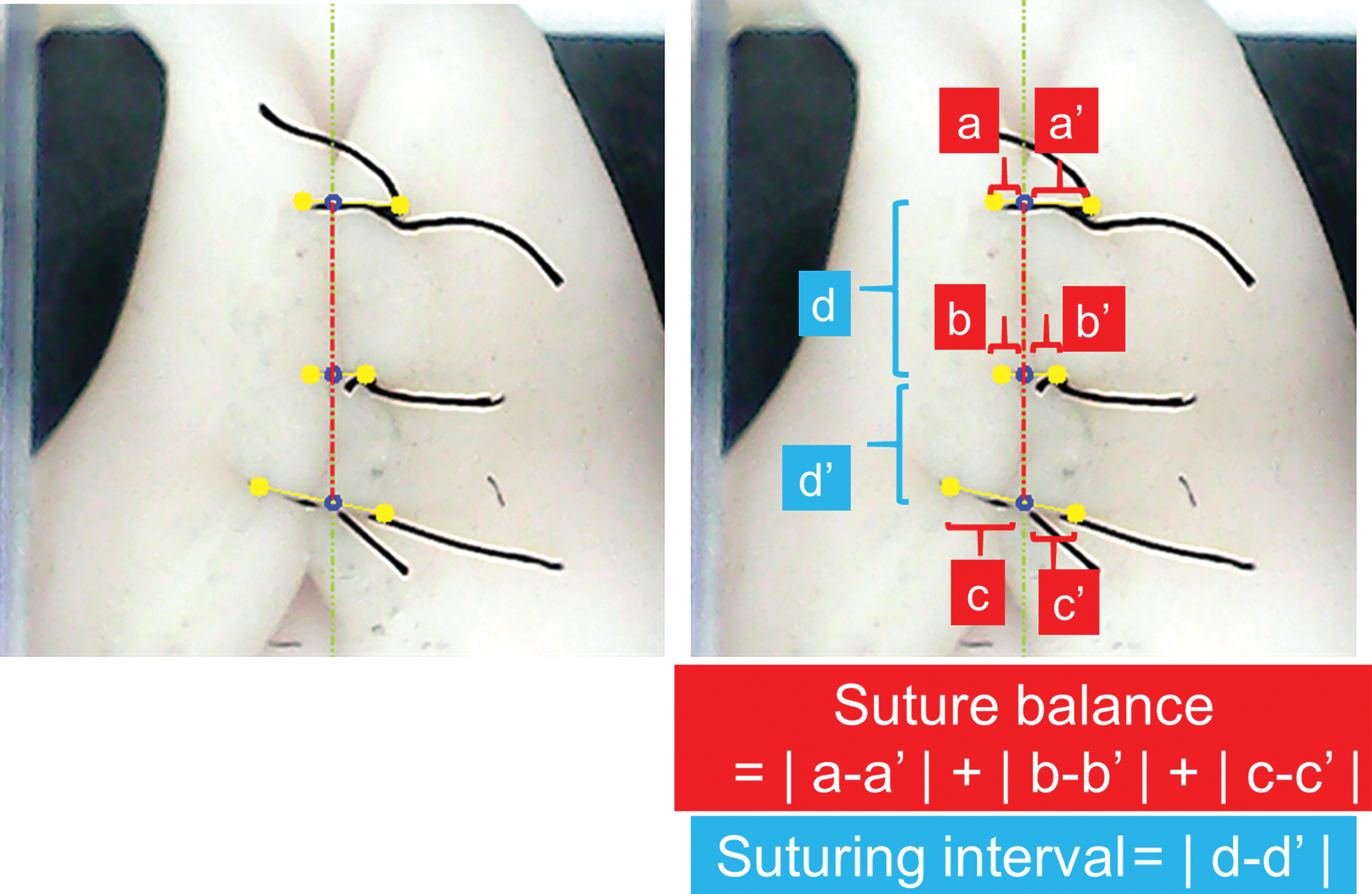
Time required to complete the task The required time was measured in seconds. It was defined as the performance time from the start to completion of task. Suturing balance of the right and left side in making three ligatures The suturing balance was measured during the task by an image analysis software program using a USB camera connected to a computer (Fig. 2). The sum of the bilateral gap in each suture ligature (|a − a′| + |b − b′| + |c − c′|; Fig. 2) was calculated and evaluated as the symmetry of the placement of the sutures. We told the students that a smaller gap was deemed superior before they start the task. Suturing intervals between the three ligatures in wrap construction
The sum of the gap of the right and left widths of suturing and the gap of the suturing interval was calculated. The suturing intervals between the first and second and between the second and third were measured by an image analysis software program using a USB camera connected to a computer (Fig. 2). The gap in the suturing interval was measured (|d − d′|; Fig. 2). These two assessment points were monitored by the image analysis system connected to a PC. We also told the students that a smaller gap in the suturing interval was deemed superior before they start the task. The total path length of the forceps The total path length of the forceps was determined using a TrackSTAR (Northern Digital, Inc., Ontario, Canada) system (Fig. 3a, c) and considered to be the spatial movement measured in millimeters (mm) in task. Average velocity of the forceps tips The result of the three-dimensional electromagnetic tracking system. The total path length The average velocity of each tip of the forceps was measured using a TrackSTAR system. Average acceleration of the forceps tips The acceleration values of each tip of the forceps were calculated from the velocity to evaluate the change in the rate of movement. The average acceleration was calculated from the absolute values of each 0.05-second acceleration. Number of tissue injuries and frame out times of the handed needle To evaluate the safety of handling the needle, the number of tissue injuries by the handed needle and times of frame out of the handed needle were counted based on an evaluation of the captured videos.
Skill evaluation system
The effectiveness of the training was evaluated by comparing the students' skill improvement after the 1-hour training using the artificial laparoscopic fundoplication simulator. The TrackSTAR was placed on the thoracic side of the model to trace the tips of the needle drivers to measure the three-dimensional position to further analyze the spatial trace of the tips of the forceps. The needle drivers in both hands had sensors mounted on the tips, and their three-dimensional locus was traced on a computer with an electromagnetic tracking system. The parameters used include the total spatial moving distance and the average of velocity in both forceps.
Statistical analyses
All data are expressed as the mean ± standard deviation. The statistical analyses were performed by a two-factor factorial analysis of variance followed by Tukey's multiple-comparison posttest. All of the results were considered statistically significant when P-values were <.05.
Results
The results of the skill evaluation were as follows:
Time required to complete the task
Table 1 shows the time required to complete the tasks: 1641.11 ± 375.25 seconds for the video group, 1702.75 ± 886.27 seconds for the teaching group, and 1480 ± 916.87 seconds for the virtual group. There were no significant differences among the three groups (P = .70).
The Result of the Time Required to Complete the Task and Image Analysis of Suturing
The suturing balance of the right and left side in making three ligatures was calculated to determine the sum of the gaps between each suture ligature in the task (Table 1). The sum of the gaps for the right- and left-side balance in the video group was 5.47 ± 2.60 mm, that in the teaching group was 5.15 ± 2.23 mm, and that in the virtual group was 3.82 ± 0.9 mm. There were no significant differences among the groups (P = .52).
Suturing interval between the three ligatures in wrap construction
The pitch of the three wrap sutures was measured. And the gaps between the suturing intervals of first to second and second to third were measured and calculated (Table 1). The gap in the video group was 2.76 ± 1.58 mm, that in the teaching group was 2.4 ± 2.55 mm, and that in the virtual group was 2.15 ± 1.84 mm. There were no significant differences among the three groups (P = .71).
The total path length of the forceps
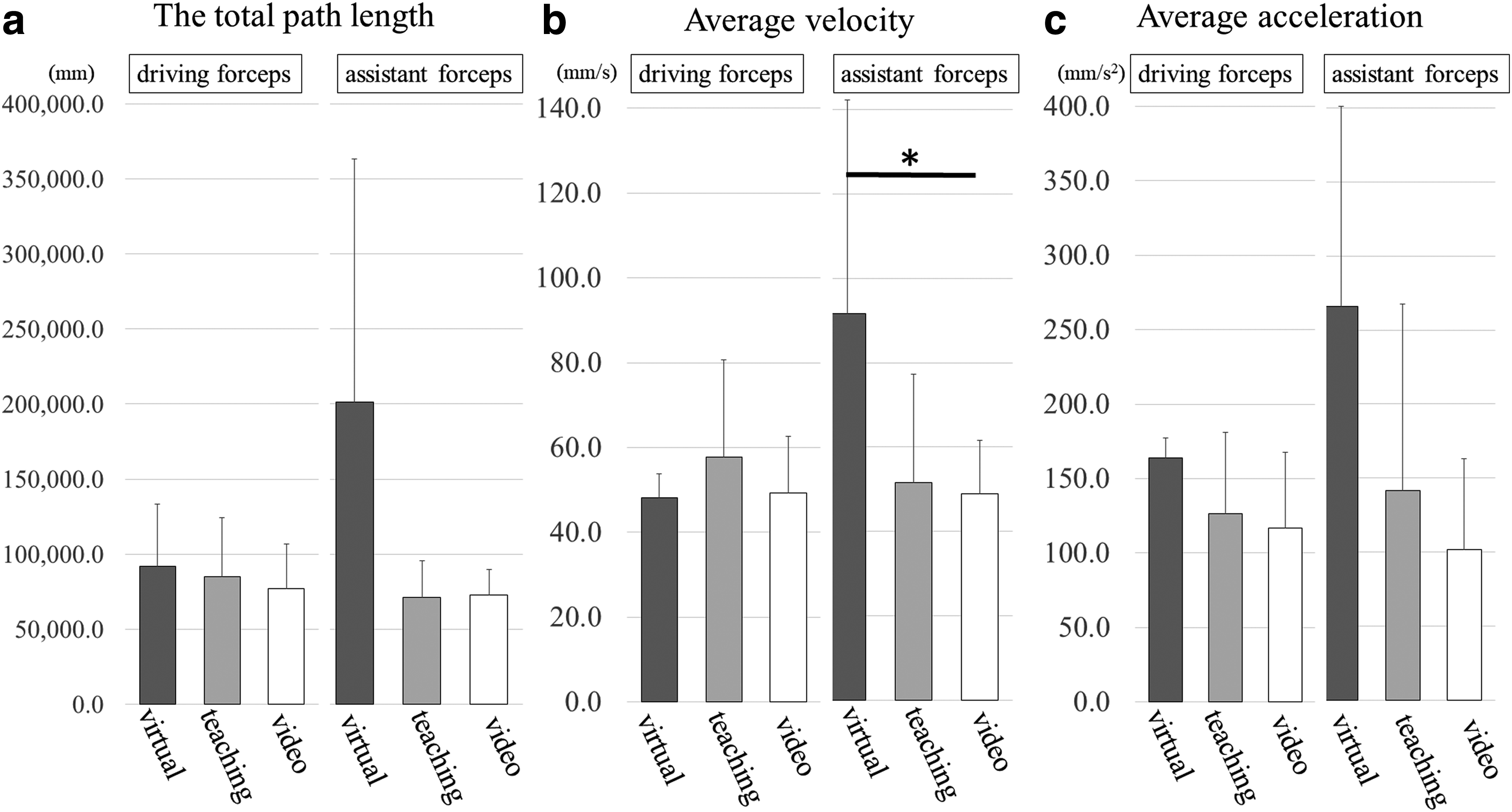
The result is shown in Figure 3a. The length of the needle-driving forceps in the video group was 77175.02 ± 29662.57 mm, that in the teaching group was 84778.47 ± 39746.98 mm, and that in the virtual group was 92089.01 ± 40975.45 mm. There were no significant differences among the three groups (P = .48).
The length of the assistant forceps in the video group was 72675.41 ± 17265.22 mm, that in the teaching group was 71270.62 ± 24544.79 mm, and that in the virtual group was 201308.59 ± 162047.59 mm. There were no significant differences among the three groups (P = .06).
Average velocities of the forceps tips
The average velocity of the each forceps tips is shown in Figure 3b. The average velocity of the needle-driving forceps in the video group was 49.32 ± 13.34 mm/s, that in the teaching group was 57.65 ± 23.02 mm/s, and that in the virtual group was 48.19 ± 5.61 mm/s. There were no significant differences among the groups (P = .45).
The average velocity of the assistant forceps in the video group was 48.93 ± 12.76 mm/s, that in the teaching group was 51.66 ± 25.59 mm/s, and that in the virtual group was 91.58 ± 50.72 mm/s. There were no significant differences among the groups (P = .08).
Average acceleration of the forceps tips
The average acceleration of the forceps tips is shown in Figure 3c. The average acceleration of the needle-driving forceps in the video group was 116.85 ± 50.51 mm/s 2 , that in the teaching group was 126.18 ± 54.95 mm/s 2 , and that in the virtual group was 164.05 ± 13.25 mm/s 2 . There were no significant differences among the groups (P = .10).
The average acceleration of the assistant forceps in the video group was 101.96 ± 61.04 mm/s 2 , that in the teaching group was 141.32 ± 126.11 mm/s 2 , and that in the virtual group was 265.81 ± 135.38 mm/s 2 . The average acceleration of the assistant forceps was significantly faster in the virtual group than in the video group (P = .04).
Number of tissue injuries and frame out times of the handed needle
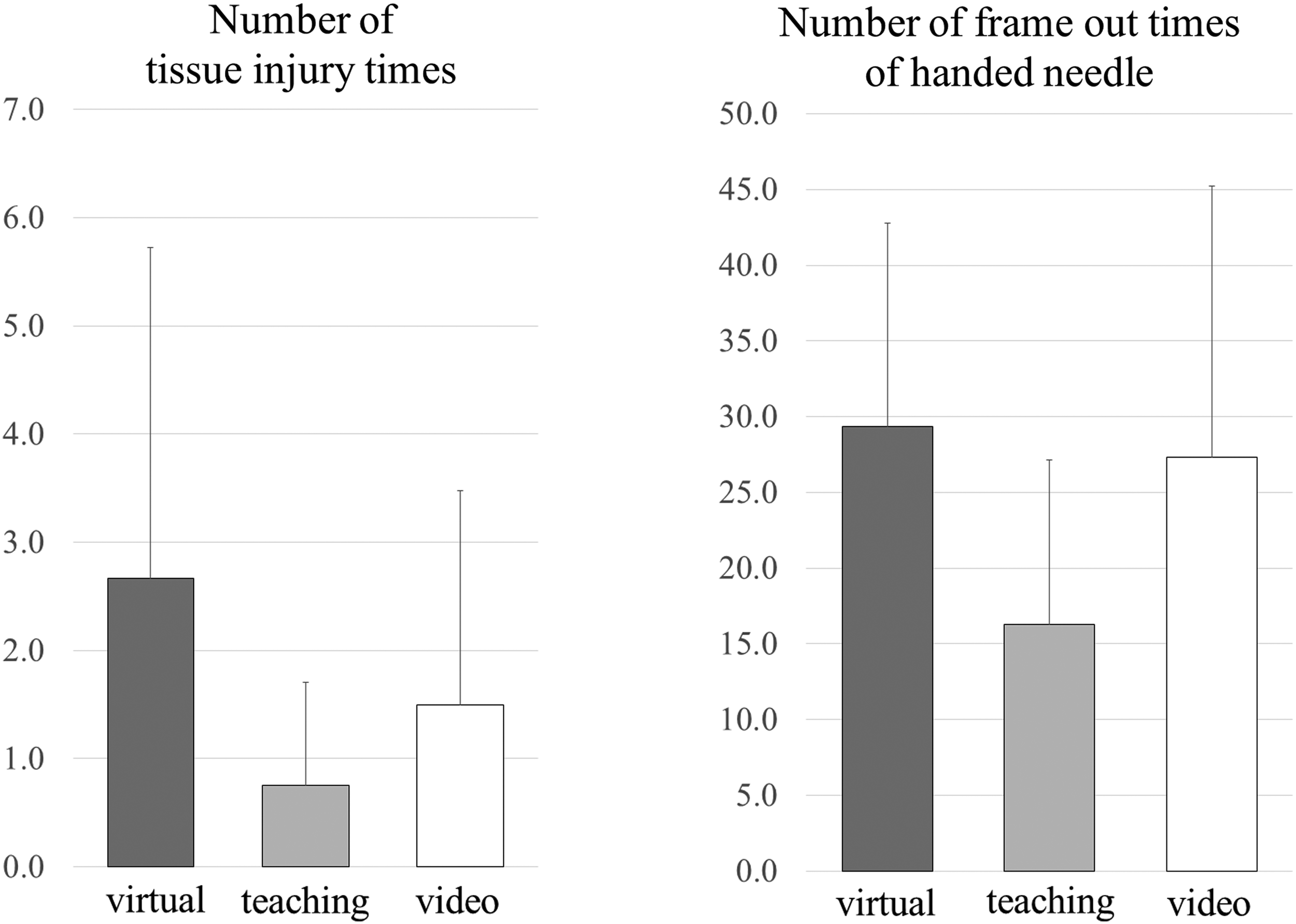
The number of times the tissue was injured by handed needle and frame out times of handed needle is shown in Figure 4. The number of times the tissue was injured by handed needle in the video group was 1.5 ± 1.97 times, in the teaching group was 0.75 ± 0.96 times, and in the virtual group was 2.67 ± 3.06 times. The number of frame out times of handed needle in the video group was 27.33 ± 17.92 times, in the teaching group was 16.25 ± 10.9 times, and in the virtual group was 29.33 ± 13.43 times. There were no significant differences among the groups in any assessment points; however, both numbers of the teaching group were less than other two groups (P = .49, .46, respectively).
Discussion
The present study aimed to evaluate the effectiveness of the box training (with an expert teaching or a teaching video only) and the VR simulator training for learning the complex task of intracorporeal suturing and knot tying in a small cavity and to clarify the features of each training method. We used the same evaluation methods for the endoscopic surgical skills, as described in our previous report,6,7,9–12 including the Nissen fundoplication simulator.
The number of tissue injury times by handed needle and frame out times of handed needle of the forceps among three groups was compared.
The major results of the present study were as follows: (1) the total path length of the assistant forceps in the virtual group tended to be longer than in the other two groups; (2) the average velocity of the assistant forceps in the virtual group tended to be faster than in the other two groups; (3) the average acceleration of the assistant forceps was faster in the virtual group than in the teaching or video group; (4) there were no significant changes in the total time, image evaluations of suturing, total path length and average velocity of the needle-driving forceps, or number of tissue injuries by handed needle and frame out times of handed needle among the three groups.
At the beginning of the present study, it was expected that the students taught by an in-person expert using a dry-box trainer would perform the best among the groups evaluated. The expert surgeon taught the basic skills and gave advice on each of the several points according to the suturing skill level of each of the students. However, there were no significant differences in evaluation outcomes between the teaching group and the video group. Possible reasons for this result are as follows: the training term may have been too short to reveal marked difference among methods, or the expert trainer in the teaching group may simply have been less effective at teaching than the video. Short-term training has proven effective in some situations, 13 but 1 hour might have been too short for the present study. The trainer in the present study was an expert pediatric surgeon with experience in many open and laparoscopic surgeries, who was accustomed to educating trainees. A long-term training study or a comparison of the learning curve is needed to reveal the efficacy of this teaching method. In addition, this result indicated that beginners do not always need a teacher to provide advice in person to acquire basic laparoscopic operation skills using the dry-box trainer. Beginners can start training with the dry-box trainer and a teaching video.
The total path length and velocity are associated with the quality of endoscopic procedures. Expert surgeons always advise young surgeons to slow down and avoid moving too quickly during operations, especially laparoscopic surgery. Jimbo et al. 6 reported that novice surgeons move both the needle-driving and assistant forceps faster and over a longer distance than expert surgeons when using the same fundoplication model. Our research group also reported that a slow manipulation and shorter path length increased the quality of endoscopic procedures. 12 In our study, the assistant forceps of students in the group using the VR training system tended to be faster and travel farther than in the group using the dry-box trainer. This result might suggest that dry-box training is more useful for developing motion control of forceps than the VR system. Our VR system has haptic feedback; however, the sensations experienced still differ from those experienced with the dry-box trainer or an actual operation. Novice surgeons should consider the absence or difference in the haptic feedback experienced when using the VR system. However, despite these drawbacks, when using the VR system, surgeons are able to learn the process of operations. Each training method seems to have its own characteristic benefits, so the combination of the dry-box training and the VR training might help efficiently develop surgical skills in novice surgeons.
Two previous studies have compared the efficiency of short-term training in laparoscopic skills between a classical dry-box trainer and a VR simulator.4,14 Both concluded that there were no significant differences between these two training methods. Longer term training might help clarify the efficacy of each training method.
Operations performed by an expert surgeon tend to have no complications, minimal bleeding, and no mistakes, displaying “beautiful and clever maneuvering.” Our group attempted to define “beautiful and clever maneuvering” scientifically, reporting the relevance of three factors: flexibility, stability, and fluidity of motion. 10 Fluidity of motion can be defined as a lack of abrupt maneuvers and is evaluated by the rate of change in the acceleration. When the forceps move more fluidly, the acceleration slows. In the present study, the average acceleration of the assistant forceps during the task in the virtual group was faster than in the video group using the dry-box trainer. This suggested that surgeons should use not only the VR system but also dry-box for training to hone their maneuvers.
To ensure safe laparoscopic surgery, surgeons must keep their handed needle in the screen and avoid injuring organs by handed needle. To evaluate of the safety of maneuver, we counted the number of times the tissue was injured by the handed needle and frame out times of handed needle during the task. In the present study, there are no significant differences in these errors among the three groups. Tanoue et al. 15 evaluated the effectiveness of endoscopic surgery training using a VR simulator versus a box trainer for medical students. They reported that the VR simulator training was more effective for reducing errors than dry-box training. The discrepancy between their findings and our own can be attributed to the contents of the VR simulator. Further studies are needed to determine the most effective method of practicing to ensure safe maneuvers.
In pediatric endoscopic surgery, the working cavity for the forceps is tiny. And the ports are located near each other, potentially allowing for conflict. However, an ordinary dry-box trainer reflects the body size of an adult patient. In the present study, we asked the students about their impressions after all tasks had been finished. Most of them felt that the fundoplication task was much more difficult than the knot-tying training using the dry-box trainer because of the small working space. Therefore, to help familiarize trainees with working in a small cavity, the ordinary dry-box trainer should be modified so as to be more suitable for pediatric endoscopic surgery, and VR simulators specific to pediatric patients should be developed.
The present study is limited by the small number of participants. Further studies are needed to evaluate the learning curve or the combination effect of each training method.
Conclusion
The method of short-term training in this study did not affect the acquisition of laparoscopic suturing skills among medical students. However, long-term training with each method may affect the acquisition of laparoscopic suturing skills. A long-term and combination training study should be performed to develop the best method for training medical students and inexperienced young surgeons.
Footnotes
Acknowledgment
We thank Mr. Brian Quinn for his help with the article.
Disclosure Statement
The authors declare no conflict of interest associated with this manuscript.
Funding Information
This study was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (JSPS, Nos. 17K10555, 17K11514, 17K10183, 17K11515, and 17K10180).