
Abstract
Abstract
Background:
Laparoscopic bariatric surgery has been performed safely since 1991. In a persistent search for fewer and smaller scars, single port, needlescopic surgery, and other approaches have been implemented. Our goal was to analyze the safety and feasibility of using incisionless autostatic liver retraction for sleeve gastrectomy.
Materials and Methods:
Candidates for sleeve gastrectomy were selected, excluding those <18 and having had prior upper left quadrant surgery. Patients were randomized 1:1 to either a standard five-port technique with a fan-type liver retractor (Group A); or a four-port technique with the liver retracted using a polypropylene 1 suture passed through the right crura and retrieved at the epigastrium employing a fascial closure needle (Group B). All surgeries were performed by the same surgeon. The primary endpoint was surgery duration. Secondary outcomes were quality of surgical-field visualization, complications inherent to liver retraction, and postoperative morbidity.
Results:
One hundred patients were recruited (n = 50/group). The groups (both 90% females) were demographically and anthropomorphically comparable. Surgery duration was 30.4 ± 4.6 and 29.6 ± 4.7 minutes for Groups A and B, respectively (P = .41). Visualization was considered very good in 80% versus 82%, good in 16% versus 12%, and poor in 4% versus 6% (P = NS). Two patients from each group (4%) had self-limited minor bleeding from the liver attributed to the retraction technique. No 30-day morbidity was observed.
Conclusions:
Liver retraction using a polypropylene suture was both effective and inexpensive. Visualization and the duration of surgery were comparable to a standard liver retractor. This low-cost alternative may diminish the need for expensive instruments and reduce the number of scars without jeopardizing the safety and quality of sleeve gastrectomy.
Background
Since Wittgrove first described it, in 1994, 1 laparoscopic bariatric surgery has proven to be superior to open surgery. Less pain, lower respiratory and abdominal wall morbidity, 2 and a faster return to work are just some of the former approach's benefits.
In the unceasing search for fewer and smaller scars, variations in the traditional laparoscopic approach have been attempted, including single port surgery,3,4 needlescopic surgery, 5 and even natural orifice transluminal endoscopic surgery. 6
Laparoscopic bariatric procedures usually require a port and an instrument, both dedicated to liver retraction, so the surgeon can adequately visualize the gastroesophageal junction. Many times, this retraction instrument requires either a task-dedicated assistant or an external fixation device, resulting in additional costs. The goal of this study was to compare scarless liver retraction using a suture against a conventional 5 mm instrument for laparoscopic sleeve gastrectomy.
Materials and Methods
A pilot trial to assess feasibility and safety, involving 40 patients, was completed and its results presented at a local surgeons meeting, before enrolling any patients in the current trial. Inclusion criteria were (1) being a candidate for sleeve gastrectomy; (2) being older than 18 years of age; and (3) fulfilling the National Institutes for Health (NIH) 1991 requirements for bariatric surgery. Exclusion criteria were any previous left upper quadrant surgery or refusal to participate. All participating patients provided signed informed consent.
Candidates were evaluated and treated by a multidisciplinary team that included nutritionists, psychologists, and clinicians. Three to 6 months of dietary and lifestyle change counseling was instituted, and all patients were instructed to consume a very-low-calorie, high-protein, liquid diet and micronutrient supplementation for 2 weeks before surgery. The goal was to achieve a minimum of 10% reduction in their preoperative total body weight, relative to their weight at the time of their enrollment into the study.
Patients were randomized in a 1:1 ratio using a variable block method after first trocar insertion. For Group A, a fan-type retractor was placed through a 5 mm subxyphoid port. For Group B, a polypropylene 1 suture was passed through the right crus, 2 cm from the esophagus, and retrieved with a fascia closure needle at two different points along the epigastrium to achieve triangular retraction (Fig. 1).

All surgeries were performed by the same surgeon. Anthropometric and demographic data were recorded before surgery. Surgery duration was measured in minutes, starting from insertion of the first port (postpneumoperitoneum) to withdrawal of the last port.
A scale was used for the surgeon to rate the quality of surgical field visualization. Visualization was considered very good when no additional maneuvers were required to retract the liver, good when infrequent maneuvers were needed, and poor if such maneuvers were needed frequently.
A standard laparoscopic technique was used. After transecting small vessels of the greater curvature using a harmonic scalpel, a gastrectomy was performed, ∼4–6 cm from the pylori. To determine the starting point, a line going from the left side of the esophagus through the incisura angularis to the greater curvature was envisioned. 7 A laparoscopic, linear cutting stapler was used (Echelon Endopath™ EC45 or EC60), calibrating tightly over a 27 Fr bougie. Blue loads (3.5 mm) were preferred, although sometimes gold (3.8 mm) or green (4.1 mm) loads were used on the antrum, according to estimated tissue thickness. The staple line was always reinforced with a running 2-0 polypropylene suture. A Jackson-Pratt drain was placed along the staple line, to the left of the subphrenic recess. The drain was removed between the 8th and 14th postoperative day, if no bleeding or leaks were suspected.
The duration of surgery, in minutes, was set as the primary endpoint. The duration of sleeve gastrectomy procedures remained relatively constant in our previously published series, 8 with small standard deviation (SD). Since the duration of surgery is heavily influenced by surgical field exposure, we felt it was the best parameter to use to evaluate a surgeon's view of the surgical field and the ease of surgery.
Sample size was calculated to detect a 3-minute difference in surgery length (10% of the average time for the practicing surgeon), with an alpha error of 0.05 and power of 0.90. A SD of 4.4 was estimated, based on prior experience. 8
Results were stated as mean, along with ranges and SDs, or as percentages of the whole. Normality was evaluated using a histogram, and the data's degree of skewness and kurtosis. Student's t-test was performed for the inferential analysis of continuous variables, while Pearson's chi-squared analysis was employed for categorical variables. The statistical software package PASW® v 18 (SPSS Inc., Chicago, IL) was used for all analyses, and any two-tailed P-value under .050 was considered statistically significant.
Results
One hundred patients were recruited and randomized. Table 1 summarizes baseline intergroup comparisons. Groups A and B were comparable in their mean age (42.9 versus 42.7), body mass index (BMI; 45.1 kg/m2 versus 44.5 kg/m2), and the percentage of total body weight loss between enrollment and surgery (11.9% versus 11.4%), respectively. Both groups were composed of 90% women.
Population
Data shown as mean ± SD or percentage of the whole. Group A: fan type 5 mm retractor. Group B: retraction with suture.
BMI, body mass index; %PTBWL, percentage of preoperative total body weight loss; SD, standard deviation.
Surgery duration was 30.4 ± 4.6 minutes in Group A versus 29.6 ± 4.7 minutes in Group B (P = NS) (Fig. 2). Visualization was considered very good in 80% and 82%, good in 16% and 12%, and poor in 4% and 6%, respectively (P = NS) (Fig. 3).
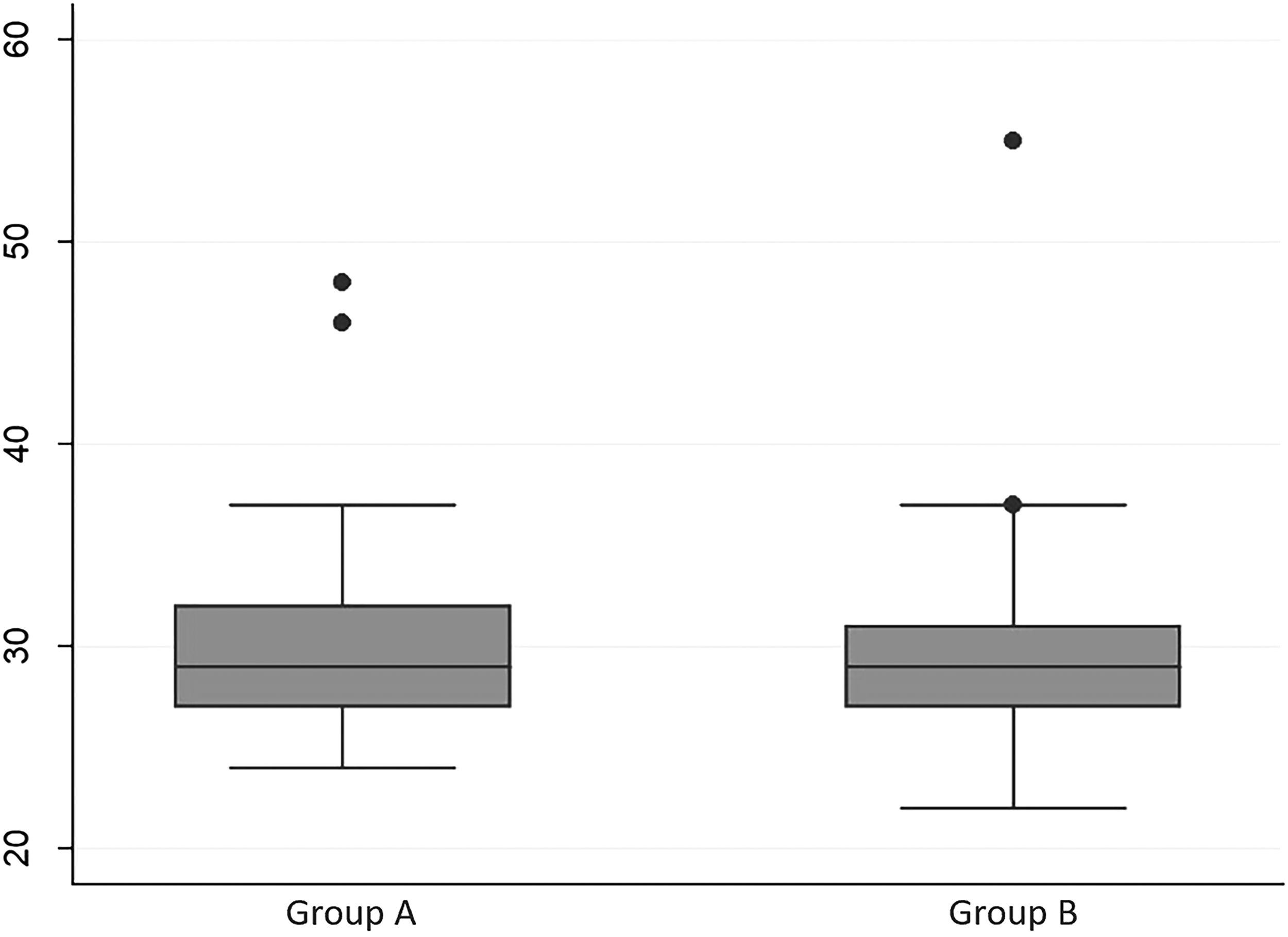
Surgical length (in minutes). Group A: fan type 5 mm retractor. Group B: retraction with suture. %PTBWL, percentage of preoperative total body weight loss.
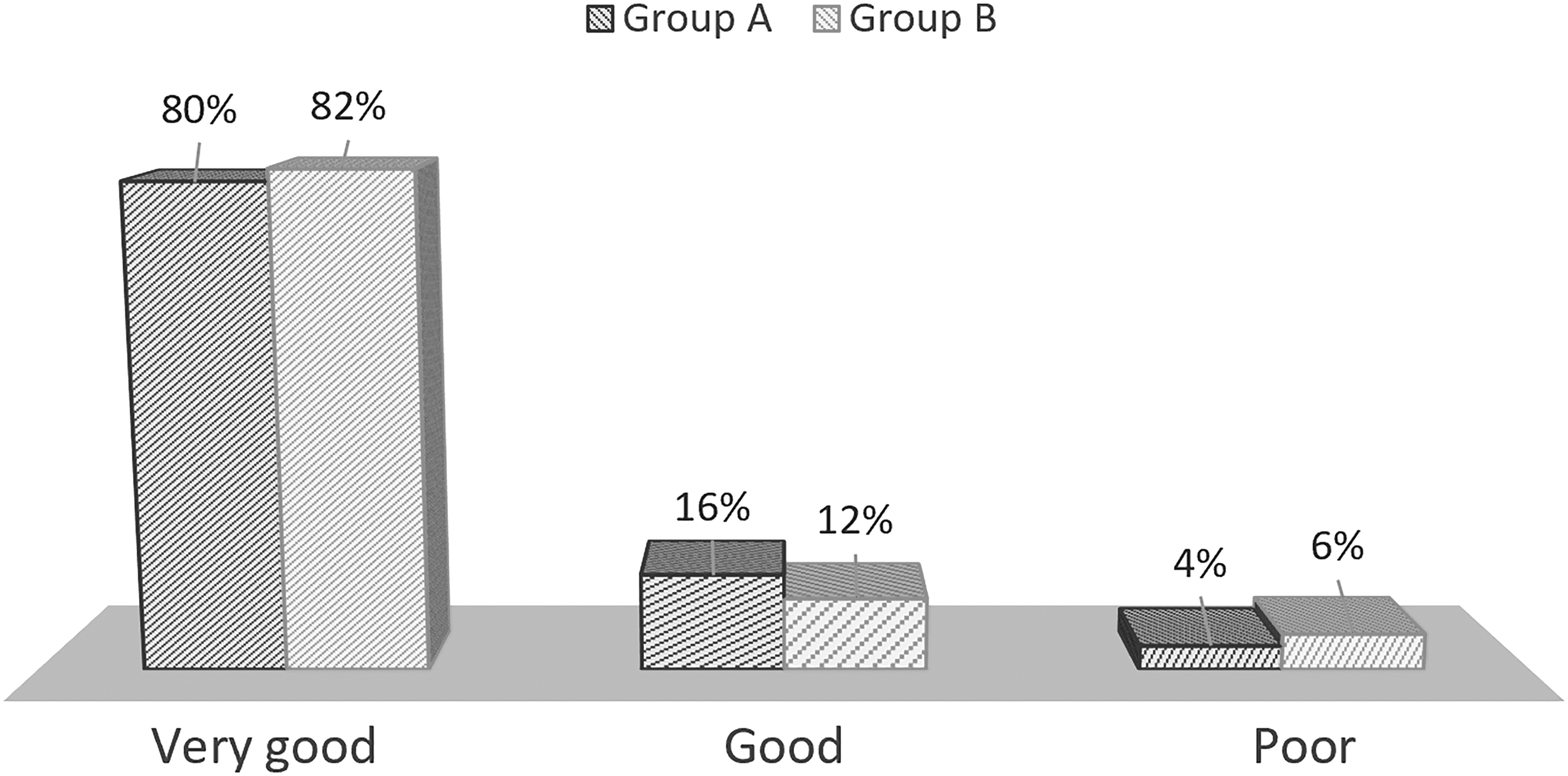
Surgical field visualization. Group A: fan type 5 mm retractor. Group B: retraction with suture.
On bivariate analysis, no significant associations were identified between surgery duration and the patient's gender, BMI, or preoperative percentage reduction in weight.
Two patients in each group (4%) suffered from minor bleeding that was attributed to the retraction technique used. All patients were reassessed at 30 days postoperatively (no drop outs), and there was no major morbidity or mortality in either group. No patient was required to stay in the hospital for more than the 24 hours, postoperatively, as is our standard practice. 9
Discussion
Laparoscopy has been documented to be superior to laparotomy, in terms of its cost-to-benefit ratio, both for the health care system and the patient.2,10 However, one of the main challenges of laparoscopy is retracting structures that surround the target tissue. Retraction involves balancing good exposure against the risk of organ injury. 11
In patients who need bariatric surgery, the liver usually has fatty infiltration, 12 which makes its mobilization difficult. Retraction of the liver also usually requires either an extra assistant or an autostatic instrument, both increasing the procedure's cost and complexity.
Different approaches to liver retraction during laparoscopic gastrointestinal surgery have been proposed. 13 More traditional methods involve inserting an instrument through a trocar or creating an incision and using either an external fixation device or assistant. These include the well-known Nathanson retractor and others.14,15 These methods provide good exposure, and the external fixation device eliminates operator fatigue. However, both can be costly and are not always available.
Other methods have been proven effective, as well. Some involve industry-manufactured devices, like the Endograb, 16 which essentially consists of a rod attached to internal fixation hooks; and the LiVac®, 17 a silicon ring that is placed between the liver and the diaphragm with a vacuum system. Both are disposable and may result in undesired extra costs.
Some surgeons utilize supplies that are already, readily available in the operating room. The V-List® 18 is a Penrose drain fixed to the diaphragm and the abdominal wall with hernia tackers. T-suspension tape 19 requires a Jackson-Pratt drain attached to a suture passed through the liver to the abdominal wall and fixated externally. Injury to the liver is a potential concern, however.
Like the technique used in the current research, Takemura et al. 20 and Saeki et al. 21 pass a suture through the left crus and place a silicon disk between the liver and the suture. This buffer has been unnecessary in our experience, however; and in none of our patients has liver ischemia become apparent or has the suture injured the liver.
Among the weaknesses of the current trial is that no liver enzyme laboratory tests were performed postoperatively to assess for liver ischemia. Also, as the sample size was calculated for surgery duration, the study was underpowered to assess morbidity. The greatest weakness, of course, is that the surgeon who rated visualization and determined the duration of each procedure was not blinded; however, such blinding was impossible, given the study's nature. The study's strengths include the randomized controlled trial design, the prior pilot study, the 100% follow-up, and that the study was conducted at a high-volume institution, which facilitated perioperative management.
The liver retraction technique described in this article is, in our opinion, the simplest and least expensive approach currently found in the literature. It involves using supplies available in any operating room, is simple to perform, and eliminates any need for expensive instruments or an additional assistant. Abdominal wall torque is minimized, which may result in less pain. It leaves no visible scars and gets rid of one of the ports usually linked to discomfort; this is especially true for women, due to their use of brassieres. We believe that other bariatric and gastrointestinal surgeries might benefit from this approach.
Conclusions
In the never-ending quest for incisionless surgery, less trauma and enhanced postoperative comfort, we found that achieving liver retraction using a polypropylene suture was both effective and inexpensive. Visualization was comparable to using a standard liver retractor, and the duration of surgery was similar. This low-cost alternative may eliminate the need for expensive instruments or additional assistants. The number of scars is reduced without jeopardizing the safety and quality of a sleeve gastrectomy. It might also be useful for other gastrointestinal surgeries.
Footnotes
Disclosure Statement
Dr. Ezequiel Fernandez and Dr. Patricio Cal are speakers and proctors for Ethicon Argentina. No competing financial interests exist for Drs Deluca, Jakob, Lonardo, and Parasporo.