
Abstract
Introduction:
Surgical treatment for Hirschsprung disease (HD) has evolved from a staged repair to a primary operation but is still associated with significant complications. Extensive transanal dissection may overstretch the sphincter and cause partial tear; however, laparoscopic dissection can decrease rectal overstretching. Thus, this study aimed to evaluate the outcome of surgical management of HD and the efficacy of laparoscopic-assisted transanal endorectal pull-through in infants and children in our center.
Patients and Methods:
We reviewed the medical records of 74 patients who underwent surgical repair of HD from 2006 to 2019. However, we excluded 42 patients with HD (patients with stoma [n = 33] and total colonic aganglionosis [n = 9]). The remaining 32 patients were divided into two groups. Group A included patients who had transanal pull-through with laparoscopic assistance only to visualize the transition zone, take a biopsy, and check for twisting or bleeding. Group B included patients who had laparoscopic-assisted transanal pull-through with dissection of the rectum. All patients had Soave repair with an approximate cuff length of 5 cm.
Results:
Group A included 18 patients, whereas group B included 14 patients. Demographic data were comparable between the two groups with no significant difference in age or gender (P = .12 and .67, respectively). Patients in group A had longer operative time (210 ± 20.75 minutes versus 178 ± 18.92 minutes; P < .001) and hospital stay (6 ± 1.33 days versus 5 ± 1.24 days; P = .033). No significant difference was observed in postoperative complications between both groups (anastomotic site stricture, P = .295; persistent soiling, P = .238).
Conclusion:
Laparoscopic rectal dissection for managing HD is associated with less operative time and hospital stay. In addition, all procedures required for the repair can be safely performed using laparoscopy.
Introduction
Hirschsprung disease (HD) is a common neonatal developmental disorder characterized by the absence of ganglionic cells in the distal intestine that results in the loss of peristalsis in the affected segment and functional intestinal obstruction. 1 Neonates with HD usually present with delayed passage of meconium or constipation later in life. HD is mainly diagnosed via radiology, anorectal manometry, and rectal wall biopsy. 2
In 1948, Swenson and Bill first described the basic principles of surgical repair of HD. 3 Since then, the surgical management of HD has progressed from a staged repair comprising two or three procedures to a primary operation. 4 In the single-stage primary correction, a laparotomy approach is used to mobilize the colon, followed by an endorectal pull-through.
Currently, three main endorectal pull-through techniques are commonly used: the Swenson, Soave, and Duhamel procedures. 5 Two decades ago, the laparoscopic approach was developed with its role limited to the identification and biopsy of the transition zone and mobilization of the rectum and sigmoid colon before the endorectal pull-through. 6 The complete transanal endorectal pull-through was later introduced by De La Torre and Langer.7,8 Both techniques had comparable results to the open procedures. 9
Laparoscopic mobilization of the colon before the pull-through improved the outcome of transanal endorectal pull-through for classic HD by avoiding excess stretching of the sphincters caused by transanal rectal dissection. Given this background, the aims of our research were to study the results of surgical management of HD and to evaluate the efficacy of laparoscopic-assisted transanal endorectal pull-through in infants and children in our center.
Patients and Methods
Patients and study settings
The present research is a retrospective cohort study approved by the Institutional Biomedical Ethical Committee, Faculty of Medicine, Um Al Qura University (Institutional Review Number HAP0-02-K-012-2019-05-313). Seventy-four patients diagnosed with HD underwent surgical repair at King Faisal Specialist Hospital and Research Center and Bakash Hospital, Jeddah, Saudi Arabia, between 2006 and 2019. Of them, 42 patients who had a stoma (n = 33) and total colonic aganglionosis (n = 9) were excluded from the study. The remaining 32 patients (28 boys and 4 girls) who underwent the transanal pull-through procedure with or without laparoscopic assistance were included in the analysis. Figure 1 shows the study flowchart.
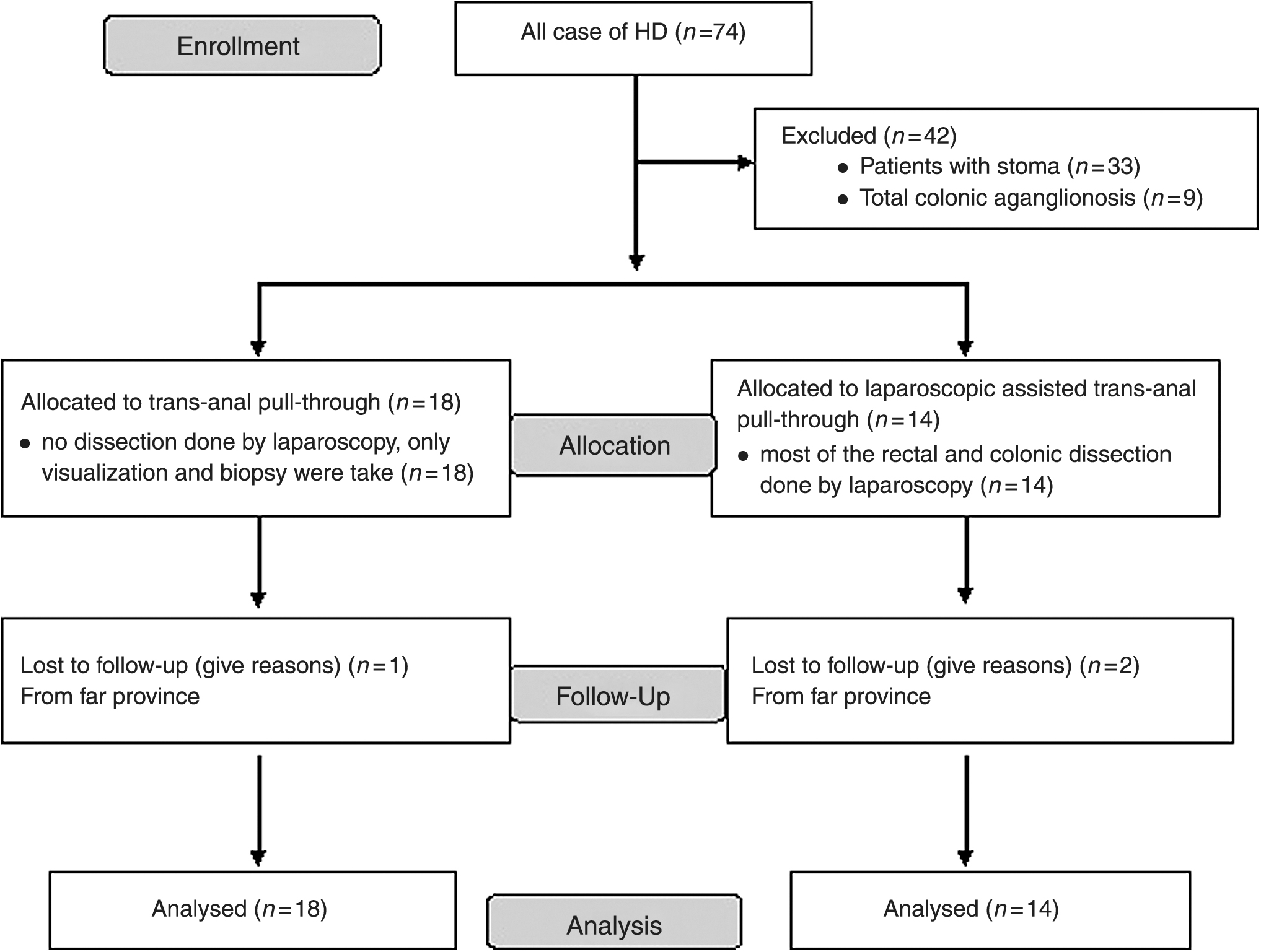
Study flowchart.
Surgical technique and grouping
All the initial cases underwent transanal pull-through with laparoscopic assistance only to visualize the transition zone, take a biopsy, and check for twisting or bleeding at the end of the procedure (group A: n = 18). From February 2014 onward, all cases of HD underwent laparoscopic-assisted transanal pull-through with dissection of the rectum (group B: n = 14).
In all the patients, HD was diagnosed based on clinical symptoms, barium enema, and rectal biopsy. All included children presented with abdominal distension or progressively worsening intractable constipation. Most of the patients had a well-defined transitional zone in the mid-sigmoid colon. The diagnosis was confirmed using intraoperative frozen biopsy. Laparoscopic assistance was used in all patients with a variable extent, and the length of resected bowel was determined intraoperatively (Figs. 2 and 3). All patients had Soave repair with an approximate cuff length of 5 cm in earlier cases and 2 cm with posterior split.
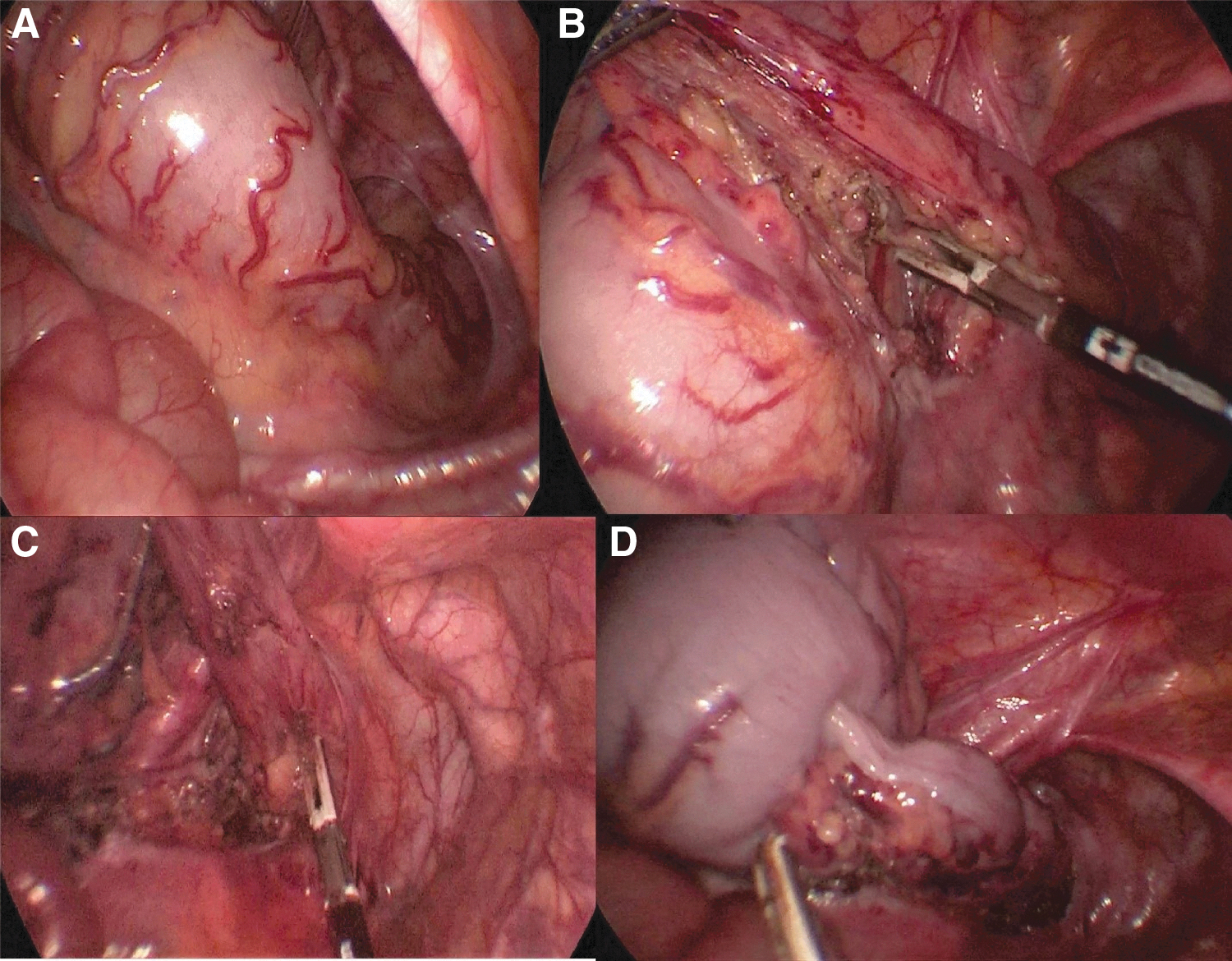
Laparoscopic mobilization of the sigmoid and rectum using LigaSure™ device.
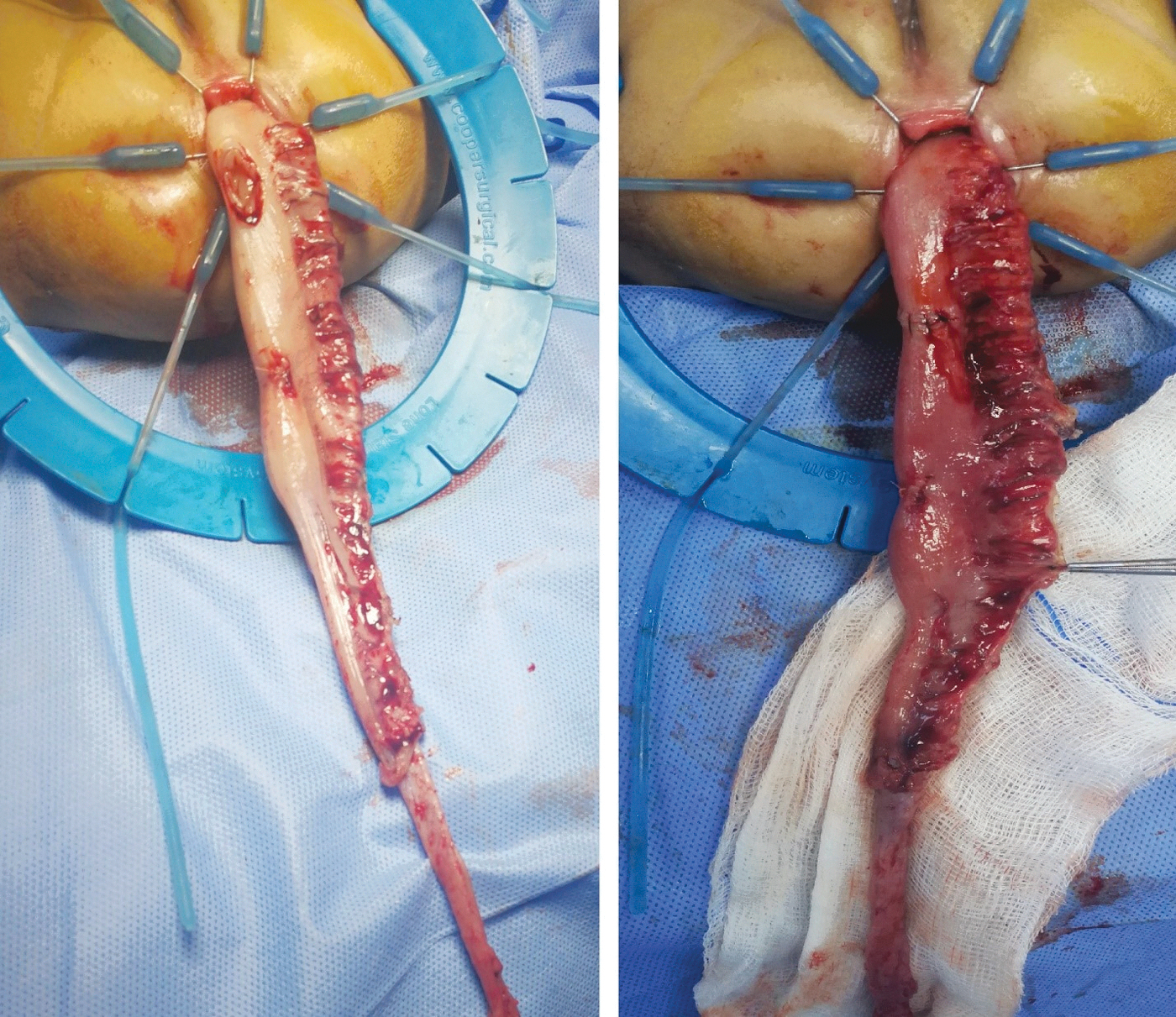
Transanal pull-through of the rectum and colon (80 cm).
Preoperative collected data included gender and age at presentation and time of surgery. Study endpoints were operative time, hospital stay, and postoperative complications.
Statistical analysis
We presented the continuous variables as mean ± standard deviation or median and range, and t-test or Mann–Whitney test was used for comparisons. Categorical variables were presented as number and percentage and compared with the Fisher's exact test. All analyses were performed using Stata 14.2 (StataCorp., College Town, TX). A P value less than .05 was considered significant.
Results
A total of 32 patients with HD (male to female ratio of 4.3:1) were included in the analysis. The patients were divided into two groups according to the surgical technique. The median age in group A was 3 months (range, 0–39 months) versus 5 months (range, 0–45 months) in group B. In addition, no difference was observed in age either at presentation or at the time of surgery between groups (P = .12 and .07, respectively) (Table 1).
Preoperative and Operative Data
Continuous variables are presented as mean ± standard deviation.
Patients in group A had longer operative time (210 ± 20.75 minutes versus 178 ± 18.92 minutes; P < .001) and hospital stay (6 ± 1.33 days versus 5 ± 1.24 days; P = .033).
In our series, only one case of a child had anal incontinence. At the age of 2 years, the child underwent dissection of the dilated colon for long-segment disease that overstretched the anal sphincter and caused the tear as observed latter on the magnetic resonance imaging (MRI). None of the patients in both groups had postoperative bleeding. Moreover, no statistically significant difference was found in the reported complications between groups (wound infection, stricture at the site of the anastomosis, skin excoriation, and soiling) (Table 2).
Comparison of Postoperative Complications Between Groups
Categorical variable as number and percentage.
Discussion
Several surgical techniques have been described for the management of HD. 10 Surgical management involves resecting the aganglionic segment and pulling the ganglionated portion through to a point just above the dentate line. Several pull-through procedures have been described for the management of HD with varying functional outcomes, but there is a lack of consensus regarding the best pull-through technique in terms of outcomes. In this study, we evaluated different techniques for the management of HD and their outcomes in 32 patients. Most of our patients were males (87.5%), and this agrees with previous reports that the disease is predominant in males. 11
The transrectal pull-through technique prevents injury to the pelvic nerves by remaining within the muscular cuff of the aganglionic segment. In addition, it is associated with a lower incidence of constipation, sexual dysfunction, and micturition disturbances. 12 These advantages are evident in infants, but older children with dilated bowel may have sphincter tear and fecal incontinence. The complete transanal pull-through, which is carried out without laparoscopy or laparotomy, avoids peritoneal dissection completely. However, this applies only in classical rectosigmoid disease; additionally, it involves major stretching of the external sphincter to facilitate lengthy submucosal dissection.
Laparoscopy can be used variably in these cases. It can be used to conduct a biopsy and check for orientation and bleeding at the end of the procedure. It can also be used for the dissection of the sigmoid colon and upper rectum to the level just below the peritoneal reflection and minimization of the transanal dissection to the lower rectum. This decreases the operative time and the extent of stretching of the sphincter.
The advantages of both approaches (transrectal and laparoscopic) were combined in group B patients. We performed the major dissection of the rectum and sigmoid through laparoscopy with magnification, and the transanal dissection was used only for the distal portion. This made HD management feasible, shortened the operative time significantly, and reduced the extent to which the sphincter was stretched. Meanwhile, in group A, all rectal and colon dissections were performed through the transanal approach without any laparoscopy. This prolonged the operative time and was technically demanding and associated with more stretching of the sphincters (Fig. 4).

Postoperative MRI for a patient in group A showing thinning of the anal sphincter (red arrow) on the right side, the white fatty tissue replaced the muscle tissue. MRI, magnetic resonance imaging.
Georgeson et al. reported the initial laparoscopic-assisted endorectal colon pull-through experience in 12 children with acceptable results. 13 Moreover, they modified the technique and described technical points in their publication in 2008. 14 In recent years, minimal access techniques have been introduced for dissection of the aganglionic part of the bowel. 15 Some surgeons advocate removing not only the aganglionic and transitional segments but also all the dilated segment. 7
The feasibility of laparoscopic-assisted repair has been evaluated before.16,17 Laparoscopic approaches for the management of HD offer several benefits. They precisely determine the level of the transition zone before perineal dissection, visualize the pulled-through segment for no bleeding or twisting, and mobilize the splenic flexure in the case of a more proximal transition zone. 18 Retained transition zone after pull-through is the primary cause of anastomotic site stricture post repair. This complication can be prevented by proper identification and resection. 19 In a meta-analysis comparing laparoscopic versus open approach for the management of HD, the laparoscopic approach had shorter operative time and lesser blood loss. 20 No difference has been observed in the incidences of enterocolitis, constipation, and incontinence between patients who had total transanal endorectal pull-through versus laparoscopic-assisted approach. 21 Three- and two-dimensional laparoscopies have been compared for the management of HD, and it has been reported that the three-dimensional approach had significantly reduced operative time. However, no difference was observed regarding other outcomes. 22
Finally, further understanding of the pathophysiology and bowl transition into abnormal segments beyond the simple description of the presence or absence of ganglion cells is essential for future refinements of surgical techniques.
Study limitations
There are several limitations to the study, including its retrospective nature with its inherited biases. The study is a single-center experience, and generalization to all centers may not be applicable. The patients were not randomly assigned to both groups, and there could be confounders that affected the outcomes and not included in the analysis. The study did not evaluate the long-term outcome of both approaches and the quality of life; hence, a longer follow-up study is recommended.
Conclusion
Laparoscopic-assisted transanal endorectal pull-through can be performed in a single stage for the management of HD with less morbidity and postoperative stay. In addition, our findings suggest that all procedures required for surgical management of HD can be safely performed using laparoscopic rectal dissection.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.