
Abstract
Introduction:
Conservative management of primary obstructive megaureter (POM) appears as the best option in patients with adequate ureteral drainage. Nevertheless, surgical intervention is indicated in cases of recurrent urinary tract Infections (UTIs), deterioration of split renal function, and significant obstruction. The gold standard includes: Ureteral reimplantation with or without tapering by open approach.
Our objective is to report our results in the treatment of POM by Laparoscopic-Assisted Extracorporeal Ureteral Tapering Repair (EUTR) and Laparoscopic Ureteral Extravesical Reimplantation (LUER) and to evaluate the efficacy and security of this procedure.
Materials and Methods:
From January 2011 to January 2018 a retrospective study was carried out by reviewing the clinical records of 26 patients diagnosed with POM. All patients underwent laparoscopic ureteral reimplantation following Lich Gregoir technique. In cases of ureteral tapering, an EUTR was performed with Hendren technique.
Results:
In all patients LUER and EUTR were performed without conversion. No ureteral tapering was necessary in six patients. There were no intraoperative complications. At 3 months in postoperative, 1 patient presented a febrile UTI, and subsequently, a vesicoureteral reflux (VUR) grade III was diagnosed by voiding cystourethrogram. In this case, a redo laparoscopic surgery was performed. After long-term follow-up, all patients were asymptomatic without recurrence of POM or VUR.
Conclusion:
Laparoscopic-assisted EUTR and LUER following Lich Gregoir technique for POM constitutes a safe and effective option, with a success rate similar to that of open procedure. Nevertheless, larger randomized prospective trials and long-term follow-up are required to validate this technique.
Introduction
Primary obstructed megaureter (POM) constitutes ∼10% of uropathies, with clinical significance detected prenatally. The overall incidence of POM is in the range of 1:1500–1:2000. 1 Currently, the ureters with retrovesical diameter ≥7 mm from 30 weeks' gestation onward are considered abnormal.
The guidelines of the British Association of Paediatric Urologists (BAPU) propose that an initial differential renal function (DRF) below 40%, or a drop in DRF of 5% on serial scans, and an increasing dilatation on serial ultrasound scans are considered suggestive of obstruction. 2
Regarding the morphologic appearance of POM, the Pfister-Hendren classification established three types of megaureters: type I involved the distal ureter without associated hydronephrosis; type II extended to both ureter and pelvis; and type III was associated with severe hydroureteronephrosis (HUN) and ureteric tortuosity.3,4
Around 80% of perinatally detected megaureters are spontaneously resolved.5–7 The majority of cases of POM are managed with conservative treatment, making this approach the current option for initial medical care.2,8
Distal ureteral tailoring is often necessary to achieve an adequate length-to-diameter ratio that is required for successful nonrefluxing reimplantation. Historically, ureteral reimplantation and tapering by extravesical or transvesical open surgery has been the treatment of choice. 9
Today, there are multiple possibilities for minimal invasive treatment, including endoscopic, laparoscopic, and robotic approaches. In 1998, Angulo et al. introduced the concept of minimal invasive treatment, using balloon dilation of the ureterovesical junction (UVJ) by cystoscopy. 10 This technique has gained popularity in the treatment of POM, with good results and with the advantages of minimal invasiveness.10–15
Laparoscopic or robotic repair for POM can be performed transvesically or extravesically. Nevertheless, purely laparoscopic reconstructive surgery can be technically challenging, even for the most experienced laparoscopic surgeons.
Kutikov et al. described the first report of laparoscopic repair for POM in 2006; subsequently, different reports have described the use of Laparoscopic and Robotic repair either transvesical or extravesical ureteral reimplantation. 16 The corresponding success rate proved similar to the open procedure, making these approaches promising for the treatment of POM.16–21
The objective of this study is to report our results in the treatment of POM by Laparoscopic-Assisted Extracorporeal Ureteral Tapering Repair (EUTR) and Laparoscopic Ureteral Extravesical Reimplantation (LUER) and to compare them with the results of other approaches reported in the literature.
Patients and Methods
From January 2011 to January 2018, we retrospectively reviewed the charts in six pediatric centers for 26 patients with POM, made up of 12 females and 14 males. The mean age was 20.4 months (8–66 months); 6 had POM on the right side and 20 on the left side.
Prenatal diagnosis was carried out in 20 cases. Two patients had lower ureteral calculi, UTIs were presented in 16 patients, and 8 patients had abdominal pain.
Preoperatively, all patients underwent ultrasound, voiding cystourethrogram (VCUG), and diuretic renogram (mercaptoacetyltriglycine [MAG3]). All patients presented worsening dilatation: 4 grade III; 22 grade II; and all of them had deteriorating DRF on serial scans. The mean distal ureter diameter was 16.5 (15–25) mm. Preoperative VCUG was done in all cases without vesicoureteral reflux (VUR). In seven of the cases, and over a period of 2 months, balloon dilatation by cystoscopy with temporary Double-J (JJ) stenting was carried out unsuccessfully. All patients underwent LUER with or without tapering following Lich Gregoir technique. Detrusor myotomy was done in a vertical manner, and ureteral tapering repair was performed in accordance with Hendren technique.
All patients underwent ultrasound at 1, 3, and 6 months after surgery, a VCUG at 3 months, and MAG3 at 6 months. Thereafter, in the absence of VUR or obstruction, the follow-up was performed by clinical examination and ultrasound every 6 months.
The definition of success was in terms of significant improvement in HUN, follow-up renal bladder ultrasound and preserved, improved DRF, and/or no evidence of obstruction on functional assessment MAG3 renogram with absence of VUR during follow-up.
Statistical analyses were performed using the SPSS software package (version 20.0; SPSS), and P < .05 was considered statistically significant. Paired tests and the Wilcoxon test were performed to compare measures before and after surgery.
Surgical technique
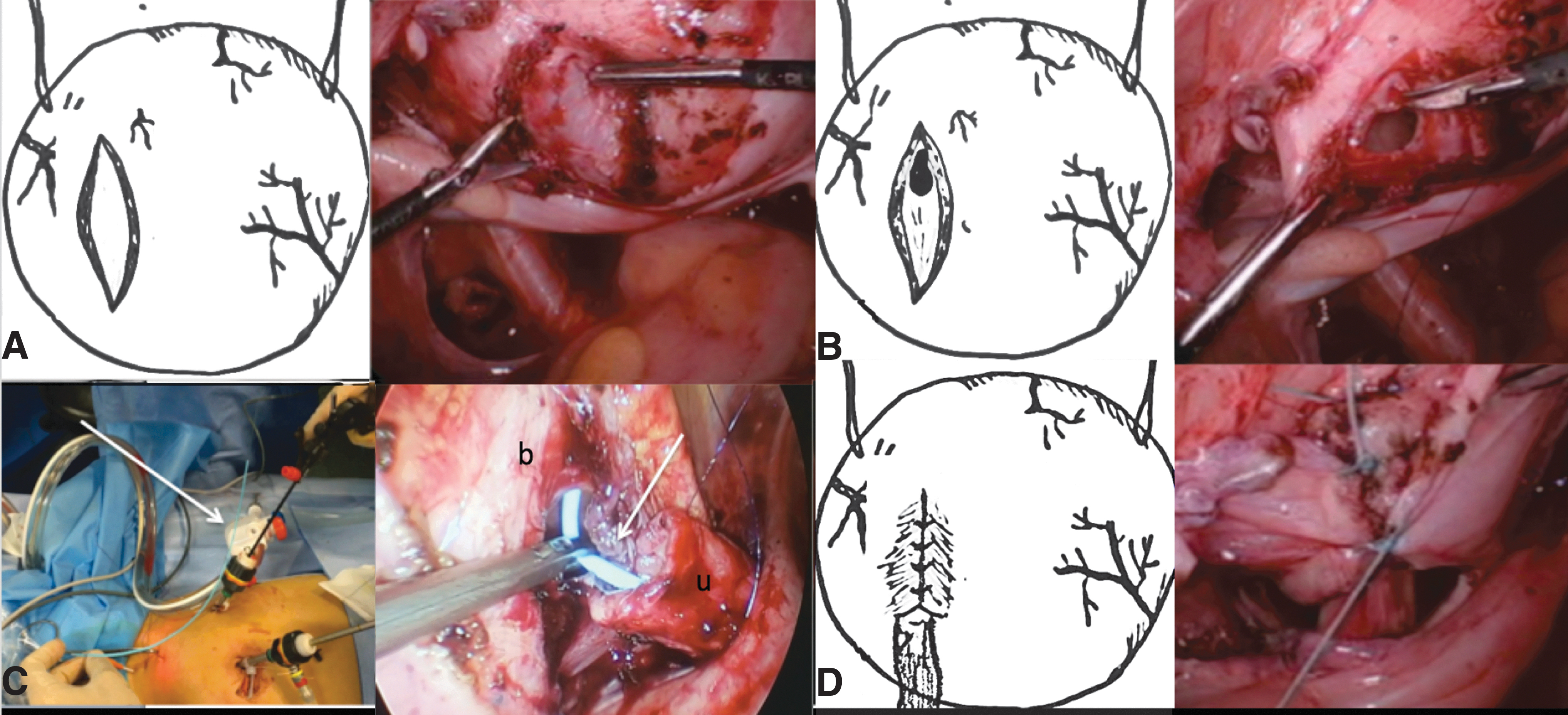
Under general anesthesia, the patient was placed in supine position with the legs apart; a urine catheter was inserted at the beginning of the surgery. Three ports were used in all cases: 5 mm-30 for the telescope and two 3 mm trocars. The surgeon was positioned at the patient's head, the assistant to the left, the nurse to the right, and the monitor at the lower end of the table. In older patients, those who are more than 8 years old, for instance, the surgeon, are positioned to the lateral position. The telescope was inserted through a transumbilical incision, and the other two 3 mm trocars were placed at the left and right lower abdomen. Two stay sutures were inserted through the abdominal wall and placed on each side of the posterior bladder to pull the anterior wall of the bladder up and to expose the UVJ. The retroperitoneum was incised to identify the distal ureter that was isolated and dissected toward the UVJ. The ureter was mobilized to achieve sufficient freedom for a tension-free reimplantation. Once the stenotic part of the ureter was completely dissected, the bladder was filled with air. Using the monopolar scissors, the peritoneum was incised to expose the muscular wall of the bladder and to create an optimal tunnel with a length that was about four times the size of the ureter (Paquin law). The detrusor muscle fibers were cautiously divided vertically, with scissors, to create a submucosal tunnel (OMIT COMMA) until the mucosa was exposed (Fig. 1A). The distal ureter was transected at the level of stenosis. In cases of ureteral tapering, the technique used was the extracorporeal Hendren procedure, with exteriorization of the ureter through the ipsilateral port, which had been enlarged to avoid tearing. Using continuous absorbable sutures, ureteral tailoring was performed. A double polyurethane pigtail soft stent Urosoft-Bard® was inserted percutaneously through the bladder in intraoperative and under laparoscopy. The ureteric stent catheter directly drains the kidney through the ureter. The distal part of the stent was left outside; it usually exits to the abdomen through the bladder wall in the suprapubic region (Fig. 1C). Vesicoureteral anastomosis was carried out after opening the bladder mucosa, using two continuous 6/0 polydioxanone sutures. The ureter was placed in the new tunnel, and the detrusor muscle was reapproximated with absorbable sutures (Fig. 1D). A nonperitoneal drain was used. During the first consultation, the stent was removed at first week after surgery.
Evolution in the technique
Two modifications were judged necessary to improve the technique: the first was the need to change the insertion point of the ureter into the bladder. During the first description one of the most challenging aspects of the technique was to perform the anastomosis in the lower part of the new tunnel because it is very laborious and time consuming. To reduce technical difficulties, the insertion point of the ureter into the bladder was moved to the top of the new tunnel (Fig. 1B).
The second important point is to avoid a second intervention to remove the stent. Currently, we are using a double polyurethane pigtail soft stent; it is inserted percutaneously through the bladder in intraoperative and under laparoscopy. It is removed at 1 week after surgery, without anesthesia, during the first consultation.
Results
From January 2011 to January 2018, 26 patients with POM underwent LUER with or without extracorporeal ureteral tapering, following Lich Gregoir technique without conversion. The first 7 cases, the vesicoureteral anastomosis, was performed in a lower part of the new tunnel (Group I); in the case of the remaining 19, the anastomosis was executed at the top of the new tunnel (Group II). In 20 patients laparoscopic assisted EUTR was carried out. The mean operative time was 141 (130–170) minutes. In 6 patients, ureteral tapering was not necessary because the diameter of the ureter was inferior to 2 cm. The mean operative time was 100 (75–120) minutes. A vertical detrusor myotomy was done in all cases. There were no intraoperative complications. The mean hospital stay was 2, 4 days (1–4 days). In the first 14 cases, the bladder catheter was removed 48 hours after surgery; in the remaining 12 cases, it was removed at the end of procedure. The JJ stent was removed under general anesthesia 1 month postoperatively. A double polyurethane pigtail soft stent Urosoft-Bard (pipi salle stent) was removed at 7 days postoperatively without anesthesia. In all patients, antibiotic prophylaxis by Trimethoprim/sulfamethoxazole was administered until the stent was removed.
The mean follow-up period was 40 (7–84) months. No urinary leakage occurred in the postoperative period. None of the patients experienced postoperative voiding difficulty. At 3 months postoperatively, 1 patient presented a febrile UTI, and VUR grade III was diagnosed by VCUG. A redo laparoscopic surgery was performed, showing partial disassembling of reimplantation; consequently, the tunnel was extended to increase the length of antireflux, and LUER following Lich Gregoir technique was performed with uneventful outcomes in long-term follow-up (Table 1).
Patients' Characteristics
DRF, differential renal function; DUD, distal ureter diameter; L, left; MAG3, mercaptoacetyltriglycine; P-H, Pfister-Hendren classification; R, right; VUR, vesicoureteral reflux.
In all cases the diameter of distal ureter was reduced. The mean diameter of distal ureter preoperatively was 16.5 (12–25) and 13.4 (9–16) mm postoperatively.
The DRF was evaluated using MAG3, showing a nonobstructive pattern, and the excretion was improved in all patients.
Statistical analysis showed significant differences in the average time of elimination on the MAG3 renogram (T1/2 55.03 versus 10.46 minutes, P < .05) obtained before and after surgery. According to these criteria, therefore, successful results were obtained in 100% of patients. With respect to the site where the vesicoureteral anastomosis was performed, we compared the patients in whom the anastomosis was performed in the lower part of the new tunnel with those in whom it was performed in the upper part of the new tunnel. Using time of elimination on the MAG3 renogram in each group, (T1/2 58.14 versus 10.42 minutes P < .018) in the lower anastomosis group versus (T1/2 53.89 versus 10.47 minutes P < .05) in the upper anastomosis group, no difference was observed in drainage regardless of the site of the anastomosis.
VCUG revealed absence of VUR in all patients. At medium-term follow-up, all patients were asymptomatic without recurrence of POM or VUR.
Discussion
Conservative treatment in POM avoids surgical correction in a maximum of 87% of patients reported in different series.5–12,22–24 The decision which favored surgical correction was based on absolute renal function. In their publication, Chertin et al. reported that renal function <30%, grade III, IV hydronephrosis, and ureteric diameter >1.33 cm are statistically significant and independent of predictive factors for surgery. 22
The gold standard for the treatment of POM includes: open surgery, excision of the aperistaltic and/or narrow ureteral segment, reduction of caliber of the distal dilated ureter, and ureteral reimplantation into the bladder in an antireflux manner, with success rates around 90%–96% in different reports. Nevertheless, complications and morbidity may occur, especially during the first year of life. The major short-term complication is urinary leakage, and long-term complications include VUR or persistent obstruction. 25
In a comparison with a historical series of open surgery by the extravesical approach for megaureters, McLorie et al. gave an account of 23 children who underwent extravesical megaureter repair. Three of them were bilateral. Only eight ureters of them were tapered. Four children had postoperative UTIs; 2 patients had stent-related complications. Transient voiding difficulty was observed in 3 children; 2 of them were bilateral and were managed by clean intermittent catheterization. Spontaneous voiding was achieved in all 3 children. 26
Concerning the age of the patient at the moment of surgery, in open surgery, higher morbidity and lower technical success are reported in children under 12 months old compared to older children. 26 In patients under 12 months old, severe difficulties in performing endoscopic treatment have been described, with the subsequent need for ureteral reimplantation. 27 In our experience, all patients benefited from the minimal invasiveness, LUER, and ureteral tapering repair, including four children under the age of 12 months.
An endoscopic approach has emerged as a minimally invasive alternative for the management of POM. Doudt et al. in 2018 researched 12 series of Endoscopic treatment for POM, which described 237 renal units in 222 patients. The success rate after a single intervention was 69.6%. After a redo endoscopic procedure, success rates increased to 79.3%. Complications included transient hematuria, UTI in 9.7%, failure to pass ureteral stent endoscopically in 9.2%, VUR in 5.1%, stone formation in 2.1%, stent migration in 1.7%, failure to advance cystoscopy through the urethra in 1.3%, and ureteral perforation in 0.8%. Only four series were routinely screened for VUR. Forty-one renal units (17.3%) progressed to ureteral reimplantation. 27
A laparoscopic approach for the correction of POM had been considered a challenge even for the most experienced. In addition, in contemporary practice, the use of LUER with or without extracorporeal ureteral tailoring for the treatment of POM is still rare, and the literature reports are scant. 3
In 2006, Ansari et al. reported the first 3 cases of LUER by the Lich Gregoir technique, with extracorporeal tailoring of the ureter, using the Hendren technique. After a 1-year follow-up, no patients presented VUR, and the renal function was preserved in all cases. 19 In 2012, Abraham et al. reported 13 cases of POM that had undergone LUER. In all cases, there was a decrease in ureteral and upper tract dilatation, as well as improved drainage. 28 In 2013, Bondarenko reported 10 cases of POM that had undergone LUER and intracorporeal plication of the ureter, using Starr technique. The mean follow-up was 13.6 months, and improvement in the dilatation of the pelvicalyceal system and the ureters occurred in all patients. 20
Our previous experience in Laparoscopic extravesical reimplantation technique, which was reported in 2017, was the basis for the development of LUER for the management of POM.29–33
At the beginning of our experience with POM, we performed the ureteral anastomosis in the lower part of the new tunnel. This was very laborious and time consuming. To become technically easier, the insertion point of the ureter into the bladder was moved to the top of the new tunnel, reducing the operative time and probably improving the quality of the anastomosis.
Another important point during surgical correction is the use of the stent. From the beginning in our initial cases, we used a standard JJ-stent placed intraoperatively by laparoscopy and removed at 6 weeks postoperatively under general anesthesia. Currently, to avoid a second anesthesia, we are using a double polyurethane pigtail soft stent (pipi salle stent); it is inserted percutaneously through the bladder and under laparoscopy draining the kidney. The distal part of the stent is left outside. It can be removed without anesthesia at 1 week during the first consultation after surgery.
Comparing the success, the endoscopic approach is approximately only 70% successful after the initial intervention, but its success increases to around 75%–80% after a second procedure. In our series, all 26 patients benefited from LUER with or without EUTR, with a success rate of 96% (Table 2).
Review of Literature
VUR is the most frequent postoperative complication in POM. Peters et al. published data on 47 infants <8 months old with POM. Of these, forty-two patients underwent open surgical correction. At a mean follow-up of 2.3 years, VUR was observed in 8 patients (19%), 3 of whom had spontaneous resolution. The 5 remaining patients were systematically reviewed, and 3 of them eventually required redo reimplantation. 34
The presence of VUR after endoscopic balloon dilatation is unknown, because a postoperative VCUG is not systematically performed. Nevertheless, the presence of VUR after this procedure is greater than after open ureteral reimplantation. In the systematic review only four series routinely screened for VUR; 41 renal units (17.3%) progressed to ureteral reimplantation.
In our series, 1 of the 26 patients (3.84%) presented a febrile UTI at 3 months postoperatively, and a unilateral VUR grade III was diagnosed by VCUG. In this case, a redo laparoscopic extravesical ureteral reimplantation following Lich Gregoir technique was done with uneventful consequences in a long-term follow-up. In our series the success rate is similar to others where surgery for POM is performed by laparoscopy.
In our experience, all cases were unilateral megaureter; the procedure was completed laparoscopically without conversion. No patient presented urinary leakage or experienced voiding difficulty.
We found that the patient's age was not a limiting factor for performance. We operated on patients younger than 1-year old with similar results to those of older patients. After long-term follow-up, all patients were asymptomatic without recurrence of POM or VUR.
In conclusion, we believe that LUER with or without EUTR for POM treatment is an alternative to open procedure with a similar success rate. It is, however, better than endoscopic treatment. It seems to be a promising technique since it offers a high success rate in a single intervention and it can be practiced in all age groups with excellent outcomes. However, the limitation of this approach is that the surgeon needs training in laparoscopic reconstructive surgery. Nevertheless, further randomized clinical trials are needed to confirm these favorable outcomes.
Footnotes
Disclosure Statement
No conflict of interest or financial disclosure has been declared by any authors.
Funding Information
No funding was received.