
Abstract
Abstract
Background:
This study aimed to review our 25-year experience with pediatric laparoscopic cholecystectomy (LC) to assess its long-term outcome.
Materials and Methods:
The records of 215 children (127 girls and 88 boys) who underwent LC for the past 25 years (1993–2018) were retrospectively reviewed. All patients had a symptomatic cholelithiasis. The cholelithiasis was idiopathic in 185 patients (86%) and secondary in 30 patients (14%). A four-trocar technique was always adopted and cystic duct and cystic artery were clipped using 10-mm clips in the first 35 cases (16.3%) and 5-mm clips in the following 180 patients (83.7%). In the last 15 cases, indocyanine green (ICG)-enhanced fluorescence was adopted intraoperatively for a better identification of the anatomy of gallbladder and biliary tree.
Results:
The average operative time was 69 minutes and fell down to 52 minutes after introduction of ICG fluorescence (P = .001). Fifteen anatomic anomalies (6.9%), involving bile duct in 5 cases and cystic artery in 10 cases, were recorded. Technical problems were reported intraoperatively in 6 cases (2.8%). We recorded 4 postoperative Clavien IIIb complications (1.9%): 1 bleeding from the cystic artery, 1 dislocation of the clips on the cystic duct, and 2 iatrogenic injuries to the main bile duct managed with choledojejunostomy in 1 case and suture of the choleducus over a stent in the second case. We also recorded 3 umbilical granulomas (1.4%) (Clavien II).
Conclusions:
LC is a standardized and effective procedure to perform in children. Our 25-year experience showed that major complications (Clavien IIIb) can occur even in experienced surgeons' hands. Age, weight, and preoperative cholecystitis were significantly associated with the risk of bile duct injury in our series. Considering its versatility and safety, we believe that ICG fluorescence technology may be adopted in every LC to ease the dissection and reduce the likelihood of complications.
Introduction
Cholecystectomy is one of the most common laparoscopic operations performed in adults worldwide. 1 Reports on laparoscopic cholecystectomy (LC) in pediatric literature are scanty compared with adult literature.2–5 The main indication for LC in the pediatric population is represented by symptomatic cholelithiasis without improvement after medical treatment. 6 In general, gallbladder stones may result from hemolytic disorders, such as sickle cell anemia, thalassemia, or spherocytosis. 7 Nonhemolytic predisposing conditions include bowel resection, chronic total parenteral nutrition, cystic fibrosis, oral contraceptive use, drugs, pregnancy, and obesity. 8 This last indication has presented an exponential increase in the pediatric population for the past 10 years. 9 It has been recently reported that the two most important factors underlying the increasing number of cholelithiasis requiring surgical treatment in pediatric population are familiarity and obesity. 8 Despite the rising prevalence of pediatric obesity and gallstone disease, also biliary dyskinesia is becoming a leading indication for cholecystectomy in children.10–12
Although LC has become the standard procedure for treating these patients in all pediatric surgical centers, the incidence and management of complications have been rarely reported.13–15 Complications seem to be higher in cases with anatomic anomalies of the gallbladder, in obese patients or in case of recurrent inflammatory episodes for presence of adhesions and distorted anatomy. 16 It has been reported that the experience of the operating surgeon and the degree of difficulty faced are the two main factors that determine the conversion rate and the complications.17–19 As for technical point of view, most pediatric surgeons prefer to adopt a four-trocar technique even if technological advances offer increased operative options and facilities. 20 One of the most helpful recent advances is represented by the possibility to use indocyanine green (ICG) fluorescence technology to improve intraoperative visualization and provide detailed mapping of the anatomy of biliary tree in selected cases. 21
This study aimed to review our 25-year experience with LC in the pediatric population to assess the long-term outcome of the technique and to evaluate the incidence and management of complications that may occur with LC in children.
Materials and Methods
The medical records of 215 children (127 girls and 88 boys) who underwent LC in our pediatric surgical unit for the past 25 years (March 1993–December 2018) were retrospectively reviewed. Patients' average age at time of surgery was 10.2 years (range: 5–17) and their average weight was 46.5 kg (range: 16–120). Fifty-three patients (24.6%) had a body mass index >30 (kg/m2) and were considered obese.
The main indication for surgery was a symptomatic cholelithiasis in all patients. A biliary dyskinesia was clinically suspected in 58 patients (26.9%), but, since all these patients were identified with gallstones or cholecystitis on imaging, they were candidate to medical treatment and/or LC and the diagnosis of biliary dyskinesia was not confirmed by further investigation with cholescintigraphy. The cholelithiasis was idiopathic in 185 patients (86%), whereas an associated pathology was diagnosed in 30 patients (14%) (sickle cell disease in 14 cases, hereditary spherocytosis in 9, thalassemia in 3, and cystic fibrosis in 4). No episodes of biliary pancreatitis or obstructive jaundice were reported in our series. In each case of first diagnosis of cholelithiasis, medical treatment with ursodeoxycholic acid was prescribed by pediatrician hepatologists at a dose of 10 mg/kg twice a day for at least 6 months. Those with symptoms despite the medical treatment were candidate to LC.
Preoperative work-up included laboratory tests to check liver function and a hematologic screening for hemolytic disorders. In addition, all patients underwent preoperatively abdominal ultrasonography (US) to confirm the presence of gallstones and exclude dilatation of extra- and intrahepatic bile ducts. Only 1 patient (0.5%) with main bile duct dilatation at preoperative US underwent perioperative cholangiography.
The following outcome parameters were assessed: operative time, intraoperative anatomical findings, intra- and postoperative complications, and reoperations. Postoperative complications were classified according to the Clavien–Dindo grading system. 22
Patients' demographics are given in Table 1.
Patients' Demographics and Results
ICG, indocyanine green.
Operative technique
All patients underwent LC using the traditional four-port technique: one 10 mm umbilical port for 0° laparoscope and three 5 mm ports for the instruments in the right upper quadrant.
Overweight and obese patients underwent preoperatively a bowel preparation with simethicone tablets (80 mg three times/day) for at least 5 days before surgery and enemas the day before surgery.
The surgery was performed under general anesthesia with orotracheal intubation and a nasogastric tube in the stomach. The children were placed on the operating table in reverse Trendelenburg position. Once the fundus was grasped and retracted, the cystic duct and the cystic artery were isolated, clipped, and sectioned in all cases. As for the technical point of view, 10-mm titanium clips were used in the first 35 cases (16.3%) whereas 5-mm titanium clips were adopted in the following 180 patients (83.7%). The gallbladder was always removed through the navel without using an endobag except in 5 patients in whom a perforation of the gallbladder wall occurred during the dissection phase and we preferred to put the gallbladder in an endobag before its extraction. In 25 patients affected by a hemolytic disorder associated with splenomegaly (11.6%), a concomitant laparoscopic splenectomy was performed. In these cases, the spleen was put into an endobag, finger fragmented, and then removed from the umbilicus. At the end of the procedure, a drain was always placed in the subhepatic space and left for at least 24 hours postoperatively.
ICG fluorescence-guided LC
In the last 15 cases, the ICG fluorescence technology was adopted intraoperatively to better identify the anatomy of gallbladder and biliary tree. A laparoscopic system (KARL STORZ GmbH & Co. KG, Tuttlingen, Germany) was used in all cases. The imaging was generated by the high-end full high-definition camera system (IMAGE1 S; KARL STORZ) connected to a 0° optic equipped with a specific filter for optimal detection of the near infrared (NIR) fluorescence and standard white light imaging. Switching from standard white light mode to NIR mode was done instantaneously by the surgeon through foot-pedal control.
In all cases, the ICG dye (Verdye; Pulsion Medical Systems, Munich, Germany) was injected into a peripheral vein 18 hours before the procedure using a dosage of 0.4 mg/kg (vials 25 mg/5 mL). In this way, it was made sure that most of the agent had accumulated in the extrahepatic duct, whereas absence of fluorescence was typically noticeable in the liver parenchyma. The critical view of safety (CVS) is a method of identification of the cystic duct and cystic artery during LC and has been proved to be helpful to avoid the risk of biliary or vascular injuries. 23 Three criteria are required to achieve the CVS: (1) the hepatocystic triangle is cleared of fat and fibrous tissue; (2) the lower one-third of the gallbladder is separated from the liver to expose the cystic plate; and (3) two and only two structures (cystic duct and cystic artery) should be seen entering the gallbladder. We always followed all three of these criteria, and ICG technology was very helpful to achieve the CVS more quickly and easily (Fig. 1). The gallbladder and the biliary anatomy (cystic duct, CD; common hepatic duct, CHD; common biliary duct, CBD), and especially the CD-CBD junction, were clearly identified in all cases, adopting ICG visualization alternate to white standard light vision, despite the presence of abundant fatty tissue or severe inflammation and adhesions between the gallbladder and surrounding tissues (Fig. 2). The biliary structures appeared blue or green under NIR mode, according to the software adopted (Figs. 1 and 2). The dissection of the gallbladder from the liver bed using cautery may also be done using NIR fluorescence alternatively to white standard light vision, according to the surgeon's preference. The fluorescence of the gallbladder was useful in differentiating the thin layer between the gallbladder and the liver.
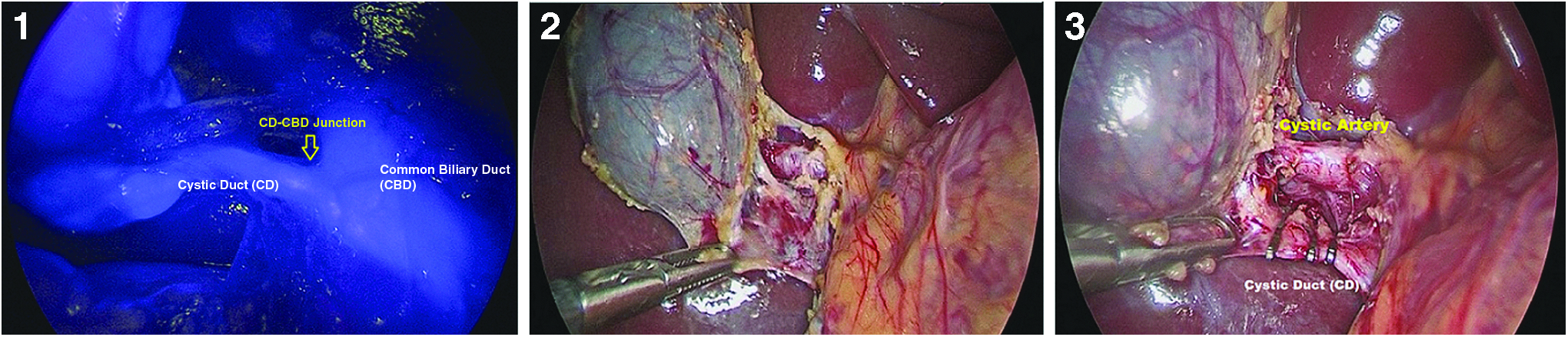
The steps of the critical view of safety:
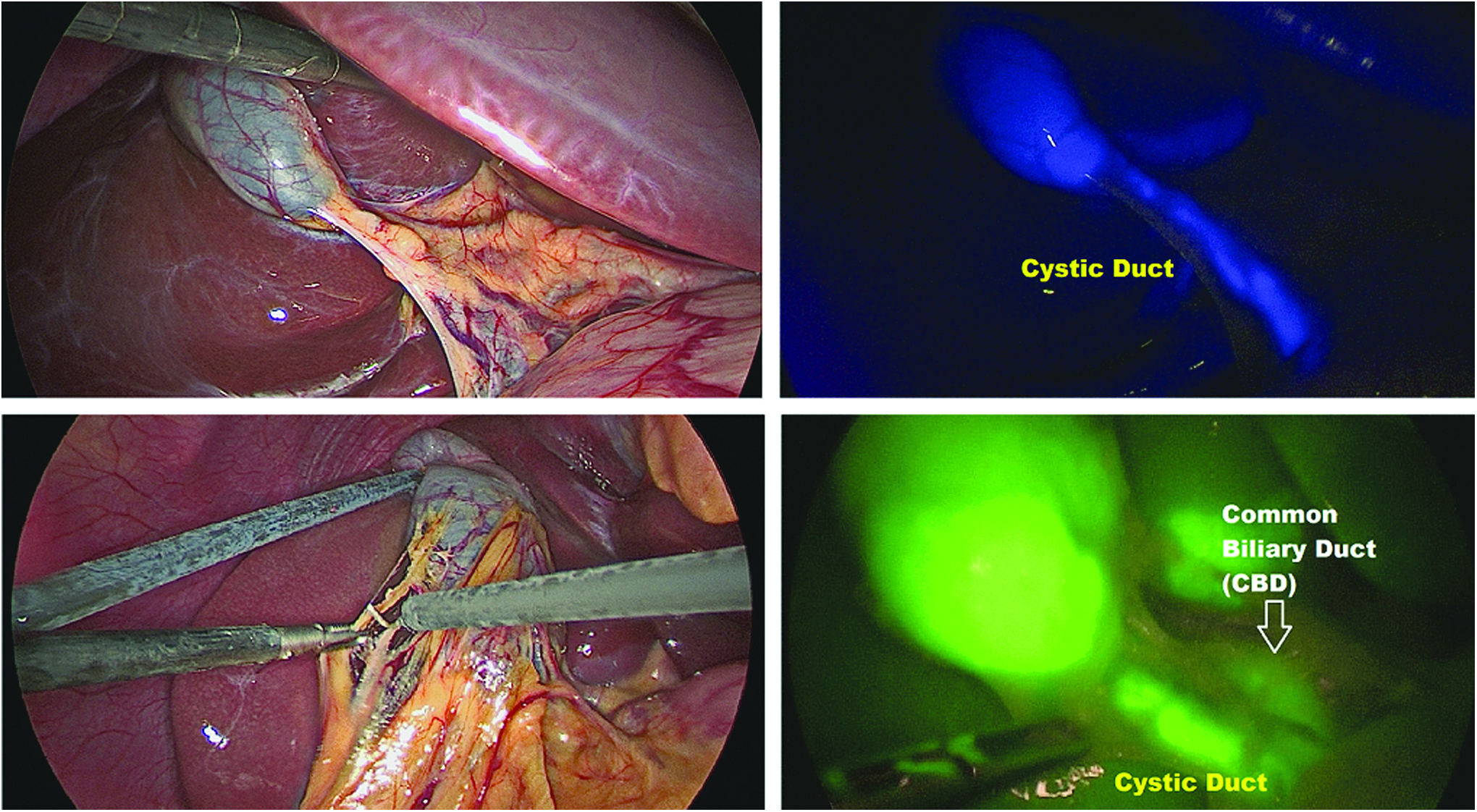
Indocyanine green fluorescence made identification of the cystic duct easier despite the presence of abundant fatty tissue or adherences.
All steps of LC using ICG-enhanced fluorescence are shown in Video 1.
Results
The operative time ranged between 42 and 100 minutes (average 69 minutes). After introduction of ICG fluorescence-guided procedure, the average operative time fell down to 52 minutes (range: 35–85). We also compared the 15 ICG operations with the last 15 cases operated without ICG technology, and we observed a significant decrease in operative time after introduction of ICG fluorescence (52 versus 66.7 minutes) (P = .001). These results demonstrated that these faster operations were directly related to the ICG use, excluding the bias of the learning curve's effect.
All patients restarted oral liquid intake few hours after surgery and full oral diet was introduced on the second postoperative day. The average analgesic requirement (paracetamol 15 mg/kg every 8 hours) was 20 hours (range: 18–30). The abdominal drain was removed on the first postoperative day in all cases and the average hospitalization was 49.5 hours (range: 26–60).
Fifteen anatomic anomalies (6.9%), involving the bile duct and the cystic artery, were discovered intraoperatively. The bile duct's anatomic anomalies, which we found in 5 patients, included a short cystic duct in 4 cases (1.8%) and aberrant hepatic ducts in 1 case (0.5%). The cystic artery's anatomical variations, which we discovered in 10 patients, included (1) the cystic artery located anterior to the common bile duct in 4 cases (1.8%), (2) short cystic arteries in 4 cases (1.8%), and (3) multiple cystic arteries in 2 cases (1%). Technical problems were reported during surgery in 6 cases (2.8%): a failed detachment of the tips of reusable scissors in 1 case and a small perforation of the gallbladder wall during the dissection phase in other 5 cases (2.3%). All these problems were easily managed by changing the instrument in the first case, whereas the hole of the gallbladder wall was closed using clips and gallbladder fluid was aspirated using a suction device and the gallbladder was extracted using an endobag in the other 5 cases. No conversions to open surgery were reported in our series.
Four postoperative Clavien IIIb complications requiring a redo surgery (1.9%) were recorded: one bleeding from the cystic artery, one dislocation of the clips on the cystic duct, and two iatrogenic injuries to the main bile duct not identified during surgery and managed with choledojejunostomy on the seventh postoperative day in 1 case and suture of the choleducus over the guide of a stent positioned using endoscopic retrograde cholangiopancreatography on the fifth postoperative day in the second case. Both patients who reported biliary complications were >14 years, obese, and had experienced several episodes of cholecystitis before surgery. We also recorded three umbilical granulomas (1.4%), treated with topical silver nitrate (Clavien II). No complications occurred in the ICG patients. All results are given in Table 1.
We also analyzed demographics and operative factors associated with bile duct injury in our series. Univariate analysis revealed that age, weight, and preoperative cholecystitis were significantly associated with the risk of bile duct injury (P = .001). No association was found between duration of surgery and presence of biliary and vascular anomalies and incidence of bile duct injury (Table 2).
Univariate Analysis of Demographics and Operative Factors Associated with Bile Duct Injury in Our Series
IQR, interquartile range.
Discussion
LC is considered worldwide the “gold standard” in the surgical management of symptomatic cholelithiasis in adult and pediatric patients.1,2 However, reports on LC in pediatric literature are scanty compared with adult literature, so it is difficult to establish the validity of this procedure in a large case series of pediatric patients.2–5 In 2001 and 2009, our group published two articles focused on the outcome of LC performed in a single pediatric surgery center.14,24 Ten years later and with >200 laparoscopic cholecystectomies performed, we decided to analyze our 25-year experience with the aim to give to the readers some take-home messages on this surgical procedure.
In accordance with the international literature reports, the cholelithiasis was more frequently idiopathic in our series (86%), and the diagnosis was often incidental during an abdomen US performed for other indications. However, before defining it idiopathic, we must always rule out all predisposing risk factors and associated pathologies. The first take-home message of our 25-year experience is that the management of children with cholelithiasis requires a multidisciplinary approach and an accurate hematologic screening is mandatory to search a possible underlying hematologic disease, as reported in 14% of our patients, who required a concomitant splenectomy in most cases. In our opinion, the strict follow-up performed by pediatricians during the conservative management and the timely indications for surgery explained the absence of preoperative complications of cholelithiasis, including pancreatitis or CBD obstruction, in our series.
The incidence of bile duct injury during LC that we reported in our series (0.9%) was in accordance with the current pediatric literature (0.3%–0.6%).25,26 Several predisposing factors to such injuries have been identified and include acute cholangitis, gangrenous cholecystitis, perforated gall bladder, scleroatrophic gall bladder, Mirrizzi's syndrome, duodenal ulcer, pancreatic neoplasm, pancreatitis, hepatic neoplasm and infections, fibrosis in triangle of Calot, obesity, local hemorrhage, variant anatomy, fat in porta hepatis, and the presence of anomalous duct or vessel. 27 Our study confirmed that age, weight, and preoperative cholecystitis were significantly associated with the risk of bile duct injury. Both patients who reported biliary complications in our series were >14 years, obese, and had experienced several episodes of cholecystitis before surgery and, therefore, presented more adhesions between the gallbladder and the surrounding structures, which made more challenging the entire procedure and in particular the dissection phase and the identification of single anatomic structures. No association was found between duration of surgery and presence of biliary and vascular anomalies and incidence of bile duct injury in our series.
Our experience confirmed that such complications can occur also in expert hands. Some authors have recently described biliary duct injuries, caused by experienced laparoscopic surgeons, perhaps because they tend to operate on more difficult patients. 28 It is obvious that severe chronic inflammatory reactions, such as “shrunken” gallbladder with shortened cystic duct, abundant fatty tissue, and biliary or vascular anomalies, make the procedure more challenging and increase the risk of bile duct injuries. 17 We believe that more likely explanations for such complications in LC are patients' disease or simply technical errors.
One of the most helpful recent advances is the use of ICG fluorescence technology that we adopted during the past 2 years to improve intraoperative visualization and provide detailed mapping of the anatomy of biliary tree in selected cases. The ICG dye may be injected intravenously with no reported adverse reactions. Fluorescence is produced by exciting the fluorophore ICG with a specific wavelength light (∼820 nm) in the NIR spectrum and it is visualized using specific cameras and optics.21,29 Since ICG is secreted entirely by the liver into the bile, the visualization of the biliary tree and in particular of the anatomy of Calot's triangle is one of the most common and useful applications.21,29 In fact, iatrogenic biliary tract injury, generally due to misinterpretation or poor visualization of biliary tree anatomy, still represents one of the most dangerous complications of cholecystectomy, with an incidence ranging between 0.4% and 1.3%.30,31 So, a careful and precise dissection of the Calot's triangle, possibly combined with an intraoperative cholangiogram, have been demonstrated to reduce the risk of intraoperative injury of biliary ducts.32,33 We always followed all criteria of the CVS 23 and the ICG technology was very helpful to achieve the CVS more quickly and easily (Fig. 1). In our series, ICG sensitivity in the identification of the gallbladder and the biliary anatomy (CD, CHD, and CBD), especially the CD-CBD junction, was 100%, irrespectively of the presence of abundant fatty tissue or severe inflammation and adhesions between the gallbladder and surrounding tissues (Fig. 2). In addition, the better anatomical vision allowed by ICG fluorescence also allowed a faster surgery compared with the traditional approach, as reported in our series. In addition, no complications occurred in the ICG patients in our series.
Also, the interval time between ICG injection and its secretion into the bile has been matter of debate,32,33 since the lag time between injection and peak fluorescence can make the ideal timing of ICG injection problematic. To obviate these problems, some authors reported that direct gallbladder ICG injection provided immediate visualization of extrahepatic biliary structures. 34 We preferred to inject the ICG dye into a peripheral vein and we standardized timing and dosage: we always performed the injection 18 hours before the procedure at a dosage of 0.4 mg/kg, and we obtained a successful visualization of the biliary tree in 100% of cases. This timing of injection also allowed us to overcome the commonly reported problem of the background fluorescence of the liver that can interfere with optimal viewing of the extrahepatic biliary structures. 34
According to our experience, the best candidates to ICG fluorescence are obese patients, patients with history of inflammation and/or with suspicion of biliary or vascular anomaly of the gallbladder on preoperative US. However, considering that this technique is easy to use, safe, and versatile, if the operating room is equipped with NIR fluorescence technology, it may be adopted in every LC with practically no adjunctive costs except for the ICG vial (cost about 40 EUR).
As for management of complications, our experience showed that most complications can be easily managed in laparoscopy, provided the surgeon is skilled in this technique. Another take-home message is that the laparoscopic team should be experienced with biliary surgery because in cases of bile duct complications—which are rare but possible—a biliodigestive anastomosis may be required. Regarding the complications linked to the use of clips, two Clavien IIIb complications occurred in our series were due to dislocation of the clips positioned on the cystic duct and cystic artery. We believe that these complications were probably due to a bad positioning of the clips. An alternative to titanium clips may be represented by hem-o-lok clips, which are probably more stable than metallic ones, or sealing devices, but we have no experience in using these devices for cholecystectomy. 35
Regarding the need for perioperative cholangiography, we performed it in only 1 patient, who presented dilatation of the main bile duct on preoperative US. The literature reports that patients scheduled for elective LC who have an unremarkable clinical examination, normal liver biochemistry and serum amylase levels, and no dilatation of the biliary tree on US do not need pre- or intraoperative cholangiography.36,37 However, as shown by our experience, ICG fluorescence imaging allowed to perform an intraoperative “virtual cholangiography” and to identify extrahepatic biliary anatomy without or with minimal dissection of Calot's triangle (Fig. 1).
In conclusion, LC is a standardized and effective procedure to perform in children. Our 25-year experience showed that major complications (Clavien IIIb) can occur even in experienced surgeons' hands. Age, weight, and preoperative cholecystitis were significantly associated with the risk of bile duct injury in our series. Considering its versatility and safety, we believe that ICG fluorescence technology may be adopted in every LC to ease the dissection and reduce the likelihood of complications. The ICG dye was cheap (about 40 EUR per vial), easily available, and the procedure was no time consuming since it required only a preoperative ICG injection, and fluorescent images of the interested organs were obtained in real time at any point during surgery. Furthermore, the procedure was very safe. In our series, no allergy or other adverse systemic reactions to ICG were reported, either early or late after surgery. The only contraindication for clinical use of ICG is in patients who have a history of allergy to iodides since it contains sodium iodide. The other main limitation is the need of a special equipment in the operating room to use the ICG technology.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.