
Abstract
Background:
Gastrostomy tube placement (G-Tube) is a frequently offered procedure in children with feeding difficulties. Various procedures exist for G-Tube, with the pull technique more commonly used for a percutaneous endoscopic gastrostomy (PEG) in children, considered by many to be the safer approach. Major complications requiring reoperation range from 3% to 5%, depending on the study. In our center, PEG placement is performed by gastrointestinal endoscopists through the pull technique. In the last 5 years, there were 150 procedures, with 15 minor and 3 major complications. We will describe the last 3 cases, plus a fourth PEG placement at another center.
Patients and Methods:
Patients ranged from 2 to 10 years (median age: 4.5 years). Median weight was 10.7 kg (range: 7–18 kg). Patients were neurologically impaired children, except one with severe nephropathy.
Results:
Laparoscopic repair with a 3-trocar technique was effective, when the patient's general condition allowed for it. After fistula repair, a new gastrostomy was placed; this step can be performed endoscopically under laparoscopic control (or can be performed completely laparoscopically).
Conclusions:
In 4 patients, we faced unusual PEG placement complications, due to colon interposition during blind gastric puncture. In those with anatomical deformities or previous surgery, or dealing with toddlers (under 10 kg), we suggest laparoscopic-assisted PEG, or a full laparoscopic gastrostomy to avoid the risk of a major complication.
Introduction
Gastrostomy tube placement (G-Tube) is done in children with feeding difficulties. Indications include: severely neurologically impaired (NI) children, failure to thrive, esophageal atresia, dysphagia, and short bowel syndrome. Various procedures can accomplish this: the Stamm open approach, percutaneous endoscopic gastrostomy (PEG), full laparoscopic approach, combined endolaparoscopic LAPEG (laparoscopic-assisted percutaneous endoscopic gastrostomy), and laparoscopic-assisted gastrostomy (LAG).
For PEG placement, two techniques are commonly used: the Ponsky/Gauderer pull method and the Sachs-Vine push technique (Seldinger technique). The pull technique is used in children, considered to be the safer approach.
The reported rate of complications following PEG vary from 16% to 70%, including minor and major conditions. 1 Major complications requiring reoperation range from 3% to 5%, along with the specific study. More frequent minor complications are peristomal wound infection, tube obstruction or fragmentation, leakage around the tube, migration through the small bowel (ileus), cellulitis, and hematoma.
Major complications are sepsis, peritonitis, migration through the gastric wall, perforation, fistula, hemorrhage, necrotizing fasciitis, tumor implantation at the stoma, aspiration, intra-abdominal abscess, and gastric outlet obstruction.
In our center, PEG placement is performed by gastrointestinal endoscopists through the pull technique. In the last 5 years, 150 procedures have been performed with 15 minor and 3 major complications. In the next section, we describe the last 3 cases, plus a fourth PEG placement performed in another center.
Case Gallery
Case 1
The patient was a 4-year-old NI child referred from another hospital in March 2018. The PEG procedure was performed 6 months earlier: since that time, the child had suffered from persistent diarrhea, attributed to malabsorption. Purulent secretions from the peristomal skin were noted and attributed to a granuloma. However, normal growth was present.
A contrastogram through the gastric tube revealed direct injection of the contrast agent into the colon, so a diagnosis of gastrocolocutaneous fistula was proposed (Fig. 1). Laparoscopic repair was easily performed, thereby including a new gastrostomy, without postoperative complications.
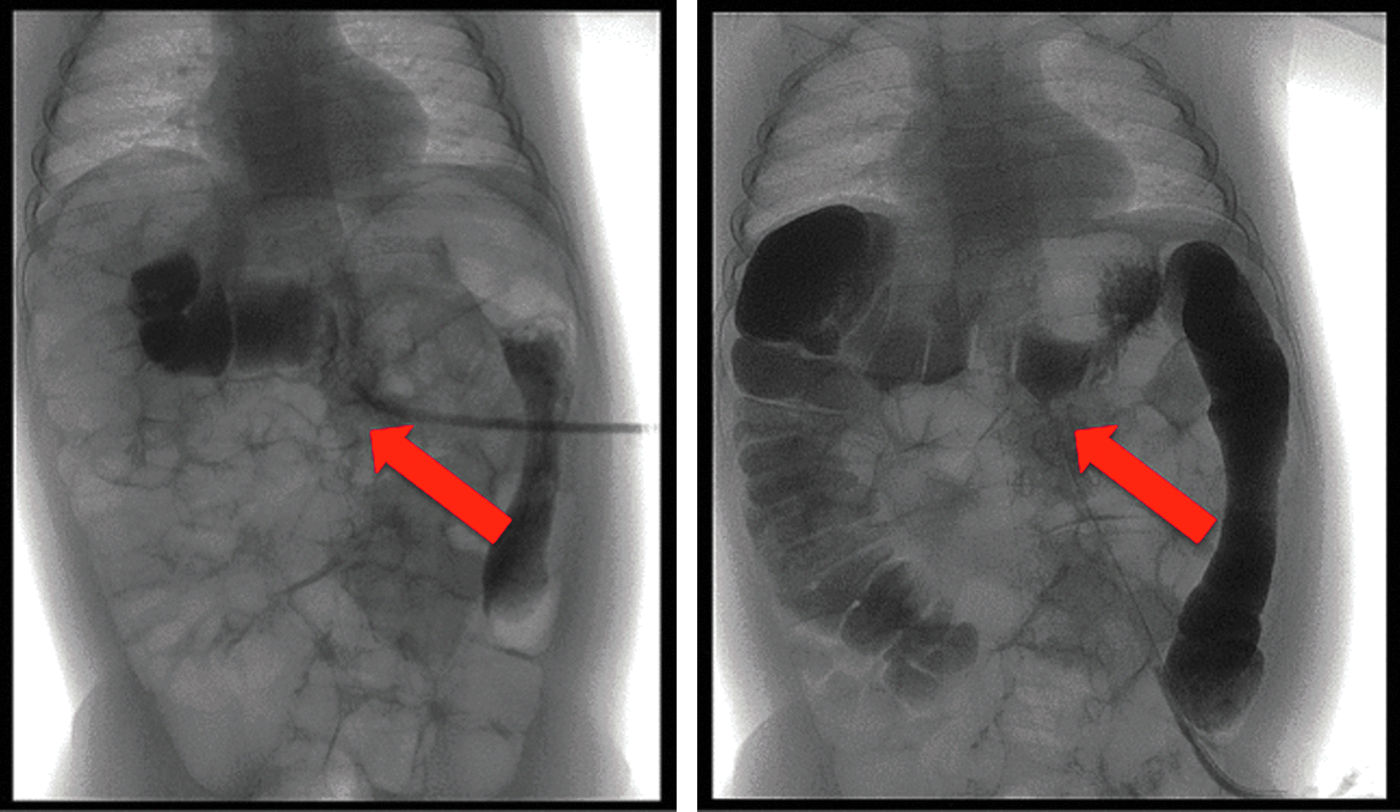
A contrastogram through the gastric tube revealed a direct injection of the contrast agent in the colon (red arrows), so a diagnosis of gastrocolocutaneous fistula was posed.
Case 2
The patient was a 10-year-old NI child, evaluated in May 2018. PEG was performed 3 months earlier, eliciting persistent diarrhea. The parents reported purulent secretions from the peristomal skin, yet normal growth was reported.
A contrastogram through the gastric tube evidenced the contrast agent immediately injected into the colon, confirming the presence of a gastrocolocutaneous fistula (Fig. 2). Effective laparoscopic repair, creating a new gastrostomy, was scheduled to be done over the following days.
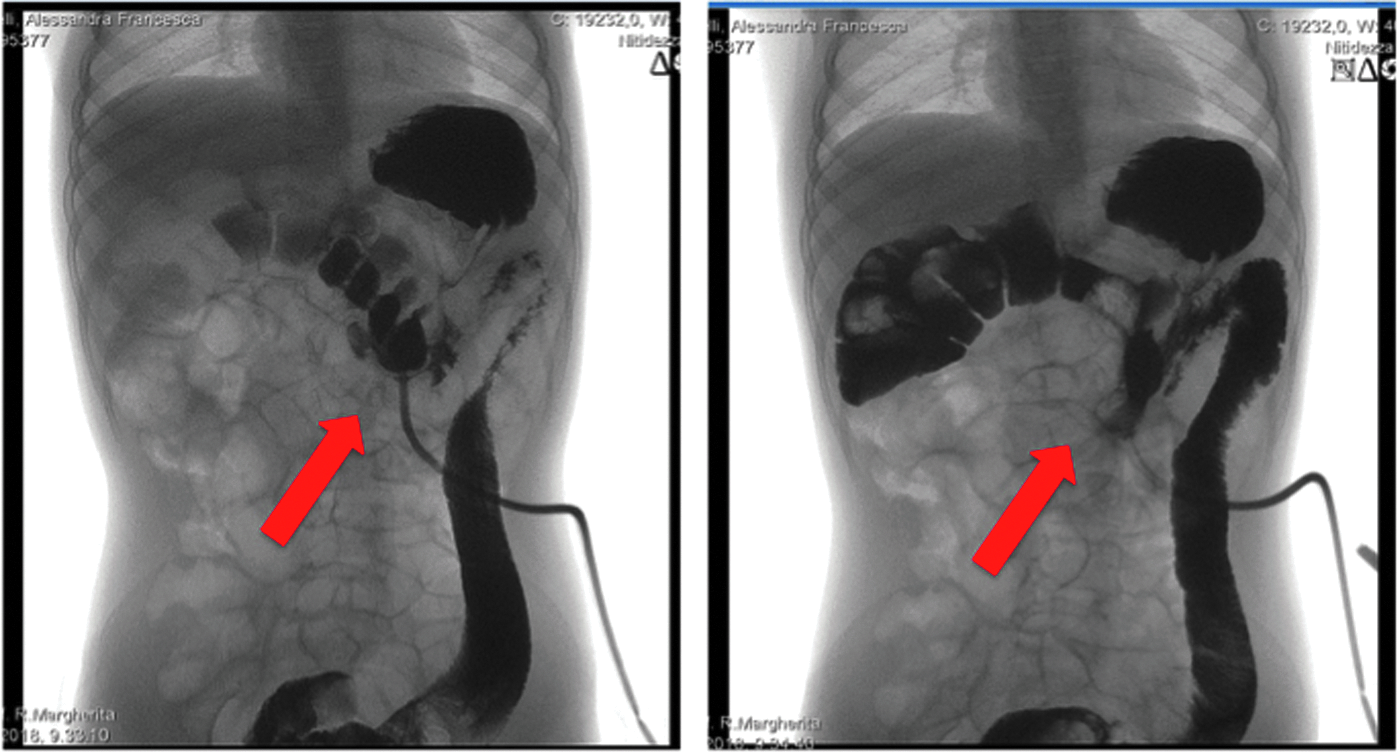
A contrastogram through the gastric tube evidenced the contrast agent that immediately injected the colon (red arrows) confirming the presence of a gastrocolocutaneous fistula.
Case 3
A 2-year-old child with severe nephropathy, weighing 9 kg, was a candidate for PEG, with inadequate caloric intake due to a chronic medical condition. PEG was performed in June 2018. The same day, about 12 hours postprocedure, the child manifested an acute abdomen with pneumoperitoneum. Abdominal X-ray and computed tomography scan were immediately obtained, revealing colonic and gastric transfixion in the gastric tube, with sudden onset of symptoms and separation of the transfixed colon from the abdominal wall (Fig. 3).
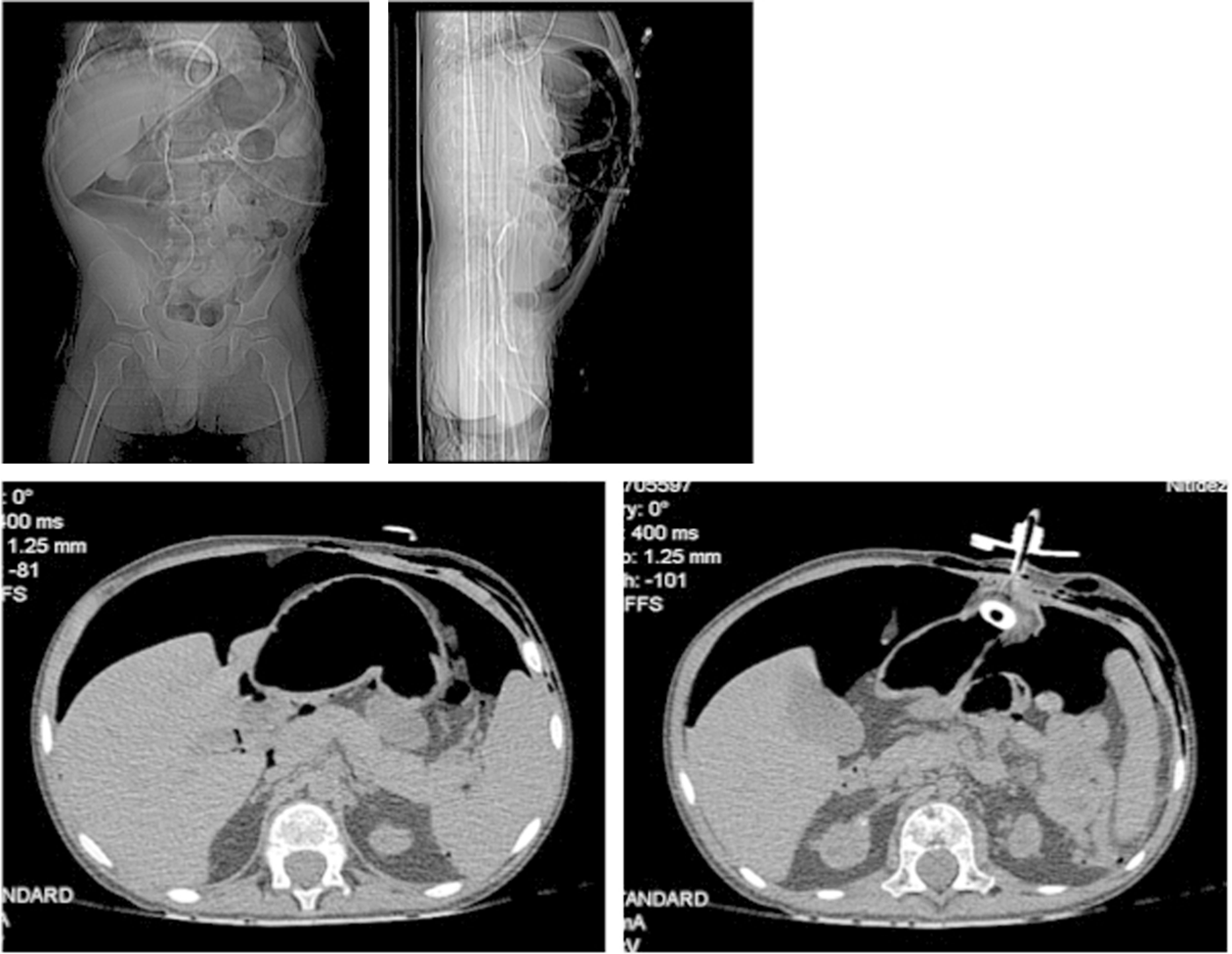
Abdominal X-ray and CT scan demonstrated colonic and gastric transfixion by the gastric tube. CT, computed tomography.
Emergency laparoscopy was initiated, and was almost immediately converted to open surgery due to the patient's critical condition. The colonic perforation was repaired, which was subsequently called a Stamm gastrostomy. The child had a normal recovery, with an uneventful follow-up.
Case 4
A 2-year-old syndromic child was hospitalized in October 2018 in our Infectious Disease Service for neutropenia. PEG was performed 6 months before for dysphagia. An episode of peristomal necrotizing fasciitis was also reported 3 months later, which resolved after several days of intravenous antibiotics.
While hospitalized for pneumonia, fecal secretions were noted from the peristomal skin. A contrastogram through the gastric tube was normal, with the contrast agent initially opacifying the stomach and then the entire ileum; due to persistent secretions through the stoma (confirmed by laboratory examination), a barium enema was conducted, identifying the colocutaneous fistula. Laparoscopic repair clarified fistula anatomy; due to anesthesiological problems from a laryngeal malformation, we converted to open surgery to close the colonic fistula (for a Stamm gastrostomy). The postoperative course was uneventful.
Results
Laparoscopic repair with a 3-trocar technique has been effective, when the patient's general condition allows for it. The procedure consists of three steps.
The first step is separation of the colonic fistula from the abdominal wall with Metzenbaum scissors (Fig. 4). The second step is closure of the residual colonic breach of the colocutaneous fistula, using internal separated absorbable stitches. The third step is gastrocolonic fistula isolation (usually located in the posterior gastric wall), and completed with dissection and closure, as well as the use of an endostapler (Figs. 5, 6 and 7).
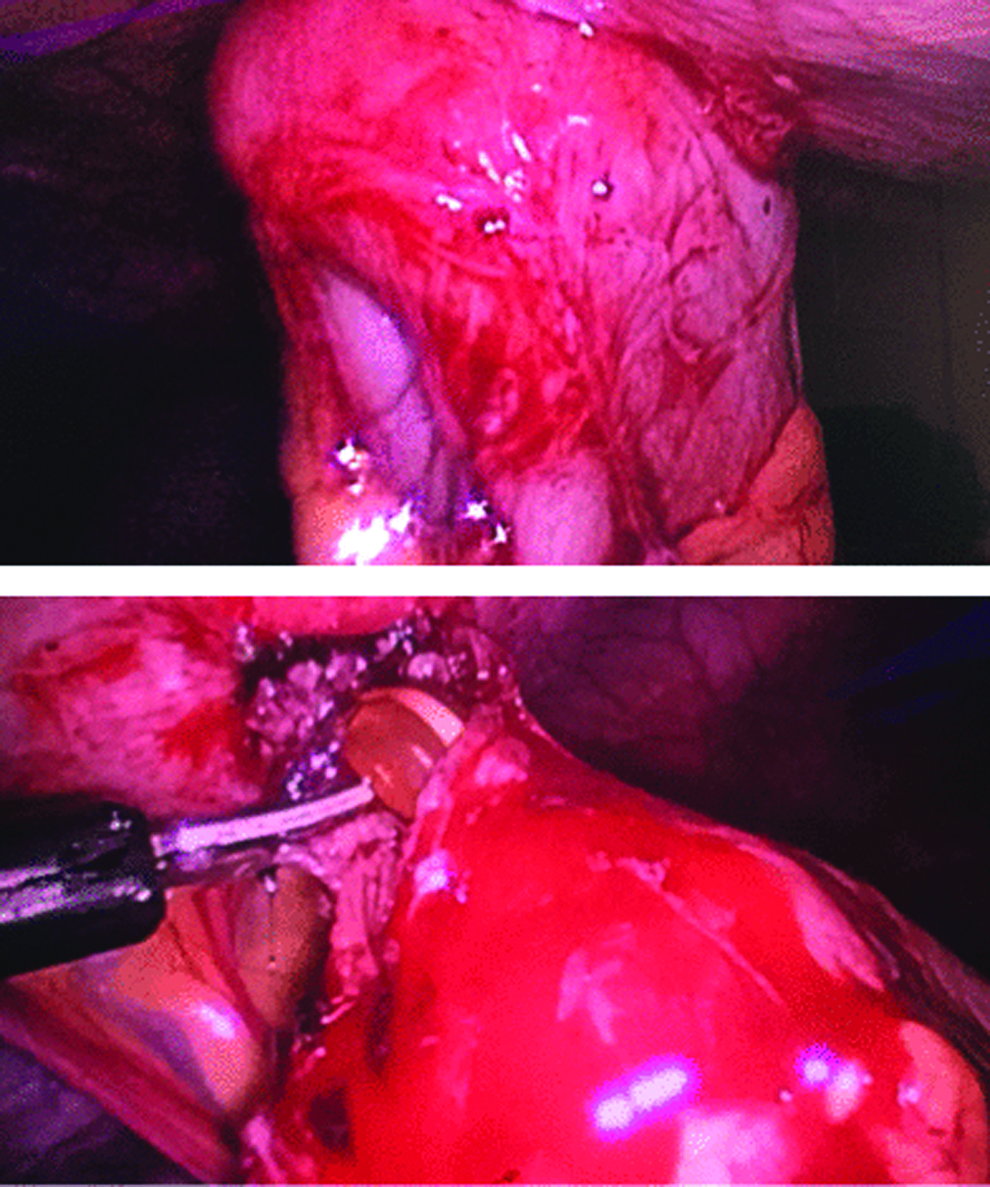
First step of the laparoscopic repair: the division of the colonic fistula from the abdominal wall with Metzenbaum scissors.
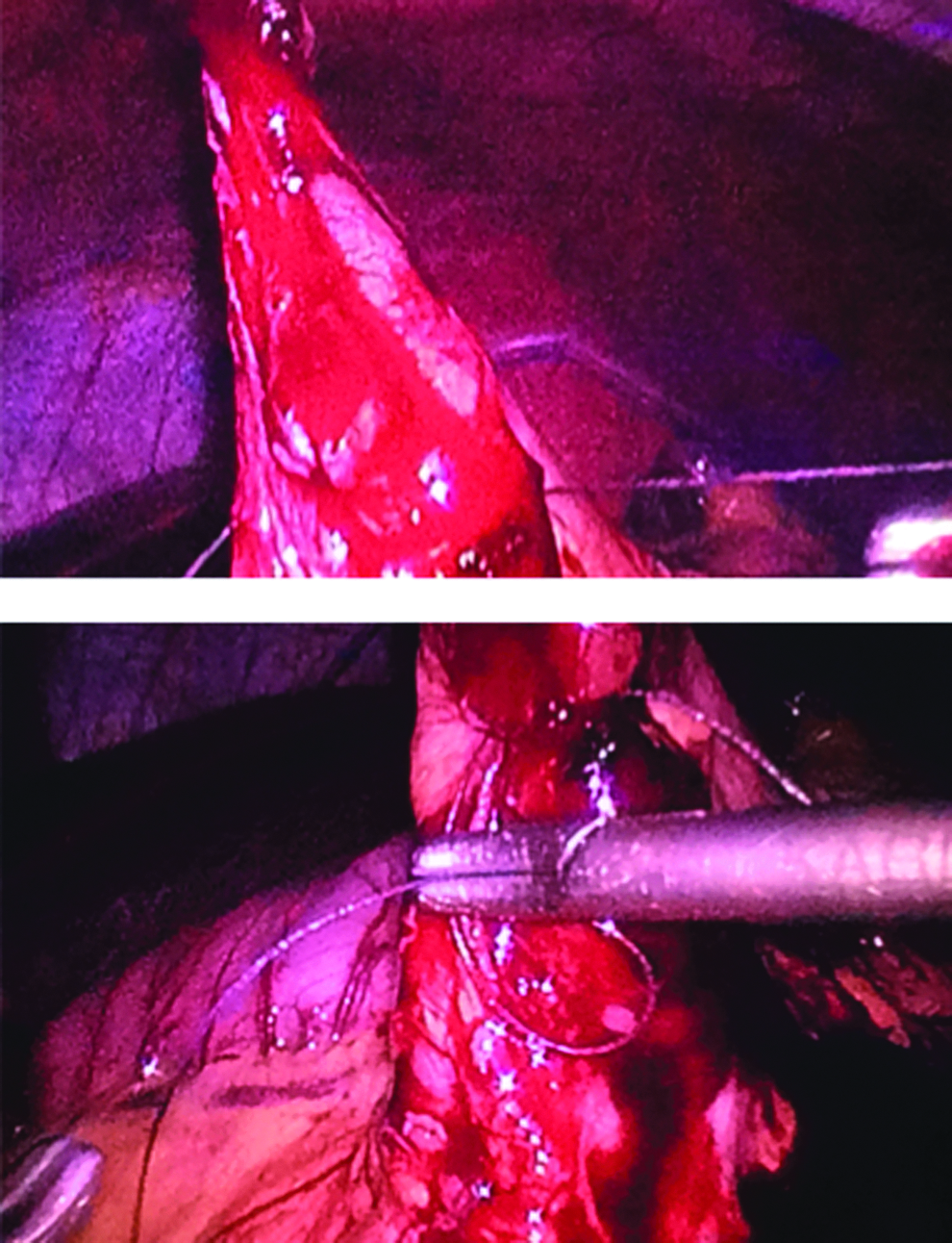
Second step: the closure of the residual colonic breach of the colocutaneous fistula, with internal separated reabsorbable stitches.

Third step: the gastrocolonic fistula isolation (usually the fistula was located in the posterior gastric wall). The green boxes show the exact position of the fistula (or channel) between the colon and the stomach.
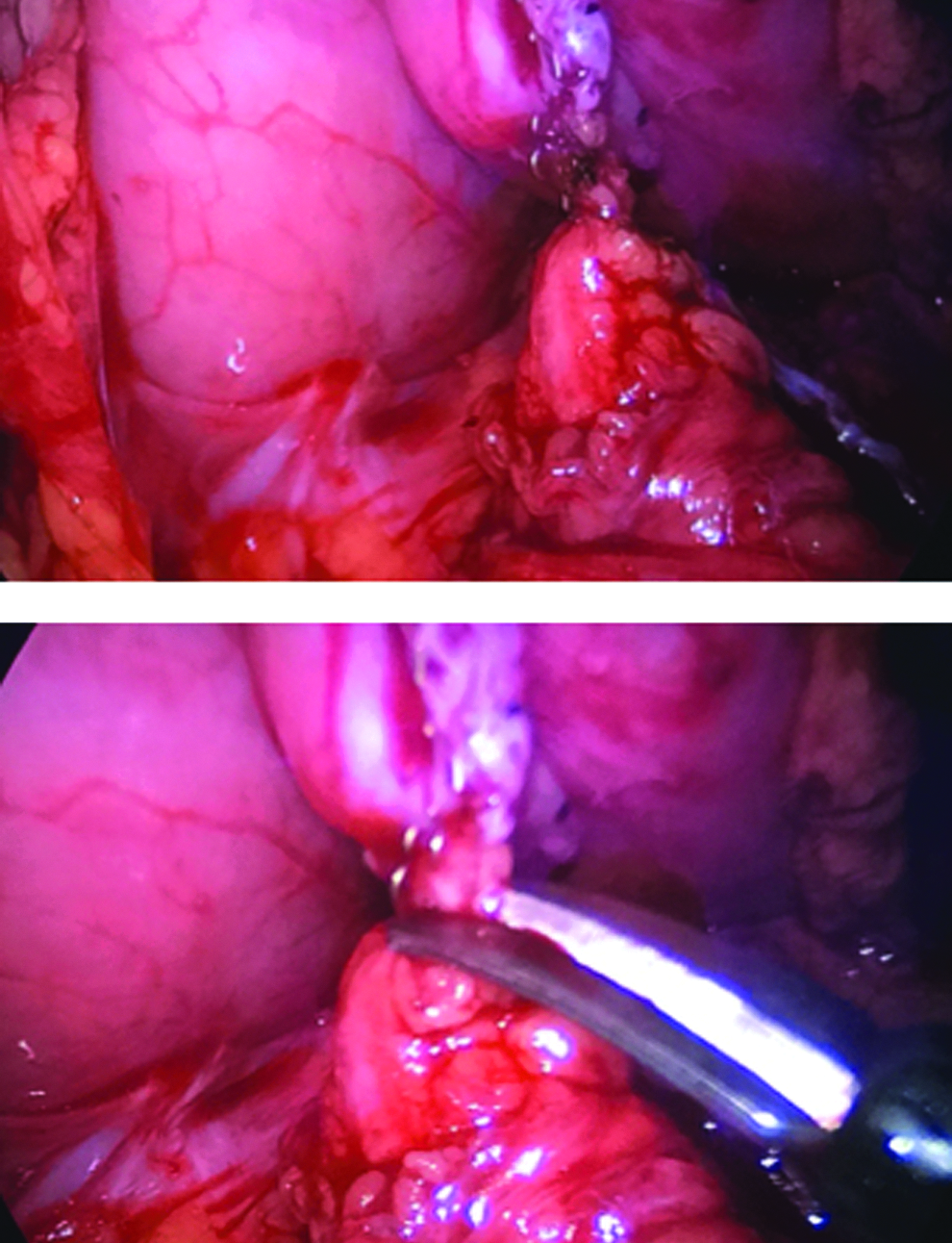
The gastrocolonic fistula division and closure with an endostapler.
After fistula repair, a new gastrostomy is placed, which can be performed endoscopically under laparoscopic control, or completely laparoscopically.
Discussion
The first PEG was reported by Gauderer et al. 2 in 1980; it has since become a common procedure that provides access for long-term enteral nutrition to patients, when oral feeding is not possible. Many children needing gastrostomy have comorbidities, so that every intervention constitutes a potential risk. Comorbidities are considered for planning future surgical interventions.
In these 4 patients, we faced unusual PEG placement complications, due to colon interposition during the blind gastric puncture. In our first two, a long gastrocolic fistula formed, with the bumper found in the colon, while in the third and fourth cases, the bumper was found in the stomach. Anatomical risk factors included extensive scoliosis and small abdominal cavities (in young children).
In a meta-analysis of gastrostomy placement in children in 2015, 1 Baker et al. observed that LAG was more favorable than PEG, with a calculated odds ratio of 0.29 and a 95% confidence interval of 0.17–0.51 (P = .0001). Forty-five cases were assessed to reduce major complications, accomplished by abandoning PEG.
In the recent literature, Petrosyan et al. 3 published a 6-year study comparing 150 PEG procedures with 143 laparoscopic gastrostomies in children under 5 years of age. They concluded that PEG tubes had a higher major complication rate than laparoscopic gastrostomy tubes, and despite a longer operative time, laparoscopic gastrostomy seemed to be the optimal procedure for children who required enteral access: moreover, it also eliminated unnecessary tube changes. Suksamanapun et al. 4 conducted a systematic review and meta-analysis, but offered no definitive conclusion as to which procedure was safer. Macchini et al. 5 reviewed 23 PEG procedures in infants during another 6-year study; they experienced 6 minor complications, concluding that PEG was safe and feasible in infants if performed by highly experienced physicians. A recent meta-analysis by Sandberg et al. 6 demonstrated a wide spectrum in the frequency of major complications between the two most common procedures, LAG and PEG, for gastrostomy tube placement in the pediatric population. The LAG technique is associated with fewer major complications, at a rate of 1%, compared with the major complication rate of 5.4% with the PEG technique.
Given these complications, the improved safety rate with LAG is a function of direct visualization of the peritoneal cavity for establishment of a gastrostomy. One can avoid blind puncture through the abdominal cavity, necessary for tube placement with PEG. Another technical advantage of direct visualization is the ability to choose a site for incision, which facilitates minimized tension.
To summarize, PEG in children has been associated with an increased risk of major complications, compared with a laparoscopic approach. The advantage of operative time appears to be outweighed by an increased safety profile for laparoscopic gastrostomy insertion.
Conclusions
In patients with anatomical deformities or previous surgeries, or when done in small children (under 10 kg), we suggest performing LAPEG, or a full laparoscopic gastrostomy to similarly avoid the risk of a major complication.
Compliance with Ethical Standards and Submission Statements
Ethics approval
All procedures performed in this study were in accordance with the ethical standards of the Institutional and National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants (children's parents) included in the study.
The article has been read and approved by all the authors; the requirements for authorship have been met and each author believes that the article represents honest work. The article has not been sent elsewhere during the submission to this Journal.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.