
Abstract
Aim:
To report the surgical technique and early outcomes of robot-assisted ureterocalicostomy (RAUC) with near-infrared fluorescence (NIRF) in the management of secondary pelvi-ureteric junction obstruction (PUJO) in adults.
Materials and Methods:
The data of 6 patients who underwent RAUC using Da Vinci Xi system with NIRF technology between November 2017 and April 2019 were retrospectively reviewed. Indication was secondary PUJO due to previous failed pyeloplasty. The outcome variables evaluated include operative time (total and console), length of hospital stay, blood loss, and complications. Success was defined as the absence of pain and radionuclide scan demonstrating nonobstructive drainage and improvement/stabilization of split function of the renal moiety.
Results:
The mean (range) patient age was 33.7 (18–41) years. Total mean (range) operating time was 178 (140–240) minutes and mean console time was 135 minutes. Estimated mean blood loss was 115 (50–200) mL and average hospital stay was 6.1 (5–8) days. There were no conversions to open or laparoscopic surgery. Clavien–Dindo complications occurred in 2 patients. (Grade I-1 and Grade II-1). After a median (range) follow-up of 15 (6–22) months, all 6 patients had successful clinical and radiological outcomes.
Conclusion:
RAUC is a safe and feasible technique with acceptable outcomes in the setting of secondary PUJO. The utility of NIRF in determining vascularity of the ureter seems to be promising in this setting. Multi-institutional prospective studies with large patient cohort are necessary to validate the role of robotic platform in ureterocalicostomy in the reoperative settings.
Introduction
The management option for secondary pelvi-ureteric junction obstruction (PUJO) includes endopyelotomy or complex surgical reconstruction (redo pyeloplasty, ureterocalicostomy, or rarely ileal ureter replacement). However, endopyelotomy is a contraindication in patients with ureteric stricture segment greater than 2 cm. 1 Hence, these patients need to be managed by the above-mentioned complex surgical reconstruction by open, laparoscopy, or robot-assisted laparoscopic approach. Although majority of secondary PUJO can be surgically treated by redo pyeloplasty, certain anatomic situations require the adaptation of ureterocalicostomy as a salvage option. This includes primary PUJO with an intrarenal pelvis; small renal pelvis rendered by previous pyeloplasty, complex anatomy, and obliterated pelvi-ureteric junction (PUJ)/ureter after prior surgery.2,3 In addition, the success rates of endopyelotomy are much inferior to pyeloplasty in the primary setting. This has resulted in a significant increase in the number of patients requiring ureterocalicostomy in the modern era. 4
Owing to the technical complexity, majority of the series have reported open approach for ureterocalicostomy. 5 Gill et al. first described the laparoscopic approach for ureterocalicostomy, paving the way for the adaptation of minimal access surgery in this clinical scenario. 6 However, only few centers were able to adapt the technique of laparoscopic ureterocalicostomy due to the steep learning curve. Korets et al. reported the first robotic-assisted laparoscopic ureterocalicostomy (RAUC) in 2007. 7 The adoption of robotic technology has facilitated meticulous dissection and suturing, which is very essential for the execution of this surgical procedure. The critical part of this surgery is in ensuring the vascularity of the proximal ureteral segment before proceeding to anastomosis with the lower polar calix to avoid ischemia and subsequent failure. The robotic Xi platform with the Firefly® technology with intraoperative indigo carmine (ICG)-fluorescence imaging helps in this vital step. 8
The objective of the present study is to report the technique and early outcomes of robotic ureterocalicostomy with adoption of near-infrared fluorescence (NIRF) with Firefly technology.
Materials and Methods
The present study was carried out by retrospectively reviewing the hospital records of patients who underwent robotic ureterocalicostomy at Jawaharlal Institute of Medical Education and Research from July 2017 to April 2019 after obtaining approval from the Institute Ethics Committee. Six patients (males: 2, females: 4) were eligible to be included in the study. The etiology of secondary PUJO was a previously failed pyeloplasty. The chief presenting complaint was flank pain. In addition, 1 patient presented with fever and pyonephrosis. On presentation, ultrasound-guided percutaneous nephrostomy was performed on all the patients to relieve the pain as well as to relieve the obstruction. The surgical reconstruction was performed on the right side in 4 and left side in 2 patients. All the patients underwent diuretic renography to assess the baseline renal function and repeat scan for 3 to assess the drainage pattern as well as to document the recovery of the affected kidney function. Subsequently, the anatomy and the stricture length were assessed based on antegrade and retrograde pyelography and/or computerized tomography. The length of the strictured segment ranged from 1 to 3 cm in our patients. The patient's characteristics at presentation are summarized in Table 1. The indication for surgery in this study cohort was PUJO secondary to failed pyeloplasty associated with intrarenal pelvis and long-segment ureteric stricture precluding a redo pyeloplasty.
Clinical Characteristics and Demographics of the Patients
PUJO, pelvi-ureteric junction obstruction.
Surgical technique
The patients underwent robotic ureterocalicostomy under general anesthesia. The authors adopted the surgical technique described by Chhabra et al., 9 with modifications for the Da Vinci Xi system. Initially, a 5F open-ended ureteric catheter was placed into the ureter just below the PUJ stricture under fluoroscopic guidance and secured to a 14F Foley catheter. Subsequently, the patient was placed in the lateral decubitus position and strapped to the operating table. The pneumoperitoneum was created using the Veress needle. Three robotic 7 mm ports were placed along the lateral border of the rectus muscle in a straight line, as there is no need for a triangulation with the Da Vinci Xi System. An assistant port (10 mm) was placed in between the subcostal and the camera port. The nephrostomy tube was clamped before the start of the dissection.
Using the 30° telescope, the white line of Toldt was incised. The duodenum was kocherized when operating on the right side. The ureter was identified at the common iliac artery bifurcation and traced up to the lower pole of the kidney. The preplaced ureteric catheter facilitated this step. All efforts were taken to preserve the periureteric vasculature during this dissection. Then, the lower pole of the kidney was cleared off the perinephric fat all round. The ureter was disconnected at the stricture segment. At this point, intraoperative near infrared (Firefly) technology using ICG was used to assess the vascularity of the proximal segment of the ureter. About 2.5 mL of ICG, a fluorescent dye was injected intravenously and the Firefly was activated. A well-vascularized ureteric end will demonstrate a green glow. In ischemic condition, the ureteric segment will remain dark (Fig. 1). This technology is of immense help to the surgeon in fashioning the ureter before anastomosis thereby avoiding nonviable segment and eliminating the risk of restricture. Then, the lower pole of the kidney at the most dependent area was amputated to expose the calix (Fig. 2). The ureter was spatulated on the lateral aspect, and ureterocaliceal anastomosis was performed using 4-0 Vicryl sutures in a standard manner to ensure a dependent, tension-free anastomosis after placing a 5F double J stent antegradely (Fig. 3). The anastomosis was then wrapped with perinephric fat to facilitate anastomotic healing. A drain was placed at the end of the surgery.
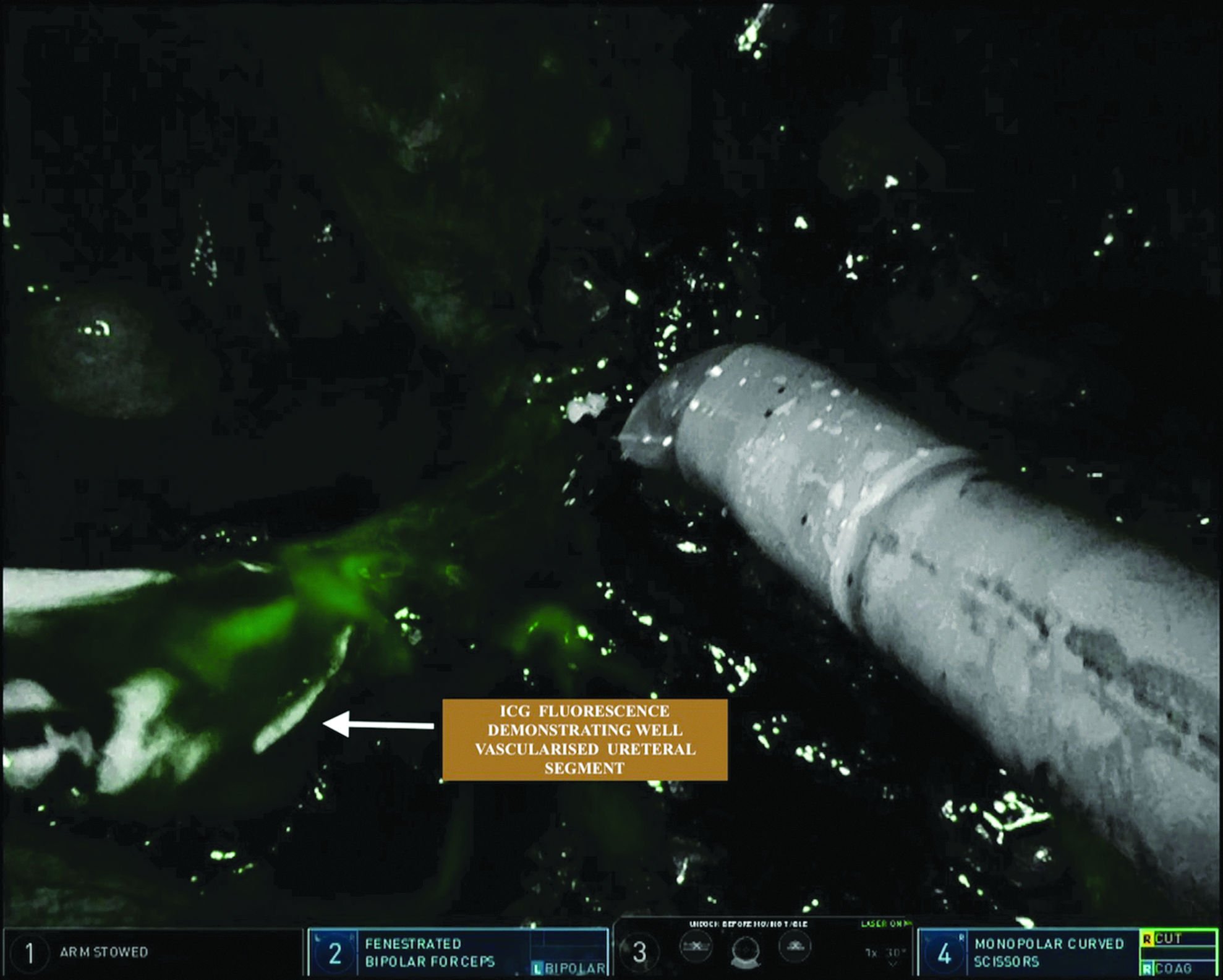
Intraoperative NIRF demonstrating the green fluorescence of the resected ureteric edge implying vascularized segment. NIRF, near-infrared fluorescence.
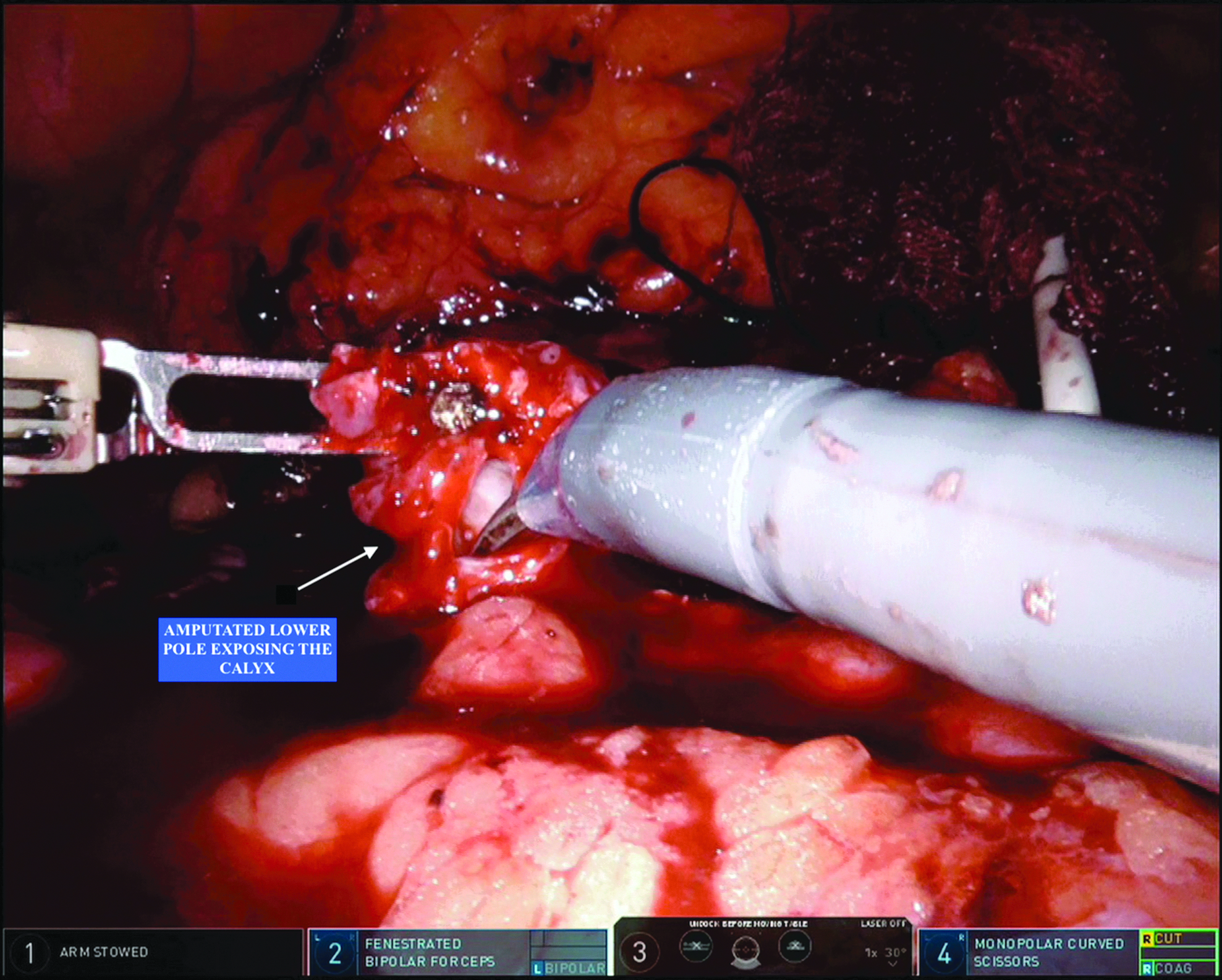
Intraoperative photograph showing the amputated lower pole of kidney with exposed calix.

Completed ureterocaliceal anastomosis.
The Foley catheter was removed on the second postoperative day. The percutaneous nephrostomy was removed on the third postoperative day and the drain output was monitored for 1 day. Subsequently the drain was removed and the patient was discharged. The stent was then removed after 4 weeks on outpatient basis. All the patients underwent radionuclide scan at 3 months postoperative period to assess the drainage pattern as well as the split renal function.
Success was defined as the absence of pain, radionuclide scan demonstrating nonobstructive drainage and improvement/stabilization of split function of the renal moiety.
Results
The mean (range) patients age was 33.7 (18–41) years. There were 2 males and 4 females in our study group. The robotic ureterocalicostomy was performed on the right side in 2 and left side in 4 patients. Total mean (range) operating time was 178 (140–240) minutes, and mean console time was 135 minutes. Estimated mean blood loss was 115 (50–200) mL and average hospital stay was 6.1 (5–8) days. The mean (range) age of the 6 patients was 27.1 (19–35) years. There was no blood transfusion in our series and no conversion to open or laparoscopic surgery. Two patients developed postoperative complications. Clavien–Dindo Grade I (fever) was managed conservatively, and Grade II (urinary tract infection) required antibiotic administration. At a median (range) follow-up of 15 (6–22) months, in all the 6 patients, the outcomes of the surgery were deemed to be successful based on both the clinical and radiological criteria. However, the patient who presented preoperatively with pyonephrosis demonstrated persistent severe hydronephrosis at 6 months of follow-up, although diuretic radionuclide scans showed delayed tracer clearance. This patient is under close follow-up to detect worsening renal function.
Discussion
Neuwirt et al. in 1947 first described the surgical technique of ureterocalicostomy for complicated PUJO. 10 Hawthorne later modified this technique. 3 Subsequently, Ross et al. documented that the indications for ureterocalicostomy were scarring of the pelvic-ureteric junction due to previous pyelolithotomy and previously failed pyeloplasty in a small series of patients. 11 However, Matlaga et al. observed that the majority of patients in their series required ureterocalicostomy as a result of failed endourological approach or due to a complication of endourological approach. 5 Chhabra et al. also reported similar indications in their series of 5 patients who underwent robotic ureterocalicostomy. 12 This is in contrast to our series where the indication was previously failed pyeloplasty (open or laparoscopic approach).
In conditions leading to obstruction to flow of urine from the upper tract such as failed pyeloplasty, secondary PUJO due to previous endourological interventions and congenital PUJO with intrarenal pelvis, the risk of upper tract deterioration is a clinical concern. In these circumstances, a definitive surgical treatment is imperative to mitigate the risk. The above-mentioned causes are the indications for ureterocalicostomy. Endopyelotomy can be an option in this setting, but the outcomes of definitive techniques such as redo pyeloplasty or ureterocalicostomy are superior in terms of providing a durable and long-term nonobstructed drainage. 13 There are only a few case series and isolated case reports on the use of ureterocalicostomy in literature. Majority of the surgeons preferred open approach due to the anatomical complexity of this technique.5,11,14,15 The reported outcomes of ureterocalicostomy are variable among different series.5,11,16,17 The success rates are higher in children 18 and in primary PUJO.16,17 Moreover, the success rate decreases as the duration of follow-up increases.
The key surgical steps include complete amputation of the lower pole of the kidney, preservation of all periureteral tissue and the blood supply, creation of a widely spatulated, tension-free, mucosa-to-mucosa anastomosis, and internal stenting. 5 Some authors recommend covering the lower pole capsule over the renal parenchyma to buttress the anastomosis. 17 The most frequent complication after ureterocalicostomy is recurrent obstruction and anastomotic stricture. Making all attempts to preserve the vascularity of the ureter during dissection in the already scarred region can obviate this complication.
Subsequent to the demonstration of the feasibility of laparoscopic ureterocalicostomy in animal models, Gill et al. reported the first clinical series of laparoscopic ureterocalicostomy in 2 patients. 6 The first patient had a successful outcome, whereas in the second patient although there was radiologic improvement, the patient required nephrectomy due to persistent pain. Arap et al. reported the largest series of laparoscopic ureterocalicostomy, in which 6 patients underwent the procedure for complicated PUJO. 19 The etiology included failed pyeloplasty, anatomical abnormalities, and upper ureteric stricture. The median operative time was 215 (180–270) minutes. There was no conversion to open technique and no major intraoperative complications. At a median follow-up of 30 months, all the 6 patients demonstrated clinical and radiological improvements translating into a 100% success rate.
The first reported case of RAUC was described by Korets et al. who used a hybrid technique by utilizing conventional laparoscopy for the initial dissection and robotic platform for the anastomosis. 7 Following this, Schimpf and Wagner in 2009 successfully completed ureterocalicostomy using the robotic platform in a female patient. 20 Casale et al. reported the largest series of RAUC in 9 pediatric patients with successful outcomes in all the children. 21 Recently, Jacobson et al. also reported their outcomes of RAUC in 5 children with favorable results confirming the durability of the robotic approach. 22 Chhabra et al. report their experience of RAUC in 6 renal units in 5 adults. 12 The indications include failed pyeloplasty (1); postpyelolithotomy PUJ stricture (4), and postpercutaneous nephrolithotomy (1). The mean operating time was 172 minutes and estimated mean blood loss was 100 mL. There were no open or laparoscopic conversions in their series. The median (range) length of hospital stay was 6.5 (5–8) days. Out of the 6 renal units, 5 had successful outcomes at a median follow-up of 11 months. One of the patients is on regular Double J stent change due to impaired renal drainage. Narain et al. reported their experience of RAUC in 5 adults of secondary PUJO with successful outcomes in all of them without major intraoperative complications or open conversion. 23
Our series of 6 patients with RAUC is one of the largest reported in literature. Five of the 6 patients in our series had successful clinical and radiologic outcomes at a median (range) follow-up of 9 (7–12 months) months. One of the patients had persistent severe hydronephrosis at 6 months of follow-up, although the diuretic renography demonstrated delayed clearance. This patient is under close observation as the follow-up duration is only 6 months. The mean operating time, blood loss, and outcomes were comparable to that of Chhabra et al. 12 and Narain et al. 23 The outcomes of few large series of RAUC reported in literature are summarized in Table 2.
Details of Few Large Series of Robot-Assisted Ureterocalicostomy Reported in Literature Comparing with the Present Series
Conventionally, the viability of the ureter was determined intraoperatively primarily by the presence of bleeding at the transected surface of the ureter and the size of the ureteral lumen. The Da Vinci Xi system with intraoperative NIRF technology using intravenous ICG provides an adjunct technique in determining the vascularity of the proximal end of the ureter. The vitalized end appears as green, while blackish appearance indicates a devitalized segment. The authors believe that this technology aids the surgeon in real-time to demarcate vascularized from devascularized tissue in an efficacious and reproducible manner to accomplish this crucial step of ureterocalicostomy. This is perhaps one of the largest series in literature describing the use of intraoperative ICG fluorescence in RAUC. Furthermore, Lee et al. described a novel technique of intraureteral administration of ICG through a ureteric catheter to determine the level of stricture to aid in appropriate resection of the strictured segment. 24
The use of the robotic platform with its inherent advantages helps in fine dissection and suturing, thereby facilitating this complex reconstructive surgery, similar to open surgery, at the same time conferring the advantages of minimal access technique to the patients. The outcomes of the present series compares favorably with that of Chhabra et al. 12 and Narain et al. 23 In addition, this study adds the utility of ICG fluorescence on the Da Vinci Xi platform in RAUC.
The limitations of the present study include few patients, retrospective study design, single-center series, and shorter follow-up. There is a need for a multi-institutional prospective study involving a larger cohort of patients with longer follow-up to validate our results.
Conclusion
The indications for ureterocalicostomy in literature are showing increasing application for endourological failures in contrast to our series, in which failed pyeloplasty was the indication. Robot-assisted ureterocalicostomy is a technically feasible procedure with the inherent advantages of magnified vision, precise dissection, and meticulous suturing providing a minimal access solution for a complex reconstructive technique. Moreover, near infrared fluorescence shows promise and the early surgical outcomes are definitely encouraging. However, these outcomes need to be validated in a multi-institutional, prospective setting with a larger patient cohort.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.