
Abstract
Background:
Roux-en-Y gastric bypass (RYGB) is frequently performed for weight loss purposes in the morbidly obese population. The popularity and acceptance of this procedure have increased the knowledge of the physiological (anatomical and functional) changes that this technique produces in the organism. RYGB improves gastric emptying and gastroesophageal reflux symptoms.
Materials and Methods:
We analyzed 6 patients in whom an RYGB was performed for non-bariatric purposes. Symptom questionnaire was used to evaluate response.
Results:
None of the patients qualified for bariatric surgery, as all had a body mass index (BMI) <35 kg/m2. Five patients were operated on for severe gastroesophageal reflux disease symptoms, and one for gastroparesis. All patients had good to excellent results, with marginal modification of their BMI.
Conclusion:
Non-bariatric RYGB can be considered in patients with functional diseases of the upper gastrointestinal tract, regardless of their BMI.
Introduction
Bariatric surgery has been shown to be safe and effective for weight reduction and the resolution of comorbidities associated with obesity. Within the therapeutic arsenal, gastric bypass continues to be considered the gold standard, and its use has been widely spread, 1 allowing to understand the functional changes generated by the gastric bypass in different settings such as gastroesophageal reflux disease (GERD) and gastric emptying disorders.
The technique of the non-bariatric gastric bypass will be described, as well as the fundamentals for its application for non-bariatric or metabolic purposes.
Materials and Methods
Description of the technique
Traditionally, the main mechanism of action of bariatric gastric bypass is the restrictive one and second, the hypoabsorptive component related to re-routing nutrients through the gastrointestinal tract. Currently, it is well known that besides the anatomical changes, the modification of gut hormones, microbiota and biliary salts are the main actors that explain weight loss in bariatric patients.
Taking into considerations all the factors named before, restriction is given by creating a 15-30 mL gastric pouch and a small gastrojejunal anastomosis. The lengths of the limbs that integrate a Roux-en-Y generate a transient hypoabsorption. These measurements exceed in length those made for other purposes. By modifying these aspects of the technique, we can reduce its impact in terms of weight loss.
The operating room setting is similar to that used in bariatric surgery. Trocar placement varies according to different groups.
Gastric pouch
Gastric section is made horizontally with a 60 mm linear stapler, respecting both the vascularization of the lesser curvature and the Latarjet branch of the anterior vagus nerve. The anesthesiologist introduces an orogastric tube until resting it on this line of staples corresponding to the horizontal section previously described. The creation of the pouch is completed, subsequently stapling the stomach toward the angle of His. The gastric pouch should have dimensions that ensure to minimize gastroesophageal reflux and optimize its emptying.
Biliopancreatic and alimentary limbs
The Treitz angle is identified. The section of the small bowel is performed at the second jejunal loop, 70 cm of alimentary limb is measured, and the jejunojejunostomy carried on with vascular 45 mm stapler. The common channel of the anastomosis and the mesenteric defect are both closed in the usual manner.
Gastrojejunostomy
The alimentary loop is brought to the supra mesocolonic compartment, and the gastrojejunal anastomosis is performed. This anastomosis must be wide enough (6 cm) to avoid restrictive effects at that level. Both the transverse mesocolon gap and the Petersen gap must be closed.
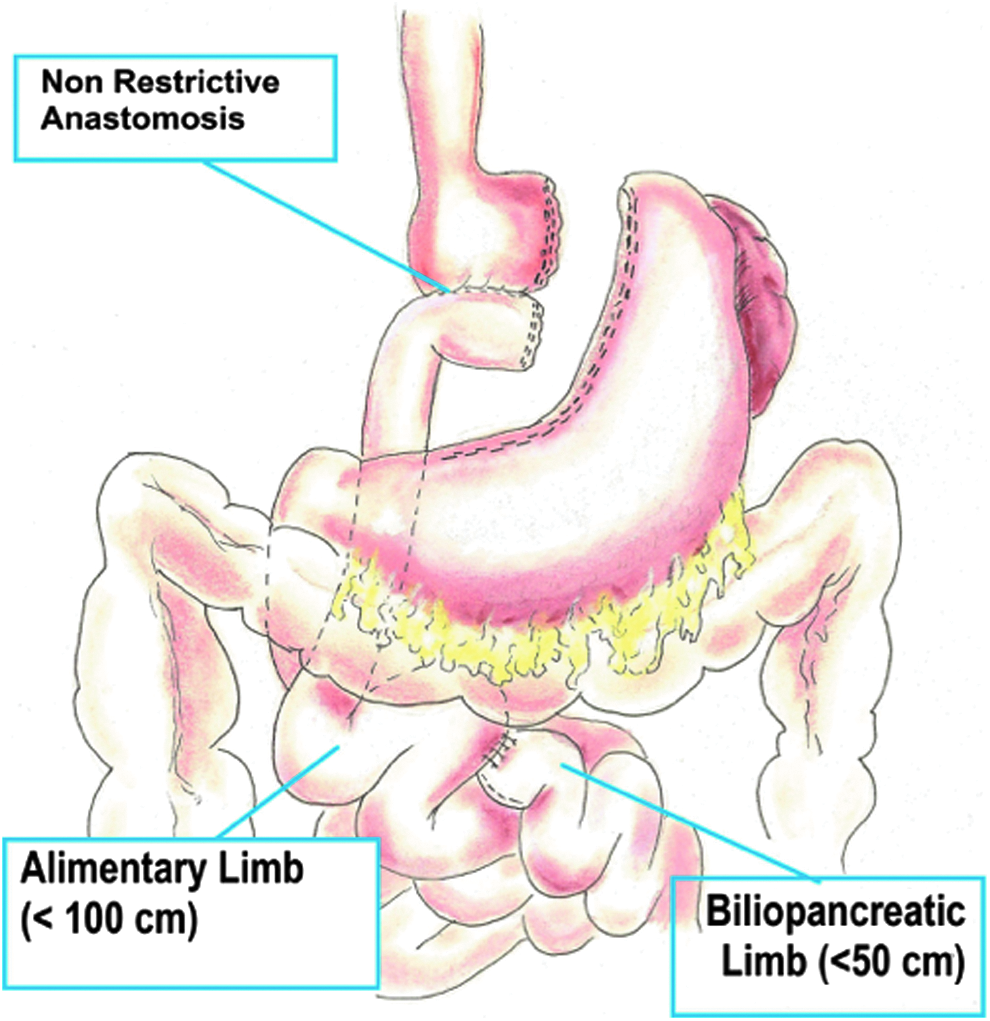
A modified gastric bypass for non-bariatric purposes is shown in Figure 1, with less restriction, and with limb lengths that mimic those used in a gastrectomy for other purposes.
A modified gastric bypass for non-bariatric purposes reduces the impact in terms of weight loss.
Indications
The previously described technique has been used to treat different functional disorders. Patients with GERD were evaluated with upper endoscopy, barium swallow, manometry, and 24-hour pH monitoring. Gastroparesis was confirmed with gastric emptying scintigraphy.
Results
Non-bariatric Roux-en-Y gastric bypass (RYGB) was performed in 6 patients with functional disease of the upper gastrointestinal tract. Five of them suffered from GERD and one of them had gastroparesis. Patient's symptoms were evaluated before and after the procedure with a symptom score. Patient's body mass index (BMI) evolution was registered. All patients had at least 1 year of follow-up. Table 1 summarizes the population evaluated and results.
Summary of Patient Population and Results
n/s, not specified.
Discussion
RYGB is considered the gold standard procedure for bariatric surgery. It has been used for years to treat severe obesity worldwide and, during the last two decades, the understanding of this technique allowed us to comprehend the modifications the procedure generates in terms of gastric emptying and reflux disease.
RYGB has demonstrated systemic benefits beyond BMI for different obesity-related diseases, and for patients with type 2 diabetes, it is now considered a therapeutic tool, even in patients with lower BMI, without nutritional complications.
With this concept in mind, it is reasonable to apply RYGB to get its functional benefits in terms of reflux control and gastric emptying symptom resolution, avoiding excessive weight loss with close dietary guidance. Non-gastric bypass has demonstrated to be effective to treat GERD, without significative weight loss in patients with BMI below 35 kg/m2.
Gastroparesis is defined as a syndrome caused by delayed gastric emptying in the absence of mechanical obstruction. It manifests with early satiety, nausea, vomiting, bloating, epigastralgia, and weight loss. 2 The first-line treatment for mild and intermittent symptoms is dietary modification. Patients with moderate symptoms are treated with prokinetics and antiemetic medication. The failure of medical treatment is followed by endoscopic attempts to alleviate symptoms. In this regard, the forced dilations of the pylorus and/or the injection of botulinum toxin at that level have been described.
The role of surgery in gastroparesis is not well established and is reserved for cases of gastroparesis refractory to medical and endoscopic treatment. Among the surgical procedures, we can mention the placement of a gastric pacemaker, gastrectomy, and the non-bariatric gastric bypass.
Although a recent review showed controversial results regarding the improvement of symptoms after the implantation of gastric electrical stimulation device (GES), 3 this system is one of the most utilized for treatment of refractory gastroparesis. Its cost represents a stumbling block not corrected by this procedure.
Another technique described for the treatment of refractory gastroparesis is total gastrectomy. 4 Of lower cost than the implantation of a gastric pacemaker, it has very good functional results, by removing the affected organ. Unfortunately, this technique leads to the possibility of serious complications that could eventually end in a fatal outcome.
One way to reduce the morbidity and mortality rate of total gastrectomy without neglecting its functional benefits to treat gastroparesis is the creation of a gastroplasty that mimics a total gastrectomy with Roux-en-Y reconstruction (non-bariatric gastric bypass).
There is scarce literature that reports the use of RYGB as a therapeutic option for the treatment of this pathology.
In 2014, Papasavas et al. studied 7 patients with a variable range of BMI (mean: 39.5, range 22–54), who suffered from gastroparesis. RYGB produced a marked improvement in symptoms. Four patients taking prokinetics drugs stopped the medications after the operation. After an average follow-up of 315.2 days, there were no postoperative complications. 5 In this publication, the authors included patients who are outside the range of bariatric surgery and applied the RYGB to treat gastroparesis regardless of their BMI.
The following year, Sun et al. performed at the Cleveland Clinic a review of all morbidly obese patients (BMI 35 kg/m2), who underwent GES or Roux-en-Y gastrojejunostomy with or without total gastrectomy (RYGJ) as a treatment for refractory gastroparesis. The main objective of the study was to examine the evolution of symptoms, postoperative complications, and change in BMI. There were 20 patients (15 women and 5 men) who underwent GES placement. A total of 7 patients (6 women and 1 man) underwent RYGJ; among them, 4 patients were converted to RYGJ by failed response to GES placement.
The operating time was significantly longer in the RYGJ than in the GES implantation (P = 0.01). However, this did not affect the hospital stay. The long-term improvement of symptoms was achieved in 11 patients (55%) in the GES group and in 5 patients (71%) in the RYGJ group (P = 0.68). The RYGJ group had a similar morbidity to the GES group (14.3 vs. 15%, P = 1). No mortality was reported in the shortand long-term follow-up in the RYGJ group.
Based on their results, Sun et al. conclude that laparoscopic RYGJ is an effective treatment for refractory gastroparesis and that it can be performed with an acceptable complication rate. Above all, it is an acceptable strategy in patients in whom GES placement failed, since they had a 100% improvement in symptoms in the short term, after conversion to an RYGJ. 6
Recently, Wakamatsu et al. 7 found that there were no significant differences between RYGB and GES in complication rates (6% versus 0%), readmission rates (6% versus 17%), and reoperation rates (6% versus 21%). For the authors, both treatments are feasible for refractory gastroparesis. In conclusion (Table 1), based on these studies, gastric bypass would seem to be a safe operation for refractory gastroparesis, with a low risk of complications in the hands of trained surgeons.
Our series includes 1 patient with diagnosis of gastroparesis, refractory to conservative treatment, in which RYGB perfectly controlled the symptoms generated by this uncommon functional disease (Table 2).
Control of Symptoms After Roux-en-Y Gastric Bypass
Non-bariatric Roux-en-Y gastric bypass: bigger pouch, wider gastrojejunostomy, and shorter biliopancreatic and alimentary limbs than a standard gastric bypass performed for weight loss purposes.
BMI, body mass index; GERD, gastroesophageal reflux disease.
GERD affects ∼20% of the population in the United States. Occasionally, it is associated with obesity. 8
For the diagnosis and quantification of GERD, functional tests are needed. Symptoms are usually unreliable for these purposes.
The Lyon consensus considers its diagnosis only with specific endoscopic findings such as cases of severe esophagitis (grades C and D of the Los Angeles classification), Barret's esophagus or peptic stenosis, or when the time of exposure to acid in the esophagus is greater than 6% of the time studied through 24-hour pH monitoring. 9
The conception of a surgical procedure that treats the etiological agent of esophageal sequelae is attractive, acting secondarily on the mucosal alteration.
In this context, the gastric bypass appears again as a procedure that could provide substantial benefits, and that could go beyond weight loss objective. This operation also turns out to be an excellent antireflux technique, since it isolates the esophagus from gastric and duodenal secretions, positively impacting the patient's symptoms.10–15
Among the anatomical and physiological changes it produces, we will mention three relevant facts:
The small gastric pouch contains a smaller mass of parietal cells and therefore, the production of acid to which the esophagus is exposed is minimized.12–14
Compared with a normal stomach, gastric bypass is associated with more rapid emptying, thus decreasing the acid exposure time.
13
Roux-en-Y configuration avoids exposure of the esophagus to duodenal contents.12–14
It is clear that the results of antireflux surgery (Laparoscopic Nissen fundoplication) in patients with a BMI >35 are not encouraging; and in these cases, most surgeons choose to approach the patient as a bariatric one and treat simultaneously these concomitant entities with an RYGB. 16 The increase in intra-abdominal pressure (obesity) is a known risk factor for the failure of a fundoplication, with subsequent recurrence of reflux.
However, when specifically analyzing patients with overweight (BMI between 25 and 30) and obesity class I (BMI 30–35), these results are even more controversial. While studies like that of Morgenthal et al. 16 and Luketina et al. 17 in the analysis of subgroups with overweight and obesity class I did not find worse results with a Nissen fundoplication, Schietroma et al. 18 found that both groups, overweight patients and those with obesity class I, had reflux recurrence rates significantly higher than those observed in subjects with normal weight.
In this discussion of what would be the best technique to treat gastroesophageal reflux in patients with overweight and obesity class I, outside the range of bariatric surgery, it would not be unreasonable to think about the utility of non-bariatric RYGB.
With this concept, Rosenthal et al. 19 in their report of 59 patients submitted to an RYGB for non-bariatric purposes, patients with gastroparesis or GERD represented 28.8% of the cases as a whole.
Author's series includes 5 patients with intractable complicated GERD, in whom RYGB allowed symptom control (Table 2).
Failed previous antireflux surgery is another indication for this modified bariatric procedure. Patient satisfaction with primary antireflux surgery is high. The control of symptoms is achieved in ∼80%–90% of patients, even 10 years after a fundoplication.20,21 However, a percentage of patients experience symptoms that justify a re-intervention. Recurrent reflux, dysphagia, pain, and bloating are some of the manifestations of failure.
Once the patient has been evaluated and the re-operation indicated, this population becomes a real challenge for the surgeon. Redo Nissen is a technically demanding procedure, with a success rate lower than the primary procedure and higher morbidity and mortality rates.22,23 The RYGB is an effective procedure for this subset of patients,24,25 which prevents reflux by changing the mechanism of action of the procedure. Some authors report that it may represent a good alternative, even superior to a re-fundoplication in obese patients.26–28 The procedure achieves an excellent symptomatic control of reflux and has been shown to improve patient's quality of life, with acceptable perioperative morbidity.29,30 Therefore, it should be seriously considered in the treatment of obese patients after failures in a fundoplication, and in those cases in which the reconstruction of the GE junction is extremely difficult (for example: limited hiatal dissection, inability to obtain an adequate length of intra-abdominal esophagus or achieve the crural approach).30,31
Scleroderma is a systemic autoimmune disease, characterized by abnormal collagen deposition in tissues, vasomotor alterations, and extensive fibrosis.32,33 The gastrointestinal tract is affected in 90% of cases and the most involved segment is the esophagus. 34 Reflux is a frequent problem in these patients and is mainly caused by the combination of a motor disorder that alters the normal emptying of the esophagus, and an incompetent lower esophageal sphincter. 35 Gastroparesis, present in up to 50% of these patients, contributes to reflux,35,36 along with the poor production of saliva.
Fundoplication in this population is associated with postoperative dysphagia that varies by 30% to 70% according to the different series. 35 In this context, non-bariatric RYGB emerges again as a reasonable strategy to provide excellent control of reflux, together with a lower risk of dysphagia and concomitant improvement of gastric emptying.
Kent et al. 35 presented his experience in the treatment of GERD involving patients with scleroderma. A total of 23 patients were studied. Five patients underwent esophagectomy, 10 patients a fundoplication, and 8 patients a modified RYGB. In the RYGB group, the presence and severity of dysphagia were significantly lower compared to the fundoplication group. The GERD-HRQOL score was also significantly lower in the RYGBP group. Both fundoplication and RYGB were performed without significant morbidity.
Recently, Yan et al. 37 analyzed 14 patients with scleroderma and GERD. Seven underwent fundoplication and another 7 underwent modified RYGB. Five patients with RYGB, who had symptoms of GERD, had an improvement or resolution of the symptoms, while only near 50% (n = 3) of the patients with fundoplication reported a partial improvement.
The surgical technique performed in these studies was similar, having in common the modification of the gastrojejunal anastomosis and the length of the alimentary loop, to reduce the impact on weight loss. This was achieved with a larger and less restrictive gastrojejunal anastomosis, and with an alimentary limb length of less than 100 cm.
Other indications of a non-bariatric gastric bypass include cases of upper mesenteric artery syndrome and complications of gastric surgeries. 19
Conclusions
The RYGB is one of the most widespread procedures for obesity surgical treatment. Its use has allowed standardizing the technique, thus reducing morbidity and mortality rates. This experience exposed the positive impact of this procedure on different functional disorders of the upper digestive tract. In light of these results, the RYGB has been modified to obtain a procedure that can be used for non-bariatric purposes. Experience has shown that its application to diseases, such as GERD, gastroparesis, and failure of a previous antireflux procedure, carries functional benefits and puts it in a place to be considered when facing patients suffering from these disorders.
Footnotes
Disclosure Statement
No competing financial interests exist.