
Abstract
Introduction:
Oncological and surgical safeties are pivotal issues of cancer operations. Robotic thyroidectomy adds cosmetic advantage to those safeties. We have performed bilateral axillo-breast approach robotic thyroidectomies (BABART) since 2009 and recently started transoral robotic thyroidectomy (TORT) in 2017. This study aimed to compare the surgical outcomes of a single surgeon's initial TORT and BABART.
Materials and Methods:
We retrospectively collected data of 103 patients who underwent robotic thyroid lobectomy for papillary thyroid cancer and analyzed the first 14 and 56 cases of TORT and BABART, respectively, after propensity score matching. The surgeon performed 224 BABARTs before starting TORT.
Results:
There were no significant differences between the BABART and TORT groups in mean age (40.02 ± 9.37 versus 38.69 ± 9.21 years, respectively; P = .7520), sex distribution (P = .3697), mean body mass index (23.60 ± 4.31 versus 23.87 ± 2.45 kg/m2, respectively; P = .4737), and tumor size (0.75 ± 0.35 versus 0.76 ± 0.29 cm, respectively; P = .9969). The TORT group had a longer operative time than the BABART group by 78.04 minutes (P < .0001). The visual analog scale pain scores on postoperative day (POD) 2 and POD 3 were higher in the TORT than the BABART group by 0.59 and 0.77, respectively (P = .0227 and .0119, respectively). The number of retrieved lymph nodes and unintended parathyroidectomies was similar in the two groups. There were no severe complications such as tracheal injury, transection of recurrent laryngeal nerve, or surgical site infection.
Conclusion:
Our study suggests that both BABART and TORT are safe and feasible during the initial period. TORT can be undertaken without any adverse event if the operator is experienced with other robotic thyroidectomy. The patients may choose the surgical approach based on their preference.
Introduction
The gold standard of thyroid surgery is the conventional transcervical approach established by Theodor Kocher “the father of thyroid surgery” in the late 1880's. 1 This approach has the advantage of easy access to the thyroid gland, but the disadvantage of a visible scar on the anterior neck, which can lead to a displeasing result and negatively affect the patient's quality of life. 2 Therefore, over the last two to three decades, minimally invasive surgery or oncoplastic surgery has aimed to minimize the length of the wound and avoid scarring in the area of the thyroid surgery.
With the advancements in surgical techniques and instruments, robotic thyroidectomy has become widespread. The most common methods of robotic thyroid surgery are the transaxillary approach (TAA) and the bilateral axillo-breast approach robotic thyroidectomy (BABART). 3 These methods achieve the goal of minimal scarring by moving the surgical incision to the invisible areas, such as axilla or areola, but have the disadvantage of extensive dissection, which is inevitable to create a working space due to the remote-access approach. Therefore, it is unreasonable to call them minimally invasive surgery.
On the other hand, the transoral robotic thyroidectomy (TORT), using the concept of natural orifice transluminal endoscopic surgery (NOTES), has been highlighted to comply with the principles of minimally invasive surgery as it minimizes the range of flap dissection through closer access, as compared with the BABART or TAA methods. Additionally, TORT has the advantage of oral mucosal incisions, which are completely invisible and can heal without keloids or hypertrophic scars. The transoral thyroid surgery can be performed through a sublingual approach, oral vestibular access, or a combined sublingual and oral vestibular approach. 4 The sublingual and combined approaches are difficult and likely to injure the floor of the mouth (related to high complication rate), therefore the oral vestibular approach is generally preferred due to its safety and lesser traumatic profile. However, the efficacy and feasibility of TORT have not fully evaluated as the technique is still in the infantile stage.
We aimed to report our initial experience of TORT performed by a single surgeon, and compare the surgical outcome of TORT with those of BABART for feasibility and safety.
Materials and Methods
Study population and data collection
We retrospectively collected data of all the patients who underwent robotic thyroidectomy by an experienced single surgeon (W.S. Park) at the Kyung Hee University Medical Center from February 2009 to April 2019. Out of the 246 patients who underwent robotic thyroidectomy, 230 underwent BABART, which was launched in February 2009, and 16 patients underwent TORT, started in October 2017. After a thorough explanation of BABART and TORT, the surgical method was decided according to the patient's preference. There was only 1 case of total thyroidectomy in the TORT group. Therefore, we included patients who underwent lobectomy with or without central neck dissection (CND) for thyroid cancer in this study for an adequate comparison between the two groups. In most cases, prophylactic or therapeutic CND was performed, but CND was not performed in some cases of a small tumor without evidence of extrathyroidal extension (ETE) and lymph node metastasis. The patients who received lobectomy for benign nodules and patients who received lobectomy with lateral neck dissection were excluded. A total of 103 patients who met the criteria were identified and 70 patients were eventually enrolled in this study after propensity score matching (PSM); 56 patients were included in the BABART group and 14 patients were included in the TORT group. A flow chart of the study is presented in Figure 1. Surgical outcomes, including operation time, hospital stay, completeness of surgical resection, number of retrieved lymph nodes, presence of parathyroid gland in permanent specimen, postoperative pain, and postoperative complications, such as tracheal injury, recurrent laryngeal nerve (RLN) injury, transient hoarseness, wound seroma, wound infection, and flap perforation were compared between the two groups.
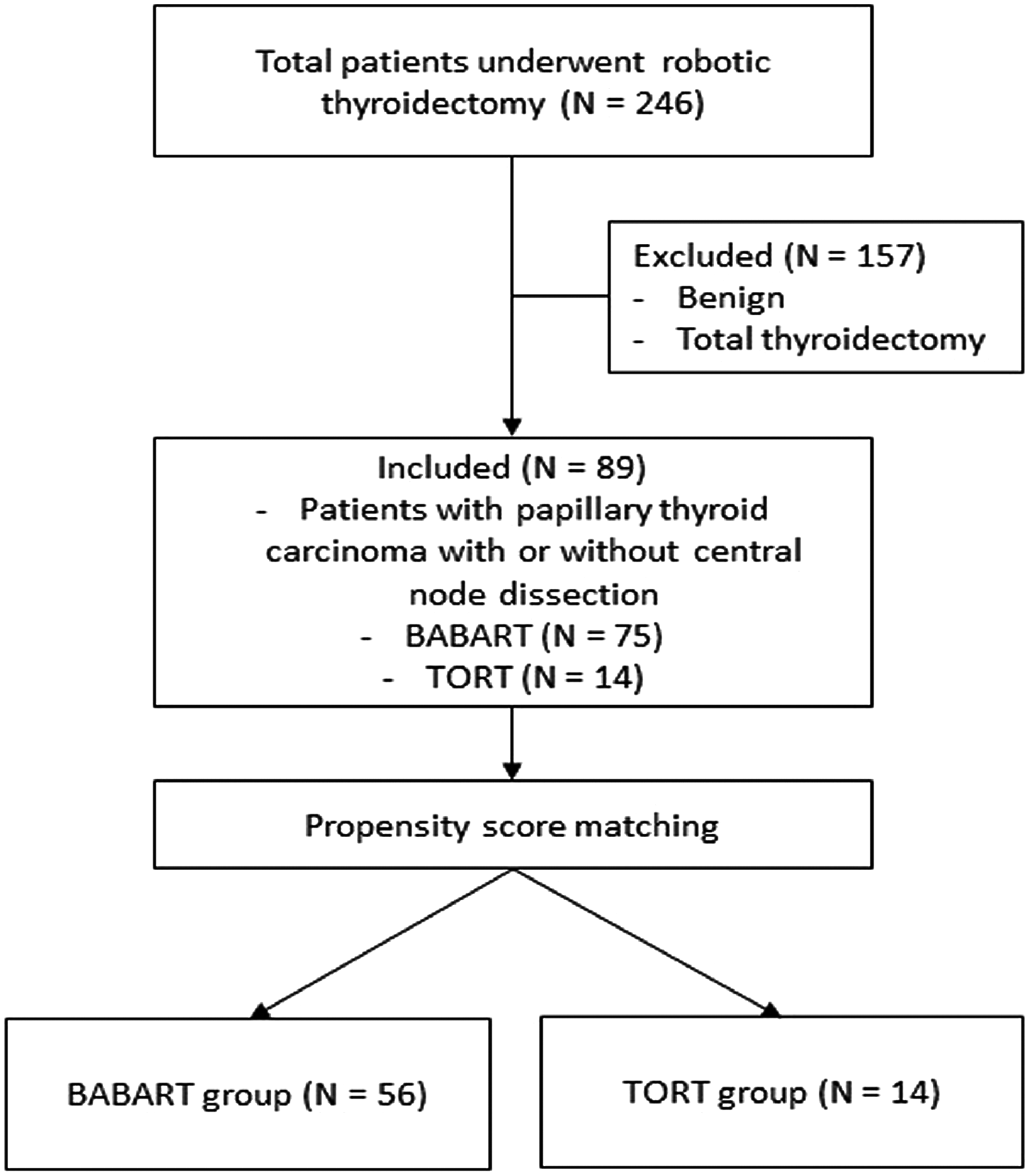
Diagram of the study population. BABART, bilateral axillo-breast approach robotic thyroidectomy; TORT, transoral robotic thyroidectomy.
The size of the tumor was determined by the longest diameter of the largest tumor in cases of multiple masses. The operative time was determined from skin incision to closure. The postoperative pain was measured using the visual analog scale (VAS) score (0–10 points) on the day of the surgery, first, second, and third postoperative days (PODs); and the mean value of the VAS scores was calculated for each day. The period of hospitalization was defined from the day of surgery to the day of discharge. The vocal fold motion was routinely assessed with laryngoscopy preoperatively and at the first outpatient visit after discharge; additional laryngoscopic examinations were performed at every visit when symptoms such as hoarseness persisted. Permanent RLN injury was defined as vocal cord palsy persisting after 6 months. Prophylactic intravenous (IV) antibiotics were given before making incisions. To alleviate postoperative pain, IV pain killers were administered along with fluids on the day of operation and oral pain killers were routinely administered twice a day until discharge. A neural integrity monitor (NIM-Response 3.0 System; Medtronic Xomed, Jacksonville, FL) was utilized for all the cases.
Operation methods
All robotic thyroidectomies were performed by an experienced single surgeon (W.S. Park) with the da Vinci Si Surgical Robot System (Intuitive Surgical, Inc., Sunnyvale, CA).
Bilateral axillo-breast approach robotic thyroidectomy
The BABART was performed as described by Lee et al. 5 Briefly, the patient was placed in the supine position with the neck extended and both arms adducted. We used normal saline administration for flap elevation instead of diluted epinephrine. An 18 mm incision was made for videoscopy along the superomedial margin of the areola on the right side and a 12 mm incision was made on the left areola for the robotic instruments. After blunt dissection of the subcutaneous tissue of the breast, a subplatysmal working space was created with an avascular tunneler. Following insertion of a 12 mm trocar through the incision, the working area was inflated with CO2 gas at a pressure of 6 mm Hg; a 10 mm robotic videoscope was then inserted through the trocar. Two additional robotic 8 mm da Vinci trocars were inserted through the incision at both axillae, respectively. Figure 2 shows the state after insertion of all the trocars in BABART. The patient-side cart of the da Vinci surgical system was docked to the trocars. The working space was widely bordered by the thyroid cartilage superiorly, 5 cm below the clavicle inferiorly and just beyond the lateral border of the sternocleidomastoid muscle (SCM) laterally. The midline division of the strap muscle was performed using a hook monopolar electrocautery. After visualization of the cricothyroid membrane, isthmus, and the central group of lymph nodes, the isthmus was separated using an ultrasonic shear. The lateral side of the thyroid gland was dissected. The thyroid lobe was retracted upward and dissected from the trachea and surrounding connective tissue in the lateral margin of the lobe. The parathyroid glands were identified and saved. With careful manipulation for dissection, the RLN was identified and preserved. If necessary, prophylactic or therapeutic CND was done. The resected specimen was removed using an endopouch through the axillary incision. Hemostasis was achieved meticulously, and a hemostatic glue and an antiadhesion barrier solution were coated onto the flap. Next, a Jackson-Pratt (JP) drain was placed in the thyroid bed through the axillary incision. The divided strap muscles were sutured continuously with absorbable threads and the skin incisions were closed using subcutaneous sutures.

Position after insertion of all trocars in BABART. BABART, bilateral axillo-breast approach robotic thyroidectomy.
Transoral robotic thyroidectomy
The TORT was performed as first described by Richmon and Kim.6,7 The patient was placed in a lithotomy position with the neck extended. Hydrodissection was performed with a 20–50 mL of epinephrine–saline diluted solution (1:200,000) administered into the oral vestibular area of the lower lip down to the chin and the anterior neck. After inverted U-shaped 20 mm incision was made at the midline in the lower lip, blunt tunneling was performed to widen the working space. A 12 mm videoscopic port was inserted at the midline of the lower lip. Two lateral incisions were made near the lateral junction of the lower lip, and 5 mm ports were placed after hydrodissection with an epinephrine–saline solution. Figure 3 shows the state after insertion of all the trocars in TORT. Using a 10 mm 30° videoscope with craniocaudal visualization, a working space was created down to the sternal notch and laterally to the lateral border of the SCM muscles. An additional 8 mm port was inserted at the right axillary area, and then the robot was docked. The midline of the sternohyoid muscle was separated by a hook monopolar cautery. The isthmus was divided using an ultrasonic shear, and a lateral dissection was performed by separating the thyroid from the sternothyroid muscle. Next, the superior pole and the cricothyroid muscle were dissected along an avascular plane, and the branches of the upper pole vessels were divided and sealed using an ultrasonic shear. The upper parathyroid gland was identified and preserved. The thyroid gland was carefully dissected while retracting upward, and the RLN was identified at the insertion to the larynx near the Berry's ligament and preserved. Using the NIM, the surgeon confirmed the integrity of the RLN. While dissecting in the craniocaudal direction, the thyroid was separated from the trachea after preservation of the lower parathyroid gland. If necessary, prophylactic or therapeutic CND was performed. The subsequent procedures of the surgery, such as removal of the specimen, hemostasis, placement of a drain, and closure of the wounds, were performed similar to a BABART. The video clip of the procedure for the first case of TORT was edited with a focus on the key steps and can be found in the Supplementary Video S1.

Position after insertion of all trocars in TORT. TORT, transoral robotic thyroidectomy.
Statistical analyses
A PSM was conducted to minimize selection bias and the potential confounding effects on the surgical outcomes. The following variables were included in the PSM: age, sex, body mass index (BMI), extent of lymph node dissection, pathological type, tumor size, multiplicity, ETE, and the American Joint Committee on Cancer (AJCC) TNM stage (eighth edition). Fourteen patients who underwent TORT were matched in a 1:4 ratio with 56 patients who underwent BABART. The demographic data and the surgical outcomes for the subgroups were then compared using the Fisher's exact test for categorical variables and the Mann–Whitney U test for continuous parametric variables. The operative times were compared using the Mann–Whitney U test as they were assumed to be nonparametric. The continuous variables were presented as mean ± standard deviation or median with interquartile range (Q1–Q3) and were compared between the two groups using an independent t-test or the Mann–Whitney U test depending on the distribution. The categorical variables were presented as frequency with percentage and were compared between the groups using the Fisher's exact test. The generalized linear model was used with surgical outcomes as a dependent variable, including operative time, length of hospitalization, number of retrieved lymph node, and postoperative pain. The logistic regression was performed with variables such as the number of unintended parathyroidectomies and complications. The Firth penalized likelihood approach was used to reduce small sample bias. The estimates from the regression models were presented corresponding to 95% confidence intervals (CIs). Statistical significance was set at a P value <.05. All the statistical analyses were performed using SPSS 23 (Statistical Package for Social Science, version 23.0; IBM Corporation, Chicago, IL) and R 3.5.1.
This study was approved by the Institutional Review Board of Kyung Hee University Medical Center and informed consent acquisition was waived.
Results
The baseline demographic characteristics of the patients are presented in Table 1. The mean age of the patients was 40.88 ± 9.80 years and the mean BMI was 23.66 ± 4.00. All the operations were completed as intended without open conversion; all the patients achieved R0 resection. Most of the cases were diagnosed as papillary thyroid cancer (PTC) with an average size of 0.73 ± 0.35 cm. The multiplicity of thyroid cancer was founded in 9 (10.11%) patients. Microscopic or macroscopic ETE was found in 29 (32.58%) patients. According to the AJCC eighth edition, 88 (98.88%) patients were classified as stage I. The average operative time was 233.60 ± 56.27 minutes. Most patients underwent a unilateral CND and the average number of retrieved lymph nodes was 3.19 ± 3.09. According to the final pathology results, the parathyroid was found in 19 cases. Complications occurred only in some cases: 1 case of tracheal injury; 8 cases of transient hoarseness; 1 case of flap perforation; and 1 case of wound seroma. All these patients were treated completely without any minor sequela. The average duration of hospital stay after surgery was 3.34 ± 0.87.
Baseline Characteristics of Patients
BMI, body mass index; CND, central neck dissection; FVPTC, follicular variant of papillary thyroid carcinoma; POD, postoperative day; PTC, papillary thyroid carcinoma; RLN, recurrent laryngeal nerve; SD, standard deviation; VAS, visual analog scale.
The comparison of baseline characteristics between the groups is presented in Table 2 and Supplementary Table S1: the former shows the results after PSM and the latter shows the result before matching. The PSM increased efficiency by 30.92% (Supplementary Table S2).
Baseline Characteristics of Patients After Propensity Score Matching
Mann–Whitney U test.
Fisher's exact test.
BABART, bilateral axillo-breast approach robotic thyroidectomy; BMI, body mass index; CND, central neck dissection; FVPTC, follicular variant of papillary thyroid carcinoma; POD, postoperative day; PTC, papillary thyroid carcinoma; RLN, recurrent laryngeal nerve; SD, standard deviation; TORT, transoral robotic thyroidectomy; VAS, visual analog scale.
In the analysis using the PSM, the patients with follicular variant PTC, those underwent bilateral CND, and those diagnosed with stage II were excluded from the comparison. In terms of surgical outcome, R0 resection was performed in all the operations. There was no significant difference in the number of retrieved lymph nodes and hospital stay after operation between the two groups. The parathyroid was detected on final pathology in 12 (21.43%) patients who underwent BABART and 3 (21.43%) who underwent TORT. There was no significant difference between the two groups and none developed hypocalcemia because all underwent lobectomy. Although not statistically significant, 6 (10.71%) patients developed transient hoarseness in the BABART group; this was not observed in the TORT group. All the patients who developed transient hoarseness improved during follow-up. Wound seroma occurred in only 1 case of the BABART group, which improved after a single aspiration. There was no tracheal or esophageal injury, RLN injury, and surgical site infection in both groups. A JP drain was inserted in all the cases, and there was no postoperative bleeding or chyle leakage. No TORT-specific surgical complications such as mental nerve injury, zygomatic bruising, or oral commissure tearing were observed, except for 1 case of perforation of the chin flap. Flap perforation occurred in the eighth case, which was immediately sutured and healed without the need for additional intervention during follow-up. The VAS pain score on the day of the surgery was not different between the two groups, whereas those from POD 1 to POD 3 were significantly lower in the BABART group. The operative time was significantly longer in the TORT group when compared with that in the BABART group (299.64 ± 52.46 versus 221.61 ± 50.19, respectively, P < .0001). The operative time for TORT tended to decrease gradually even though there was a variation by case. This is shown in Figure 4.
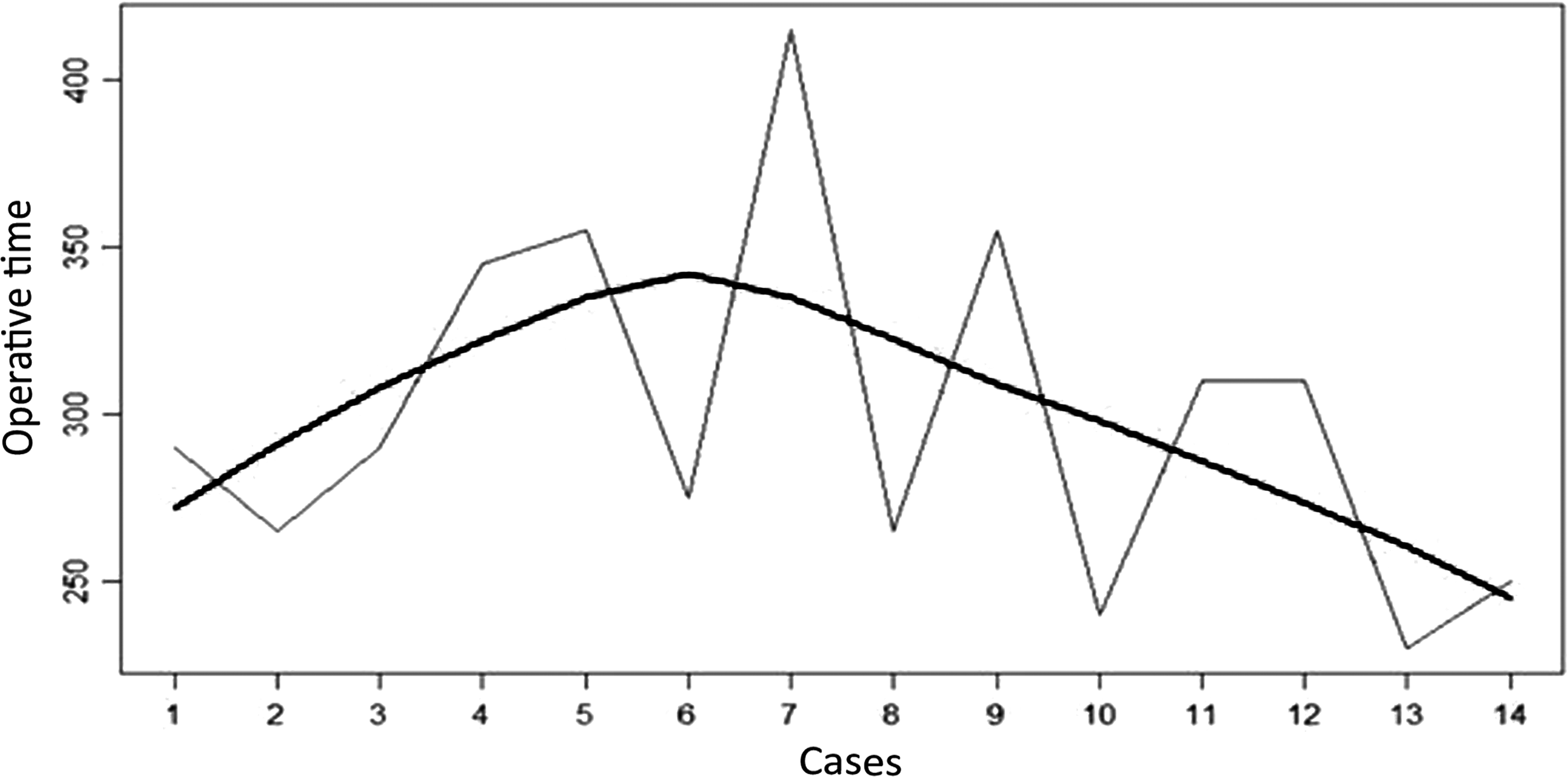
Operative time for the TORT cases. TORT, transoral robotic thyroidectomy.
Using the generalized linear model, the TORT group had an increased operative time by 78.04 minutes when compared with the BABART group (95% CI 47.85–108.22, P < .0001). The VAS pain scores on POD 2 and POD 3 were increased in the TORT group when compared with the BABART group by 0.59 and 0.77, respectively (95% CI 0.09–1.08, P = .0227, 95% CI 0.17–1.35, P = .0119, respectively) (Table 3). In terms of surgical complications, there was no significant difference between the operative methods according to the logistic regression of Firth's penalized likelihood method (Supplementary Table S3).
Generalized Linear Model for Variables According to Operation Methods
BABART, bilateral axillo-breast approach robotic thyroidectomy; CI, confidence interval; POD, postoperative day; TORT, transoral robotic thyroidectomy; VAS, visual analog scale.
Discussion
According to the Korea Central Cancer Registry, there were 26,051 cases of thyroid cancer in 2016, which accounted for 11.4% of all cancers. 8 Many patients scheduled to undergo thyroidectomy are concerned about scarring due to the incision in the anterior neck. Therefore, robotic thyroidectomy has recently become very popular in Korea due to the good esthetic results and the excellent surgical view with 3D magnification. Although BABART and TAA comprise a large portion of robotic thyroidectomies, these methods have a weak point of a somewhat wide area of dissection and therefore it is difficult to consider them as truly minimally invasive. Therefore, the TORT, an adaptation of the concept of NOTES, with a small area of dissection has recently taken center stage. In 2008, a transoral thyroidectomy was first reported by Witzel et al. in Germany. 9 They performed surgery on living pigs with a sublingual approach. Therefore, the transvestibular approach, safer and less traumatic than the sublingual approach, has become more popular and many studies have reported the results of the transoral thyroidectomy through the transvestibular approach.10,11 However, the technical difficulty of the procedure despite its minimal invasiveness has limited the uptake of TORT. We tried to evaluate the feasibility of TORT by reporting the initial experience of TORT and comparing it to BABART.
Our study showed that TORT had an advantage in terms of prevention of transient hoarseness compared with BABART. However, it was found that the TORT had longer operative time and more pain than the BABART. RLN injury is a most important complication in thyroid surgery. According to a previous study, intraoperative neuromonitoring (IONM) during thyroid surgery made it easier to identify the RLN and to understand the mechanism of RLN damage. 12 In our study, IONM was routinely performed and there was no complication involving transection of the RLN. However, transient hoarseness occurred in 6 patients, all of whom were in the BABART group. Transient hoarseness is thought to be caused by traction injury, and the reason that it was less common in the TORT group as compared with BABA group was that there is a difference in the method of traction of the thyroid during surgery. In the case of TORT, the RLN is found near the Berry's ligament. After cutting the Berry's ligament, dissection proceeds in a downward direction. Therefore, the risk of traction injury during lifting of the thyroid is reduced. 13 In terms of operative time, TORT took longer than BABART. This is because TORT is technically difficult as compared with BABART at the initial period. TORT should be performed in a craniocaudal direction, which differs from conventional thyroidectomy and BABART. It is difficult to access and completely manipulate the lesion especially when it is located on the superior pole because the mandible may restrict the movement of the instruments. Furthermore, the difficulty increases because the ultrasonic surgical devices are not angulated. In our study, 7 out of 14 patients in the TORT group had tumors located on the superior pole. The BMI is also one of the factors affecting the operative time. According to the WHO BMI cutoffs for Asian and Pacific populations, both groups had subjects in the overweight category. 14 There was no statistically significant difference between the two groups. The operative time may also have increased due to the complexity of flap formation, caused by the mental protuberance and the tubercle. Before starting a BABART, the operator had performed >100 cases of BABA endoscopic thyroidectomy. Therefore, all cases of the BABART group were after mastery of the learning curve of making the flap. The longer operative time of the TORT group was due to the initial experience of a beginner surgeon. In terms of postoperative pain, TORT, has the closest tract and smallest dissection area among the remote access robotic surgeries. Therefore, we expected the TORT group to have lower pain scores, but the result was different. It was probably due to the small number of samples.
In general, TORT provides a craniocaudal view so that the CND can be performed completely and easily up to level VI and VII, whereas BABART has a weakness while dissecting the lower central compartment. 15 However, in our study, there was no difference in the number of retrieved LNs between the two groups. The possible reason is that most of the cases in this study were early PTCs, which do not need aggressive CND.
Hypoparathyroidism is a common complication after thyroidectomy. Fewins et al. reported that hypoparathyroidism after thyroidectomy occurred in 6.9%–46% of cases. 16 Our study was conducted in patients who underwent lobectomy, so we did not routinely check PTH and calcium level postoperatively. No patient with symptoms of hypoparathyroidism and hypocalcemia was observed in both groups. Instead, we evaluated cases in which the parathyroid glands were removed without intention. There was no significant difference between the two groups.
As with chest sensory changes in BABART, TORT also has a specific injury such as mental nerve injury. The mental nerve passes through the mental foramen and is responsible for the sensation of the chin and lower lip. The mental foramen is located on the anterior surface of the mandible, the most common position being the longitudinal axis of the second premolar and generally at the level of the vestibule. Mental nerve damage is mainly caused by lateral trocar insertion and excessive stretching of the working port during the TORT operation. According to previous studies, the overall incidence of mental nerve injury was about 4.3%. 17 We tried to avoid this nerve injury and no mental nerve injury was observed in our study.
Another TORT-specific complication is infection because TORT is a clean-contaminated surgery. 18 Normal flora of the oral cavity may cause an increase in infection rate, but we tried to prevent infection with prophylactic antibiotics and thorough sterilization. There was no infection in our study.
Our study has some limitations. First of all, it is a retrospective single-center study with a small sample size. This may have decreased the statistical power. Second, the best strength of a TORT is the cosmetic effect as the oral mucosal wounds are perfectly hidden and heal without scarring. However, there was no objective evaluation of cosmesis. Third, the follow-up period was short and the long-term surgical outcomes were not evaluated. Despite these limitations, we gave meaning to report our initial experience with TORT. Our results suggest that TORT has acceptable surgical outcomes as compared with those by BABART. Further studies with a large number of cases and long-term follow-up are warranted to support the feasibility and efficacy of TORT.
In general, large tumor sizes can be a limitation for a TORT, because it is difficult to extract specimens through the port site. According to previous studies, the TORT can be performed well unless it exceeds 6 cm for benign tumors and 2 cm for malignancy. Aside from large tumor size, there are some cons of performing a TORT, such as the requirement of in-depth anatomical knowledge, difficulty in a superiorly located tumor, and infantile state of implementation. Nevertheless, the TORT can be a very good surgical procedure for selected patients especially, if the patient has a keloid constitution or wants to avoid scarring.
In our study, TORT was found to be comparable to BABART for the surgical outcome; both approaches are safe and feasible in properly selected patients during the initial period. A TORT can be performed without adverse event if the surgeon is experienced in other robotic thyroid surgery. According to this study, the patients may be given a chance to choose the surgical approach on the basis of their preference.
Footnotes
Acknowledgment
The authors thank the Division of Statistics of the Medical Research Collaborating Center of the Kyung Hee University Medical Center for statistical analyses.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.