
Abstract
Abstract
Background:
Morbidity of traditional open surgery for the treatment of gynecomastia includes asymmetry, retraction of the nipple, and poor scarring. Other approaches were described to improve the results. Endoscopic subcutaneous mastectomy (ESCM) was reported in adult series, including a few adolescents. This technique was considered as safe with good aesthetic results. The aim of this study was to evaluate the results of ESCM in an adolescent series.
Patient and Methods:
We treated 19 adolescents with Simon's grade IIB and III gynecomastia between June 2014 and July 2018. They could choose open surgery through the nipple or endoscopic surgery by axillary approach. To perform ESCM, three trocars were placed on the midaxillary line to dissect the gland. The resection was performed leaving 1 cm thickness of gland behind the nipple. The gland was extracted after morcellation through the 10 mm trocar. A drainage tube was placed in the cavity. The patients wore a thoracic belt smoothly compressing the operative areas for 15 days. The result was considered as good when there was no remaining gland, good symmetry, and no nipple retraction or nipple lateral displacement.
Results:
During the study period, 12 adolescents were treated by ESCM and 7 preferred open surgery. Among the 12 ESCM patients, 7 had bilateral and 5 unilateral gynecomastia. A subcutaneous injection of serum was done in the last 6 patients to facilitate the creation of the work space. A 2- or 3-mm second-degree burn occurred in 4 cases, 2 on the nipple and 2 just above the nipple, with a 2 mm remaining scar above the nipple in 1 case. The postoperative course was uneventful in 11 adolescents. One subcutaneous seroma expanded at 15 days postoperative and resolved after 3 weeks of prolonged compression by thoracic belt. The adolescents had 11 good results and 1 persistent asymmetry; 2 other asymmetries had a spontaneous improvement after 1 or 2 years.
Conclusion:
ESCM is feasible and safe for the treatment of gynecomastia in adolescents. This technique is challenging but permits to reach good aesthetic results and avoids scars on the anterior wall of the thorax.
Introduction
Benign abnormal enlargement of one or two breasts is common and physiological in adolescents. It affects less than 40% of males and usually involves in 1 or 2 years. A small number of adolescents’ complaints of discomfort and embarrassment when gynecomastia persists beyond 2 years. Surgery is the standard treatment when the size of the breast is important, corresponding to Simon's grade IIB and III gynecomastia. 1
Traditional open surgery by inferior partial circumareolar incision may cause significant morbidity, including asymmetry or poor scarring.2,3 Minimally invasive approaches were described such as liposuction-assisted excision, 4 ultrasound-assisted liposuction, 5 or vacuum-assisted biopsy device and liposuction by anterior axillary line incisions, and incision below the inframammary fold. 6 Endoscopic subcutaneous mastectomy (ESCM) was reported in adult series, including a few adolescents. This technique was considered as safe with good aesthetic results.7,8 We report a case series of adolescents undergoing ESCM to treat gynecomastia.
Patients and Method
Between June 2014 and July 2018, we treated 19 adolescents with Simon's grade IIB and III gynecomastia. The ESCM was presented and explained to the adolescents and their parents as a new technique in pediatric surgery, but reported in two publications in adults. The patients and their family were given the choice between ESCM and open surgery, and gave written consent before surgery. The principles outlined in the Declaration of Helsinki have been followed. In case of ESCM, a 10-mm incision was done on the midaxillary line at the level of the nipple and a work space was created with scissors close to the lateral and posterior edge of the breast. A 10 mm trocar was inserted and CO2 was insufflated with 8 mmHg pressure. For the last cases, 100–200 mL of saline serum was injected into the subcutaneous and retromammary spaces to facilitate the dissection.
The instruments were used through two 5 mm trocars on the same line on each side of the first trocar. The gland dissection was done by monopolar hook or ultrasonic scalpel. When the breast was free, it was cut leaving 5–10 mm of gland thickness below the nipple to avoid its retraction. The excised tissue was then cut into strip-like pieces before extraction through the 10 mm trocar hole. A drainage tube was placed in the cavity and was removed at day 2 before the patient discharge. The patients wore a thoracic belt smoothly compressing the operative areas for 15 days postoperative.
The adolescents were reviewed at 6 weeks and 1 year or more after the procedure, with clinical evaluation, pictures, and evaluation of adolescents' and parents' satisfaction. The result was considered as good when there was no remaining gland, good symmetry, and no nipple retraction or nipple lateral displacement, and considered as bad in case of remaining gland, asymmetry, and nipple displacement or nipple retraction.
Results
Twelve adolescents were treated by ESCM and 7 preferred open surgery during the period of study. Among the 12 ESCM patients, 7 had a bilateral and 5 an unilateral gynecomastia with a mean age of 15.6 years (13–17), a mean weight of 65.3 kg (54–85), and a mean body mass index of 20.9 (17–25). There were 8 Simon's grades IIB and 4 grades III. A 10 mm trocar was used in 9 cases and a 5 mm one in 3 cases. The subcutaneous injection of serum was performed in the 6 last patients. In the last patient, adrenaline was added in the serum and the procedure began by liposuction around the gland before removing it by endosurgery.
The mean operative time was 93.3 minutes for each side (30–220). One conversion was done in a bilateral case because of too long procedure and bad endoscopic vision with a 5 mm-telescope. In 5 cases, the remaining gland below the nipple was too large and a further resection was required at the end of the procedure. A 2- or 3-mm second-degree burn occurred in 4 cases, 2 on the nipple, and 2 just above the nipple.
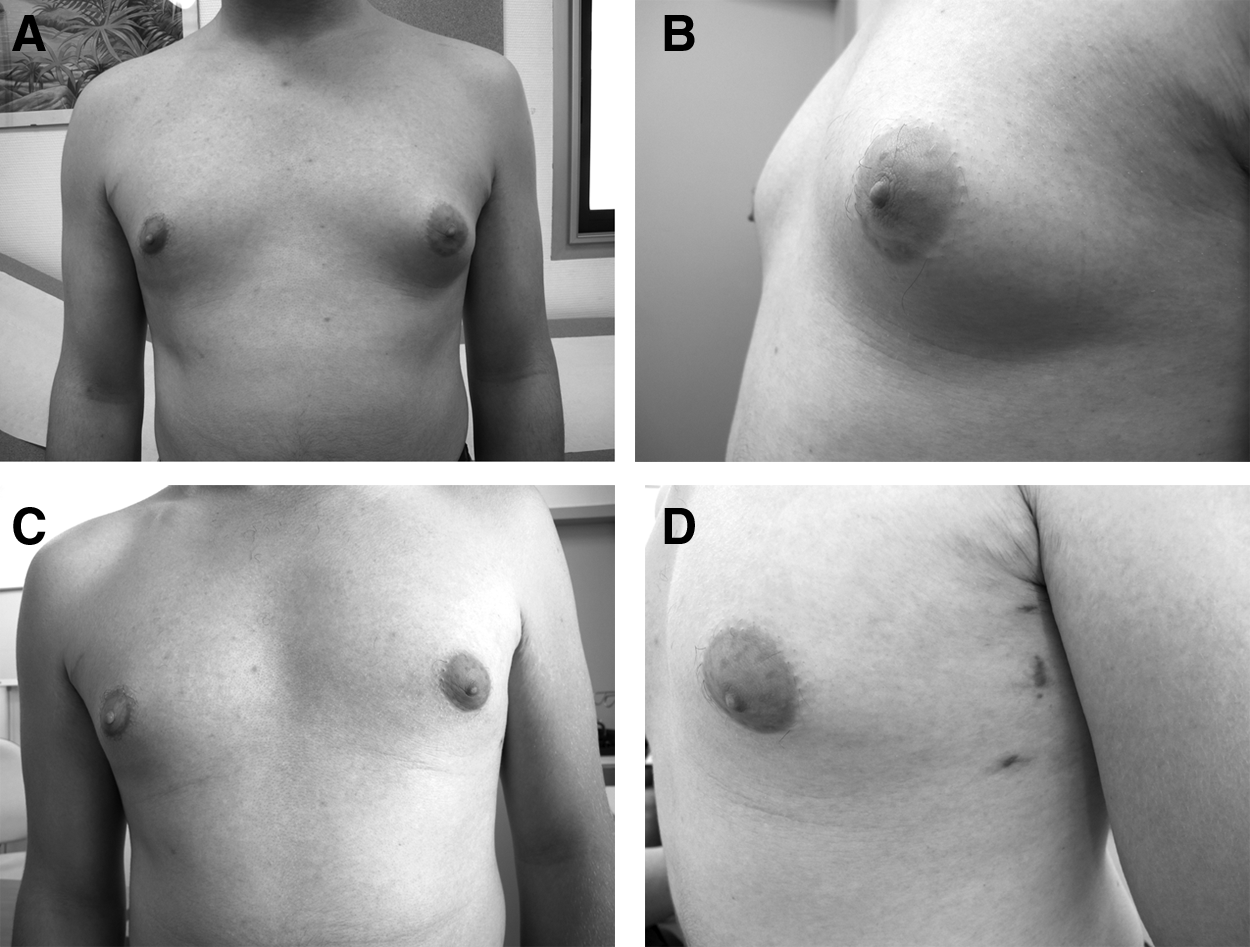
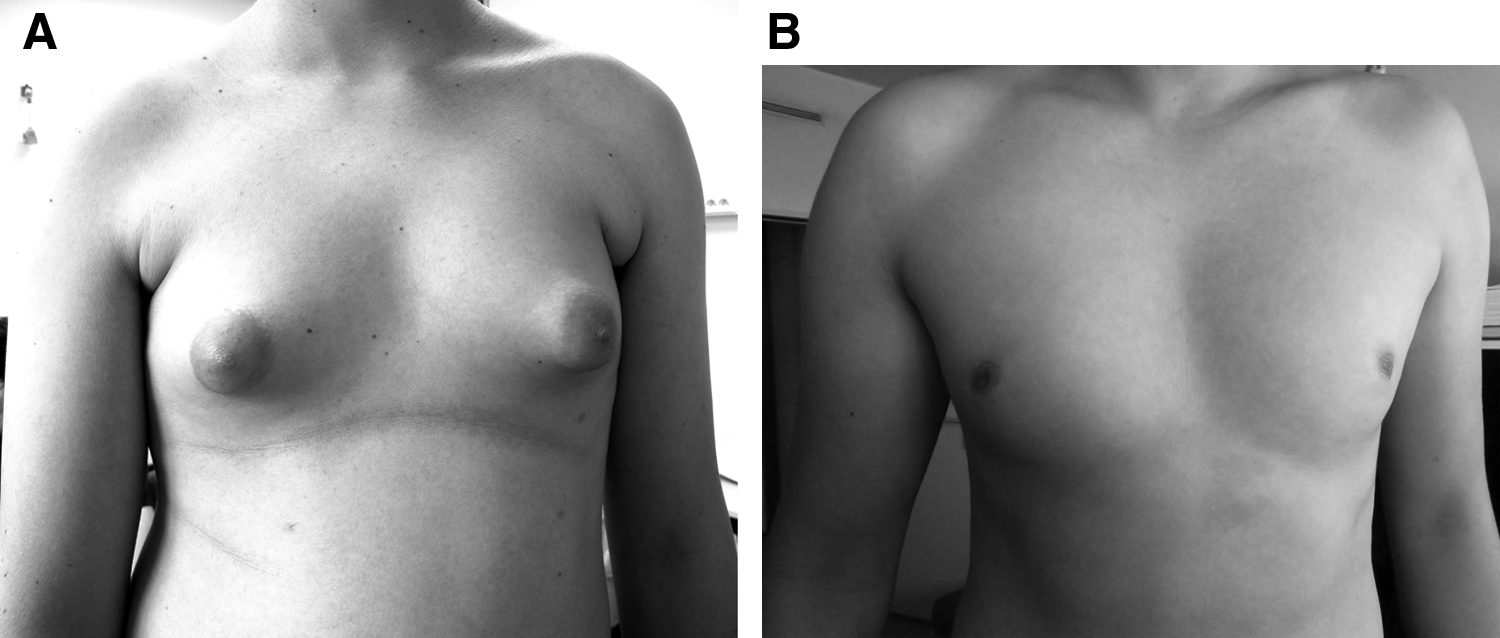
The postoperative course was uneventful in 11 adolescents. One subcutaneous seroma expanded 15 days postoperative and resolved after 3 weeks of prolonged compression by thoracic belt. We report no postoperative bleeding, hematoma, partial or total nipple necrosis, and no infection. Among the four small burns, just one left a 2 mm remaining scar above the nipple (Fig. 1). One nipple was too lateral and needed massages to free subcutaneous adhesions. Asymmetry remained in 3 adolescents with bilateral gynecomastia. They were considered as a bad result by the surgeon, but the result improved spontaneously in 2 cases after 1 or 2 years. In the 9 other patients, the ESCM was efficient with good symmetry and no lesion of the nipple (Figs. 2 and 3). Finally, aesthetic results were good in 11 cases out of 12.

Three-millimeter scar burn (arrow).
Left gynecomastia:
Bilateral gynecomastia:
Discussion
Gynecomastia is defined as benign development of male breast glandular tissue and may be asymmetric. This is a common condition in adolescents, 50%–60%, but it spontaneously regresses in 95% of the cases. 9 A minority of adolescents requires treatment. The main etiology of gynecomastia seems to be the imbalance between estrogen action relative to androgen action at the breast tissue level and this condition is named idiopathic gynecomastia. 10 Gynecomastia can also be caused by endocrine tumors (testis, adrenal gland, and pituitary gland), endocrine dysfunctions (hypogonadism, hyperthyroidism, and obesity) or uncommonly drugs intake in adolescents. An androgen resistance syndrome can also be associated, as in 1 case of the present study. A systematic endocrine evaluation is required before surgical treatment.
We used the Simon's classification in this study, 1 but various other classification systems were described from 10 clinical features: size, ptosis, tuberosity or skin elasticity of the breast, tissue predominance (gland or fat), skin redundancy, nipple malposition, chest shape, absence of sternal notch, and upper abdominal laxity. 11 None of these classifications appears to be ideal.
Surgery is indicated for gynecomastia of less than 6 cm persisting after 1 or 2 years, especially when the adolescent has psychological distress, unsatisfactory body image, and avoids activities in which the chest is exposed (swimming and sport). Several pharmacological agents have been used to change the hormonal imbalances in adult and adolescent patients, as tamoxifen, dihydrotestosterone, danazol, clomiphene, or aromatase inhibitors, but this is supported by a very low level of evidence. 12
The subcutaneous mastectomy through a semicircular incision on the edge of the areola is the gold-standard procedure and may be associated with liposuction. The results are usually good with this open technique, but postoperative complications are not uncommon, including areolar deformity, “saucer defect” from over-resection of breast tissue, poor scarring, wound infection, and nipple necrosis. In 1987, Courtiss 2 reported 101 patients with high complication rate, including under-resection (21.9%), “saucer defect” (18.7%), poor scarring (18.7%), hematoma (16.1%), and seroma (9.4%). More recently the reports rate of postoperative complications was lower. In a series of 37 patients, Fischer et al. reported 2 hematomas, 2 nipple retractions, 2 recurrences of gynecomastia, and 1 hypertrophic scar. 13 This morbidity led to the development of other procedures to improve these surgical results.
Minimally invasive surgery by axillary dissection was developed for the treatment of breast cancer by Tsangaris et al. in 1999, 14 after two studies showing this dissection was feasible in human cadavers.15,16 Tsangaris et al. showed the endoscopic axillary exploration and sentinel lymphadenectomy were achievable. This procedure is increasingly performed and the rate of complications is decreasing.
Minimally invasive surgery can be used to manage gynecomastia and Fan et al. reported the first series of 65 gynecomastia patients treated by ESCM in 2009. 7 The study included young adults with a few adolescents. Simon's type IIB and III gynecomastias could be removed by this axillary approach avoiding open surgery. This approach could even be used to treat grade III gynecomastias, as an alternative to inferior pedicle reduction mammoplasty. 17
Three steps were described by Fan et al.: (1) injection of lipolysis solution in the subcutaneous tissue, close to the gland, (2) liposuction from the axillary approach after 20 minutes to create the working space around the gland, (3) endoscopic surgery through three axillary trocars on the midaxillary line. The lipolysis solution contained 200 mL of sterile purified water, 200 mL of physiological saline, 20 mL of 2% lidocaine, and 1 mL of 0.1% adrenaline making a 521 mL mixed solution. The amount of injected solution was different according to the patient size and gynecomastia size. 7 Dexamethasone and hyaluronidase can be added. 18
Fat dissolution occurs 20 minutes after injection in the subcutaneous tissue. Liposuction is then performed around the gland and in the retromammary space, not too close to the skin and nipple-areolar complex to avoid ischemia. These two steps are very important to create the working space.
Direct dissection all around the gland from the axillary approach is much more difficult and longer, as we experienced in our 6 first cases. When the working space is achieved by liposuction, the endoscopic mastectomy can be done easily and faster with an 8 mmHg CO2 inflation and a 30° 10 mm telescope. Cooper's ligament between the gland and skin and retromammary space is resected. In 3 cases, we used a 30° 5 mm telescope and the procedure was longer, between 120 and 220 minutes for each side instead of 60–90 minutes with a 10 mm telescope that provides better vision. For the gland section behind the nipple-areolar complex, the thickness of remaining tissue was ∼1 cm, but it is not always so easy to estimate it correctly by endosurgery. The extraction of the breast tissue is achieved through the 10 mm hole after cutting it into strip-like pieces.
Fan et al. reported 2%–4% rate of complications (3 out of 125 breasts) with 1 subcutaneous seroma and 2 partial nipple necrosis occurred in the first and fifth cases, due to excessive removal of subcutaneous fat and vascular damage of the nipple-areolar complex. 7 In 2013, Cao et al. achieved this procedure in 58 patients without seromas, but reported three nipple necrosis, also at the beginning of their experience, suggesting an important learning curve. 8 Nipple necrosis did not occur in the present series. However, we deplored four small skin burns by electrocautery hook and harmonic scalpel. Fortunately no scar or depigmentation remained in 3 patients and only a 2 mm scar was visible above the areola in 1 case. Two other patients had a lateral nipple displacement. Daily massages were advised, aiming for the disappearance of subcutaneous adhesions with good aesthetic result. To avoid this complication, especially in grade III gynecomastia, the nipple position should be examined 3 days after surgery and should be adjusted by external maneuvers in case of lateral displacement to get good symmetry. 7
Asymmetry remained after surgery in 3 adolescents with bilateral gynecomastia, but the result improved spontaneously in 2 cases after 1 or 2 years. For the third adolescent, he did not want to redo the procedure because the asymmetry was less visible. Fan and Cao reported 100% of good results and adolescents' satisfaction,7,8 conversely to Fischer who reported 4 unsatisfied patients after open surgery because of 1 hypertrophic scar and 3 disaffected due to contour deformity of whom 2 persisting fatty tissue. 13
Today endoscopic axillary surgery can also be led by robotic-assisted technique and robotic nipple-sparing mastectomies for treatment of breast cancer were reported recently. 19 Other kinds of minimally invasive surgery from axillary line were described using a mammotome probe, 6 by a single incision, 18 or through a single port. 20
Conclusion
ESCM is feasible and safe for the treatment of gynecomastia in adolescents. This technique is challenging but permits to reach good aesthetic results and avoids scars on the anterior wall of the thorax.
Footnotes
Disclosure Statement
No competing financial interests exist.