
Abstract
Introduction:
The management of primary spontaneous pneumothorax (PSP) in children still remains controversial. The current literature shows a lack of scientific evidence supporting a standardized management.
Materials and Methods:
A multicenter retrospective study was performed, patients admitted for PSP in five Pediatric Surgical Units over a 9-year period (from 2008 to 2017) were included. Patient data were reviewed for each case. Management and outcomes were statistically analyzed.
Results:
Overall 159 patients (135 males and 24 females) were included in this study. During the first hospital admission, 62/159 patients (39%) were conservatively managed with oxygen therapy; 95/159 patients (60%) required a chest drain insertion; 2/159 patients (1%) underwent surgery because of a bilateral pneumothorax. Thoracoscopy was performed in 75/159 (47%) patients after the second hospital admission or for persistent air leak during the first access. Postoperatively, 8/75 (11%) patients developed recurrent pneumothorax requiring chest drain insertion in 3/8 (37%) cases or aspiration in 1/8 (13%), whereas 4/8 (50%) patients were conservatively managed. All of the patients but one, were confirmed to be affected by emphysematous-like changes at histology.
Conclusions:
Despite the limitations of being a retrospective study, we suggest that the early surgical management in children with PSP is feasible and safe and it seems to significantly reduce the recurrence rate. To the best of our knowledge there are no pediatric guidelines for the management of PSP, therefore, we support the need for prospective studies to create the evidence-based pillars for correct and standardized management of this condition.
Introduction
Primary spontaneous pneumothorax (PSP) is a rare condition occurring in healthy adolescents and young adults in the absence of an underlying intrinsic lung pathology. Its incidence is 3,4:100.000 children >18 years of age 1 with a male to female ratio of 4:1. 2 The vast majority of children present the same physical characteristics: tall stature and slight build physique. 3 The exact number of PSP in children is not exactly known since pediatric studies are usually published in literature mixed with the adult population, which makes it really difficult to extrapolate the pediatric data.4,5 The main aim of PSP management is to treat the acute episode, potentially life threatening, and to prevent recurrence with minimal morbidity; this goal might be achieved either by a conservative approach (such as oxygen therapy and chest drain) or a surgical one. Currently, there is no consensus between pediatricians and pediatric surgeons regarding the formulation of guidelines for the management of PSP in children, so the current recommendations are based on adult data. 6 Based on the growing popularity of the minimally invasive approach, some surgeons advocate for early surgical intervention as the definitive treatment for PSP leading to the resolution of the condition and to an earlier resumption to the daily activities.7,8 However, on counterparts, some surgeons might argue that the surgical approach should be reserved to those children who fail conservative management (because of either persistent communication with the pleural space or recurrent disease).9,10
Still controversial is the timing for computed tomography (CT) scan as well as the indication for early surgery in patients with a CT scan suggestive of asymptomatic apical blebs on contralateral lung (opposite side of PSP).2–10 The aim of this multicenter study was to see the type of radiological investigations used for the diagnosis of PSP in children in each center, analyze the favorite approach used for its treatment (either conservative or surgical), and finally evaluate patient outcomes to establish a possible shared pattern of treatment for the management of pediatric PSP.
Materials and Methods
Following the institutional approval, a retrospective observational multicenter study was performed. All of the patients treated for PSP over a 9-year period (from January 2008 to December 2017) in five Italian tertiary centers were included in this study. Data were extrapolated from departmental database, clinical notes were reviewed as well. Children and adolescents <18 years of age, admitted for an episode of PSP were included in the study. Patients were identified using ICD-9-CM codes for diagnosis, imaging studies, and procedures were also considered. Exclusion criteria were: presence of severe comorbidities (trauma, Marfan syndrome, cystic fibrosis, iatrogenic pneumothorax) and incomplete data.
Demographic data (age, sex, race, body index mass, kg/m2), clinical features (chest pain, shortness of breath, asthenia, number of unilateral or contralateral PSP episodes), imaging studies (X-ray, CT scan), initial and following treatments (conservative or operative), length of hospitalization and patient outcomes (postoperative complications, follow-up) were reviewed. When PSP was suspected by the clinical examination in the emergency department, a chest X-ray was requested. A “large” pneumothorax was defined when a visible rim of >2 cm between the lung margin and the chest wall (at the level of the hilum) was identified (as described by BTS guidelines).
CT scan was required in those patients who had a previous history of spontaneous pneumothorax or suggested after the first episode for documenting the presence of unilateral or bilateral apical blebs. The surgical procedures performed were: blebs resection, pleurectomy, mechanical or chemical pleurodesis, or a combination of both. A chest tube was left in situ after surgery and removed once lung expansion was satisfied at X-ray control. The considered patient outcomes were: recurrence rate following the conservative approach, length of hospitalization (according to the different procedures), timing for CT scan, length of persistency of air leak from the chest drain before performing surgery, long-term recurrence rate after surgery, and recurrence rate of pneumothorax in patients with contralateral asymptomatic blebs. Data were statistically analyzed. Categorical variables were compared using Chi-square, whereas Mann–Whitney test was used for continuous ones. Results were considered significant if P-value was <.05.
Results
Overall, 159 patients (135 males and 24 female) were identified over a 9-year period (Table 1). Eighty-five percent of the patients complained about chest pain, generally on the left side (64%). Mean age was 15.8 ± 1.2 years (range 12–17 years), with a male/female ratio of 6:1. Five percent of the patients had a familiar history of pneumothorax while smoking habit was referred by the 20%. Following the first episode, a contralateral PSP was reported in 26/159 (16%) cases. Chest X-ray showed 112 large PSP with images of bullae in 12 cases. The risk of recurrence (Fig. 1) was found to be significantly higher in patients presenting with a large PSP (P < .0001) when compared with patients presenting with a small PSP. CT scan was performed in 132/159 (83%) children, 97/132 (76%) cases at the second recurrent episode. A total of 37/159 (23%) patients presented with visible apical blebs at the chest CT scan. The finding of the blebs at CT scan affected both the lungs in 24/37 (65%) patients. A total of 11/132 (8%) patients with evidence of bilateral blebs at CT scan did not present episodes of PSP at this side. The association between recurrent PSP and presence of blebs (identified at the CT scan of the chest) was found to be statistically significant (P < .05) (Fig. 2).
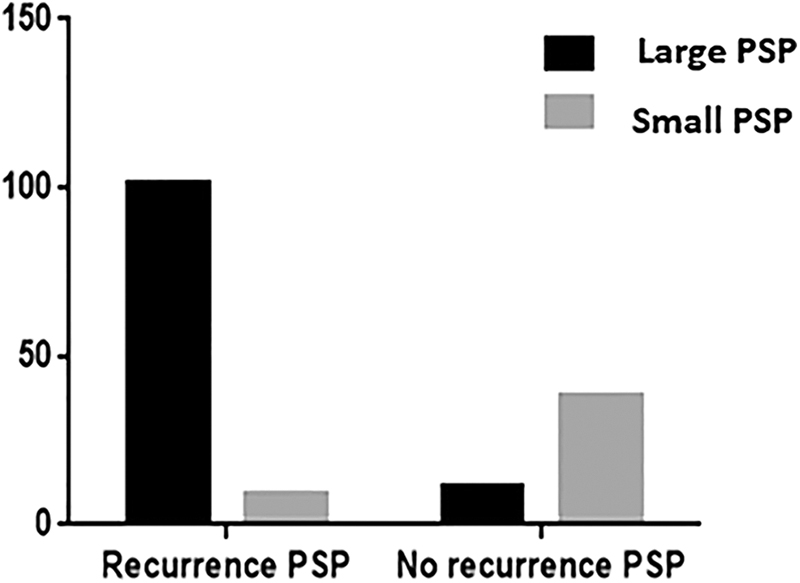
The risk of recurrence between large and small PSP. PSP, primary spontaneous pneumothorax.

The risk of recurrent PSP in patients with confirmed apical blebs at CT scan. CT, computed tomography; PSP, primary spontaneous pneumothorax.
Patient Demographics, Initial Management, and Clinical Outcomes by Recurrence
CT, computed tomography; LOS, length of stay; PSP, primary spontaneous pneumothorax.
A total of 62/159 (39%) patients were conservatively managed by oxygen therapy with a recurrence rate of 58%, chest drain insertion was required in 95/159 cases (60%) with a recurrence rate of 51%, whereas thoracoscopic procedure was performed in 2/159 (1%) bilateral PSP as a first approach. No statistically significant difference was found as far as the recurrence rate was concerned in the two groups that were conservatively managed. The evaluation of these data highlights a diffuse tendency to use the chest drain in patients with large PSP leading to a consequently longer length of stay (LOS) (P < .05, 6.3 ± 3.3 versus 7.7 ± 1.2 days; Figs. 3 and 4 and Table 1). Following the initial nonoperative management, 40% of the patients experienced an ipsilateral recurrence at a median time of 6 months (range 4–14 months). A total of 75/159 (47%) patients underwent thoracoscopic surgery, of which 11/75 patients (15%) were after an initial conservative approach and 64/75 patients (85%) during the following admissions. Indications for the surgical intervention were: persistent air leakage (15%), recurrent ipsilateral pneumothorax (57%), contralateral pneumothorax (19%), and prophylactic surgery on asymptomatic contralateral lung (9%). In summary, we performed a thoracoscopic procedure with a stapler wedge resection of the apical lung in 69/75 cases (92%), of which 27/69 cases (39%) were associated with mechanical pleurodesis, whereas 15/69 (22%) were completed by pleurectomy, and 4/69 (6%) patients with combined mixed procedures. Thoracoscopic lung apicectomy was completed by chemical pleurodesis in 7/69 patients (10%) and by an association of previous procedure and pleurectomy in 7/69 patients (10%). The remaining 9/69 cases (13%) underwent apicectomy only, which was considered as satisfied. When no evidence of blebs was demonstrated at the apex, some surgeons decided to perform only mechanical (4%) or chemical pleurodesis (4%).
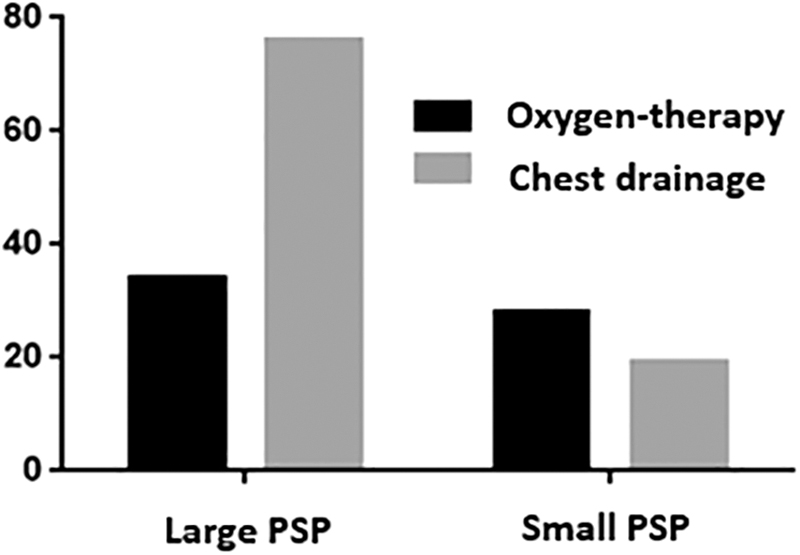
Comparison between the use of the chest drain or oxygen therapy for patients with large PSP. PSP, primary spontaneous pneumothorax.
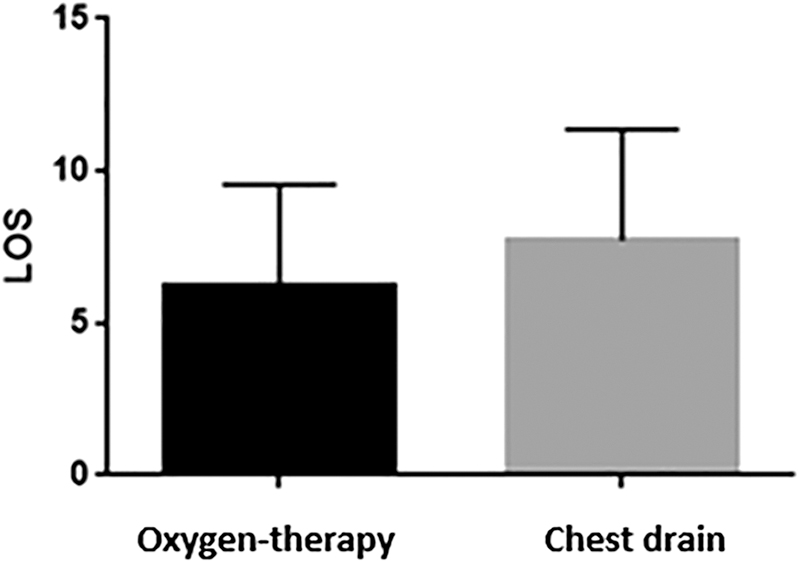
Length of hospitalization for different types of conservative management.
Overall, the chest drain was left in situ for 3 days (range 1–6 days). Postoperative complications were represented by air leak (15%) and Bernard–Horner syndrome (4%). Following the surgical procedure, recurrence occurred in 8/75 patients (11%); recurrences were treated by chest tube insertion in 3/8 (37%), aspiration in 1/8 (13%), or conservatively in 4/8 (50%). Recurrence rate was significantly higher in children treated by apicectomy only (50%). In all cases, histological results showed emphysematous-like change, except for one. Mean follow-up was 19.6 ± 4.1 months (range 12–28 months). No long-term complications were reported.
Discussion
PSP is a rare condition in the pediatric population, it is characterized by a high recurrence rate and morbidity that negatively impacts on quality of life of both patients and their families. Many controversies exists about the management of PSP in children and adolescents. The main issues are related to the conservative management represented by oxygen therapy versus chest drain insertion; another issue is represented by the correct timing for surgery and its indication. Other disputed points are the correct timing for the chest CT scan and the surgical management of the contralateral lung with evidence of blebs at CT scan. The etiology is also unclear and it is generally well accepted that PSP results from the rupture of blebs or bullae at the apex of the lung. 11 The physical development causes a rapid increase of the vertical axis size of the thorax with respect to the horizontal one leading to a higher negative pressure at the apex where mechanical stresses are higher. These events will eventually cause the formation and the breakage of the lung blebs. 12 Smoking is also a well-known risk factor for PSP, although not correctly considered in a pediatric population. 13 In our series, only 20% patients were smokers. The main goal of management of PSP is to resolve the acute episode and to prevent recurrence, reducing morbidity. 14 The recurrence rate following the first PSP episode is higher than in the adult population with values ranging from 30% to 60%. 15
In our study, we found a rate of 53% compared with the percentage reported in literature, and these data are very important for choosing the best management in young patients because the risk of recurrence limits their daily life. In accordance with our results, we found that some authors advocate an early surgical treatment for PSP in children and adolescents; however, the paucity of published data about PSP management within the pediatric age, as well as the lack of evidence in terms of preventing managements to reduce the recurrence rate, make it difficult to identify a standardized approach. 16 The accepted treatment at the first episode of PSP in accordance with both adult guidelines of the British Thoracic Society (BTS) and the American College of Chest Physician (ACCP), should be guided by the presence of symptoms and by the size of the pneumothorax at a chest X-ray.
The current management of small PSP is represented by high-flow oxygen administration, which facilitates the reabsorption of air in the pleural cavity, although resolution of the pneumothorax seems slower if managed in a conservative way. 17 Conversely, the presence of a large pneumothorax is considered as the main indication for the insertion of a chest drainage. In our study, all of the patients, with the exception for 2 patients with a bilateral PSP, were treated conservatively. The length of hospitalization was significantly longer for patients receiving chest drain insertion rather than those treated by oxygen therapy alone. Eleven patients receiving chest drain insertion, had an unfavorable clinical course with a persistent air leak (over 5 days) leading to surgery.
Since the conservative management is associated with high failure rate, 18 some authors suggested that <40% of pediatric patients with PSP were definitively treated without surgery. 19 In our study, the overall recurrence rate for patients undergoing the conservative approach was 53% (in line with pediatric literature).3–20 By the evaluation of our data, it seems reasonable to offer the conservative management (based on only oxygen therapy) to the clinically stable patients with small PSP. Equally, patients showing a large PSP at the chest X-ray, but clinically stable, can be conservatively treated over the first 48–72 hours from initial presentation. Nonetheless, cases showing a clinical deterioration will be a candidate to chest drain insertion.
However, wider cohort studies or prospective studies, are needed to understand whether (in view of a high rate of recurrence after the first episode) an immediate surgical approach would be the best option for these patients. Our data suggest that the highest risk of PSP recurrence occurs between the first and the sixth month following the first episode. Patients should be counseled regarding avoiding activities involving a sudden change of lung and pleural pressure, such as flying or diving for at least 1 year following the first episode of PSP. It seems clear that this might play an important psychological role, as a life-limiting condition. Some authors highlight the importance of identifying the presence of blebs at the CT scan following the initial presentation of PSP, 14 although the role of their presence on recurrence rate is not well defined and other authors do not support such approach. 21 We found apical lung blebs in 37 cases and still the rate of recurrence was not related to these findings. Nowadays, thoracoscopy is considered the gold standard for minimally invasive treatment of PSP. Moreover, there is a wide consensus regarding the apicectomy/blebectomy procedure combined with pleurectomy/pleurodesis as the best approach for the treatment of PSP with a low recurrence rate.9–22 The pleurodesis seems to be determinant in preventing postoperative recurrence. 23 In our series, 80% of apicectomy was associated with a higher recurrence rate in patients treated by apicectomy only. Another controversy is represented by how to treat the contralateral apical blebs in absence of symptoms. 24 The paucity of data in the current literature regarding the treatment of controlateral asymptomatic apical blebs still does not justify the surgical indications to remove them.
However, due to the limited quality of life of patients, the high recurrence rate, and the unpredictability of this condition, some centers are opting for an early surgery. On the basis of our retrospective data, we propose a management algorithm in case of the first PSP (Fig. 5) episode and ipsilateral recurrence or contralateral PSP episode (Fig. 6).

Proposal of management algorithm in the case of the first episode of PSP. PSP, primary spontaneous pneumothorax.
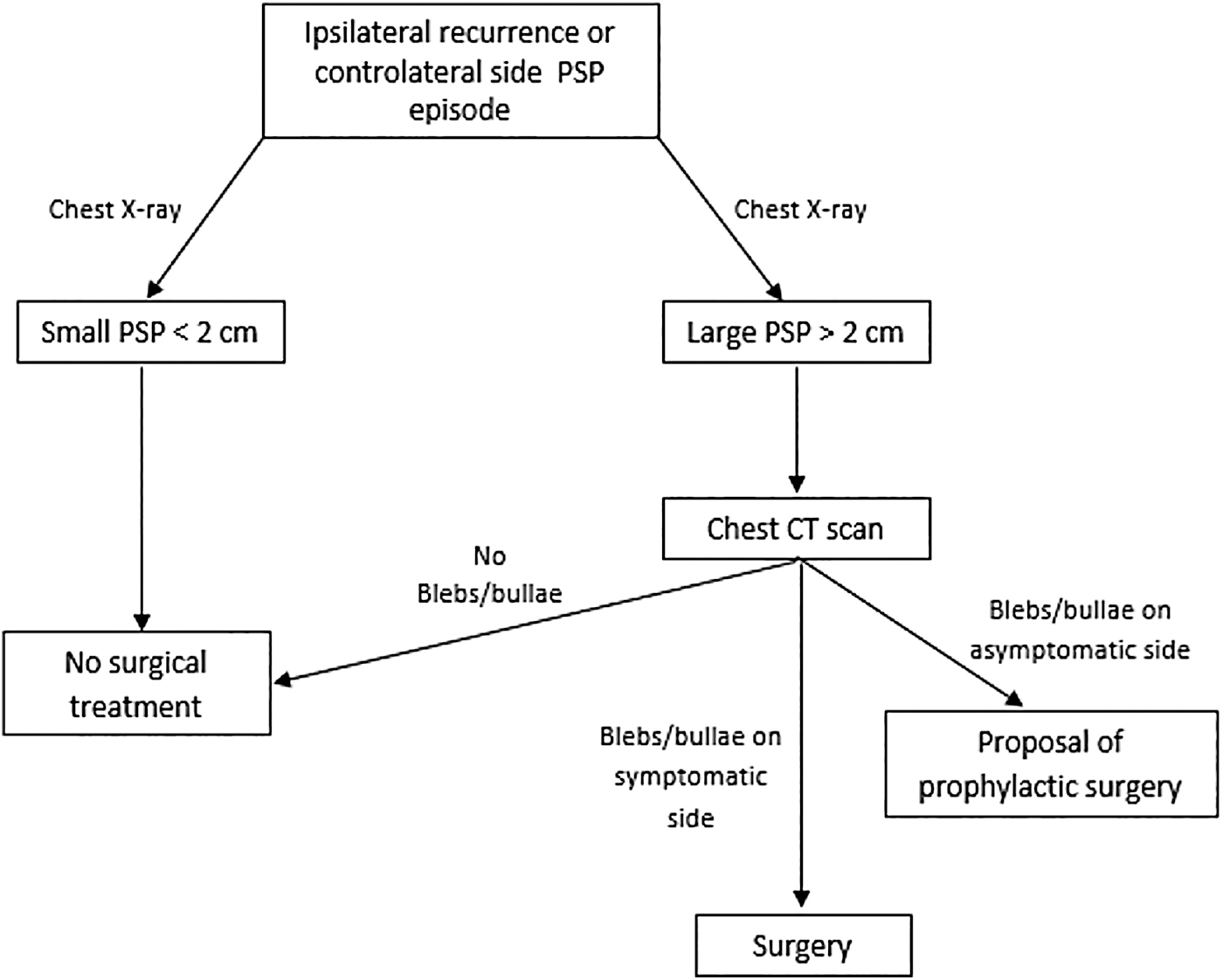
Proposal of management algorithm in the cases of ipsilateral recurrence or contralateral PSP episode. PSP, primary spontaneous pneumothorax.
Conclusion
The present study has some limitations, first it is retrospective in nature. Due to the paucity of published data in pediatric age, we strongly support further prospective multicentric studies, either national and international, to find predictive recurrence factors and try to standardize diagnostic and operative management for the treatment of PSP in children and therefore set up guidelines based on pediatric evidence.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.