
Abstract
Abstract
Purpose:
Effects of laparoscopic sleeve gastrectomy (LSG) on gastroesophageal reflux disease (GERD) symptoms are controversial. Our aim is to evaluate the effects of LSG on GERD symptoms in obese patients using a validated quality-of-life questionnaire.
Methods:
Records of 100 patients (median body mass index [BMI] 44.4 kg/m2, range 35–63.6) without hiatal hernia or severe GERD were analyzed. GERD symptoms were evaluated by GERD Health-Related Quality-of-Life (HRQL) questionnaire before and after surgery. Weight loss and comorbidity resolution were recorded.
Results:
Median GERD-HRQL scores decreased from 7 (range 0–44) to 3 (0–34) (P = .025) (median follow-up 56 months [range 7–136]). GERD-HRQL scores improved in 55 patients and worsened in 21; de novo GERD was observed in 10; no change occurred in 14 patients (differences being statistically significant: P = <.0001). On multilinear regression analysis, total preoperative GERD-HRQL score and postoperative BMI were independent variables for overall postoperative GERD-HRQL score: higher total preoperative GERD-HRQL score was associated with improved postoperative GERD-HRQL scores, whereas higher postoperative BMI was associated with worse total postoperative GERD-HRQL score. Resolution of diabetes, hypertension, and sleep apnea syndrome occurred in 84.4%, 68%, and 89.7% of patients, respectively.
Conclusions:
In obese patients, although LSG was associated with statistically significantly improved postoperative GERD-HRQL scores at mid-term follow-up in 55% of patients, only preoperative GERD-HRQL score and postoperative BMI were independent predictors of GERD after LSG. Higher overall preoperative GERD-HRQL score was associated with improved postoperative GERD-HRQL score. However, further research is needed to assess how to predict GERD outcome.
Introduction
Laparoscopic sleeve gastrectomy (LSG) has gained widespread popularity and is presently the most popular bariatric surgical procedure both in USA and in Europe.1–4 This technique has shown excellent results in terms of sustained weight loss and comorbidity resolution, with low postoperative morbidity.5,6
In obese patients who are candidates for surgery for obesity, the rate of gastroesophageal reflux disease (GERD) ranges between 50% and 70%.6–8 GERD in the obese is thought to be the result of increased intra-abdominal pressure, irrespective of the presence of hiatal hernia or not. 9 While laparoscopic Roux-en-Y gastric bypass (LRYGB) is the treatment of choice for this subset of patients for some authors,9–11 however, it is not clear whether the improvement of symptoms is due to the bariatric procedure, to associated hiatal repair when performed, or both.9,12 Likewise, the effects of LSG on GERD symptoms are not completely clear. Some authors have reported improvement of symptoms, 9 whereas others have reported de novo GERD in 0%–93% of patients.13–15
Our aim is to evaluate the effects of LSG on GERD symptoms in obese patients using a validated quality-of-health questionnaire.
Materials and Methods
This study is a retrospective analysis of prospectively collected data. The study was approved by our Institutional Review Board, and informed consent was obtained from all participants.
All patients were studied and selected to undergo surgery for obesity according to National and International Guidelines16,17 as indicated in Table 1.
Inclusion and Exclusion Criteria
BMI, body mass index; LAGB, laparoscopic adjustable gastric banding; LRYGB, laparoscopic Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy.
Based on these criteria, from October 2006 to July 2017, 125 obese patients underwent LSG in our Unit. Of these, 25 were lost to follow-up leaving 100 patients with sufficient data for analysis.
Patient characteristics are shown in Table 2. Twenty-three men and 77 women with median preoperative body mass index (BMI) of 44.4 kg/m2 (range 35–63.6) were included. Comorbidities were type 2 diabetes mellitus in 45 patients, hypertension in 53, and sleep apnea syndrome in 39, 21 of whom were undergoing continuous positive airway pressure (CPAP) therapy at the time of surgery (Table 2).
Patients' Characteristics
As denominator was 100, absolute numbers and percentage are the same.
BMI, body mass index; CPAP, continuous positive airway pressure; LAGB, laparoscopic adjustable gastric banding; T2DM, type 2 diabetes mellitus.
Questionnaire
All patients were asked to respond to the GERD Health-Related Quality-of-Life (GERD-HRQL)-validated questionnaire before and after surgery.18,19 Each of the 10 questions were rated from 0 (absence of symptoms) to 5 (severe symptoms) for a total score that may range from 0 to 50 (Fig. 1). Symptoms were defined as absent when patients reported a GERD-HRQL score of 0, mild from 1 to 15, moderate from 16 to 30, and severe from 31 to 50.
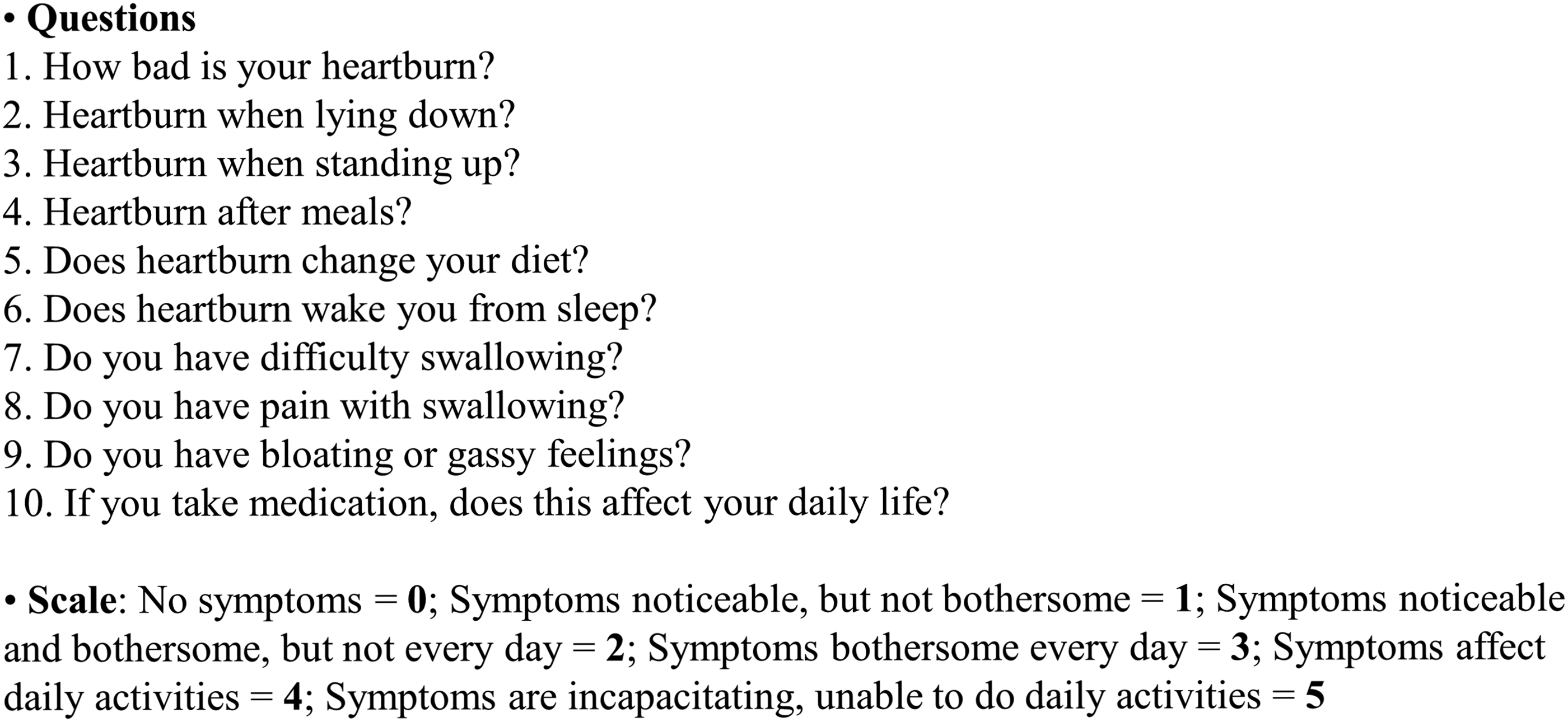
Gastroesophageal reflux disease Health-Related Quality-of-Life (GERD-HRQL) questionnaire. 18
Surgical technique
LSG was performed in a standardized fashion as previously reported.6,17 The bougie size changed with time, starting with the 48F, then the 42F, and lastly the 36F bougie, according to evolving International Bariatric Society recommendations during this time period. 20
Outcomes of interest
For each patient, a drop in postoperative score (lower than the preoperative score) was considered as an improvement of symptoms and, conversely, a higher postoperative score was considered as worsening of symptoms. De novo GERD was defined when patients with preoperative GERD-HRQL score of 0 reported a postoperative GERD-HRQL score ≥1. Unchanged GERD symptoms were considered when the pre- and postoperative questionnaire scores were identical.
To evaluate the success of the procedure, postoperative BMI and percentage excess body mass index loss (%EBMIL) were recorded according to previously described criteria. 21 Resolution or improvement of comorbidities were evaluated based on pharmacological or CPAP therapy discontinuation. If the therapy was interrupted, the comorbidity was considered to be resolved. If the dose or number of administered drugs was reduced, the comorbidity was considered to be improved. If the therapy was unchanged, comorbidity was considered to be stable. 15
Follow-up course
Our multidisciplinary follow-up program included clinical examination and blood tests at 3, 6, 9, and 12 months for the first year, every 6 months in the second year, and then once a year onward. Pre- and postoperative GERD-HRQL results were recorded between 1 and 30 days before surgery and at a median of 56 months (range 7–136) after surgery.
Statistical analyses
Data are presented as median and range. The Mann–Whitney U test was employed to evaluate the differences between groups. Linear regression analysis was performed to assess the relationship between the following parameters, age, gender, pre- and postoperative BMI, bougie size, EBMIL, total preoperative questionnaire score, and follow-up duration (independent variables) and the postoperative questionnaire score (dependent variable). All variables with P < .05 in univariate analysis were included in the multiple regression analysis with step-wise regression.
A P-value lower than .05 was considered statistically significant. Statistical analyses were carried out with SPSS software 22.0 (SPSS, Inc., Chicago, IL).
Results
Median pre- and postoperative GERD-HRQL scores were 7 (range 0–44) and 3 (range 0–34), respectively (P = .025) (Table 3). GERD-HRQL score improved in 55 and worsened in 21 patients. De novo GERD was observed in 10 patients, whereas no changes were recorded in 14 (Table 3). The differences in GERD-HRQL scores in patients with improved, worsened, and de novo GERD were statistically significant (P = <.0001 in all cases) (Table 3). Median pre- and postoperative GERD-HRQL scores in patients with de novo GERD were 0 and 3.5 (range 1–15), respectively (P = <.0001) (Table 3). Overall, 13 patients with median preoperative GERD-HRQL score 8 (range 2–34) reported no symptoms after surgery (questionnaire score: 0, P = <.0001).
Gastroesophageal Reflux Disease Health-Related Quality-of-Life Questionnaire Score Before and After Surgery
As denominator was 100, absolute numbers and percentage are the same. Statistically significant differences in bold.
BMI, body mass index; GERD-HRQL, gastroesophageal reflux disease Health-Related Quality of Life.
The median postoperative GERD-HRQL score value was significantly higher in patients with postoperative BMI ≤29.9 (44 patients) versus those with postoperative BMI ≥30 (56 patients) (8.5 [range 0–34] versus 2 [range 0–27]) (P = <.0001) at a median follow-up of 57 and 51 months, respectively (Table 4). The difference between the median pre- and postoperative GERD-HRQL scores was statistically significant in the group of patients with BMI ≥30 only (P = .008) (Table 4). The difference in median postoperative GERD-HRQL scores between patients with postoperative %EBMIL ≤49.9 (21 patients, median 1, range 0–23) versus ≥50 (79 patients, median 4, range 0–34) was not statistically significant (P = .120) at a median follow-up of 61 and 56 months, respectively (Table 4). The difference between the median pre- and postoperative GERD score was statistically significant in the group of patients with %EBMIL ≥50 (P = .010) (Table 4). The GERD-HRQL score also varied according to bougie size, as reported in Table 5. Patients undergoing LSG with the 48F had poorer weight loss results but less patients had GERD symptoms after operation.
Gastroesophageal Reflux Disease Health-Related Quality-of-Life Questionnaire Score According to Postoperative Body Mass Index
Statistically significant differences in bold.
BMI, body mass index; %EBMIL, percentage excess body mass index loss; GERD-HRQL, gastroesophageal reflux disease Health-Related Quality of Life.
Gastroesophageal Reflux Disease Health-Related Quality-of-Life Questionnaire Score According to Bougie Size
Statistically significant differences in bold.
BMI, body mass index; F, French; GERD-HRQL, gastroesophageal reflux disease Health-Related Quality of Life.
According to step-wise regression, preoperative GERD-HRQL score and postoperative BMI were independent predictors of GERD after LSG: higher overall preoperative GERD-HRQL score was associated with improved postoperative GERD-HRQL scores, whereas higher postoperative BMI was associated with a worse total postoperative GERD score.
At median follow-up of 56 months (range 7–136), median postoperative BMI was 30.7 kg/m2 (range 20–52.1) (P = <.0001) and median %EBMIL was 69.9 (range 3.2–149.6) (Table 6). The degree of postoperative GERD symptoms is reported in Table 7.
Median Follow-up, Pre- and Postoperative Body Mass Index and Percentage Excess Body Mass Index Loss of the Entire Series
Statistically significant differences in bold.
BMI, body mass index; EBMIL, excess body mass index loss.
Degree of Gastroesophageal Reflux Disease Symptoms Before and After Surgery
As denominator was 100, absolute numbers and percentage are the same.
GERD-HRQL, gastroesophageal reflux disease Health-Related Quality of Life.
Resolution of type 2 diabetes mellitus, hypertension, and sleep apnea syndrome was observed in 38 (84.4%), 36 (68%), and 35 (89.7%) patients, respectively (Table 8). No patients had worsening of comorbidities (Table 8).
Postoperative Comorbidity Data
As denominator was 100, absolute numbers and percentage are the same.
CPAP, continuous positive airway pressure; LSG, laparoscopic sleeve gastrectomy; T2DM, type 2 diabetes mellitus.
Discussion
In this retrospective analysis of 100 patients, LSG was associated with significantly improved GERD symptoms at mid-term follow-up in 55% of patients. However, in 21% of patients, GERD symptoms worsened, and an additional 10% of patients developed de novo GERD. Symptoms were unchanged in 14%. Moreover, patients with high preoperative GERD-HRQL scores had better total postoperative GERD-HRQL scores, whereas patients with high postoperative BMI had a worse total postoperative GERD-HRQL score.
At present, LRYGB is the treatment of choice for obese patients with GERD.9,22 According to the American Society for Metabolic and Bariatric Surgery guidelines, preoperative upper gastrointestinal endoscopy and pH-manometry are not mandatory before surgery for obesity or related comorbidity, and in everyday clinical practice the preoperative diagnosis of GERD most often relies on patients' self-reporting of symptoms, with low reliability. 23 This is in accordance with the review by Stenard et al., in which 6 of the 25 studies reported their outcomes based on clinical evaluation only. 24 Of note, preoperative work-up for GERD in our population included the GERD-HRQL score and routine upper gastrointestinal endoscopy.
Our improvement rate of 55% was slightly less than that of Coupaye et al. (62.5%), 25 but much higher than most of the studies reported in the literature (7%–36.4%).26–31 Our 21% worsening and 10% de novo GERD rates were well within the ranges reported in the literature (12.6%–39.6% and 8.6%–17.7%, respectively), but less than 37.5% worsening rate reported by Coupaye et al. 25 This wide variability in reporting, the use of pH-metry or not, and self-reported underestimation of GERD symptoms may be the reasons for controversial outcome data regarding reflux symptoms after LSG.25,29,32,33 One further possible explanation for our results on GERD symptoms might be that different bougie sizes were employed along the course of our experience. In fact, when we compared patients treated with the 48F versus 42F bougie, both weight loss and GERD symptoms increased, probably due to a narrower sleeve and to increased intragastric pressure.
In our study, median postoperative BMI (30.7 kg/m2, range 20–52.1 kg/m2) and median %EBMIL (69.9%, range 3.2%–149.6%) as well as resolution of comorbidities, were compatible with others studies, an assurance that our technique was adequate. Moreover, weight loss was associated with an overall improvement of GERD symptoms, as reported by others. 24
The major weaknesses of this study are the subjectivity of the cutoff values to define the mild/moderate/severe categories of GERD, the lack of objective GERD criteria (24-hours pH manometry) before and after surgery, the retrospective nature of the study, and the absence of a standardized fixed time for the patients to answer the questionnaire. Moreover, as we did not include patients having concomitant LAGB removal or hiatal hernia repair during LSG, to better evaluate the effect of LSG alone without other possibly confounding factors, we cannot interpret any of the percentages as prevalence or incidence.
In obese patients, although LSG was associated with statistically significantly improved postoperative GERD-HRQL scores at mid-term follow-up in 55% of patients, only preoperative GERD score and postoperative BMI were independent predictors of GERD after LSG. Higher overall preoperative GERD-HRQL score was associated with improved postoperative GERD scores, whereas higher postoperative BMI was associated with a worse overall postoperative GERD score. As sleeve gastrectomy is performed more and more often, and between 50% and 70% of obese patients have symptoms of GERD, further prospective studies with a larger sample size, clinical and instrumental data, including 24-hour pH manometry, upper gastrointestinal endoscopy, and barium swallow, and longer follow-up are necessary to be able to offer LSG to those patients who would most benefit from this procedure.
Footnotes
Disclosure Statement
Dr. Andrea Balla, Dr. Silvia Quaresima, Dr. Livia Palmieri, Dr. Ardit Seitaj, Prof. Annamaria Pronio, Prof. Danilo Badiali, Prof. Abe Fingerhut, Dr. Pietro Ursi and Prof. Alessandro M. Paganini report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
Funding Information
No funding was received.