
Abstract
Background:
Hidradenitis suppurativa (HS) is infrequent in the pediatric population. When indicated, surgery is often invasive, painful, and with significant recurrence rate. We aimed to report our preliminary experience using a new endoscopic technique to treat this pathology.
Materials and Methods:
We reported the data of 11 patients (9 girls and 2 boys) with average age of 15.7 years (range 14–17) with HS, who were operated using endoscopic procedure for a 15-month period. Six patients presented axillary, inguinal, and inframammary localizations, 3 patients presented axillary and inguinal localizations, and 2 patients presented only inguinal localization. Pediatric endoscopic hidradenitis treatment (PEHT) followed the same principles of pediatric endoscopic pilonidal sinus treatment (PEPSiT). The fistuloscope was introduced into the different holes, and after using an endobrush, all tracts were cauterized using monopolar electrode or laser energy, and finally the granulation tissues were removed using graspers. At the end of the procedure, all the holes were filled with oxygen-enriched oil-based gel and covered with fat gauze.
Results:
The average operative time was 47 minutes (range 30–80). All procedures were performed in a day surgery setting or with an overnight hospitalization. All patients reported no pain postoperatively and performed a local dressing with silver sulfadiazine spray and oxygen-enriched oil-based gel two times per day for 1 month postoperatively. At the longest follow-up of 1 year, the lesions were completely healed in all cases. Two patients (18%) developed further lesions in different untreated localizations that were successfully treated using PEHT.
Conclusions:
PEHT is a minimally invasive, effective, and safe treatment option for pediatric patients with HS. All patients reported a painless postoperative period and excellent results. Postoperative local dressings using oxygen-enriched oil-based gel and silver sulfadiazine spray are fundamental to achieve the complete healing. However, a further evidence with larger series and longer follow-up is required to confirm these preliminary results.
Introduction
Hidradenitis suppurativa (HS) is a chronic inflammatory disease that affects the apocrine glands in different areas of the body and is characterized by chronic or recurrent nodules that tend to suppuration and rupture with subsequent formation of abscesses, sinus tracts, and scarring.1,2 The most common localizations are axillae, inframammary folds, groin, perigenital, or perineal regions.3,4 HS usually appears after puberty and is infrequent in the pediatric population.5,6 The estimated prevalence of HS in adults is variable between 0.05% and 4.1%. 7 Very few data are available regarding the prevalence of HS in the pediatric population. In fact, the onset of HS has been reported before 11 years of age in <2% of cases, 5 and between 11 and 20 years in 35% of cases.8,9
The pathogenesis of HS is still under investigation and is probably multifactorial. 10 It seems linked to the obstruction of the apocrine glands that undergo bacterial superinfection and subsequent abscess formation. 10 Several associated comorbidities, such as polycystic ovary syndrome, obesity, diabetes, arthritis, Crohn's disease, and precocious puberty have been reported.11,12 HS may affect negatively the patients' quality of life because lesions are very painful. In addition, since the lesions are often located in the genital area, patients' social and sexual life is negatively affected.13,14
No gold standard treatment protocol supported by robust scientific evidence is currently available. 15 Treatment of HS includes both medical and surgical options. Medical therapeutic options include topical or systemic antibiotics, retinoids, topical resorcinol, and anti-TNFα drugs (infliximab and adalimumab) that have gained until now the highest level of scientific evidence in the treatment of moderate and severe HS. 16 In addition to medical treatment, surgery is often required to definitively treat the tunnels and scars associated with chronic HS. 15 Surgical treatment options include incisional drainage, limited excision using cold steel or electrosurgery, lesions' evaporation using carbon dioxide laser, and in some cases wide excision closed by primary intention using grafts, local or distant flaps; or left open for secondary intention healing.1,17 The available evidence regarding the outcome of these approaches is still limited and controversial. When open surgery is indicated, it is often invasive and painful and, despite the removal of significant amounts of tissue, remains associated with significant recurrence rate. 18
We aimed to report our preliminary experience using a new endoscopic technique to treat this pathology.
Materials and Methods
We reported the data of 11 consecutive patients (9 girls and 2 boys) with average age of 15.7 years (range 14–17) with HS, who were operated in our unit using endoscopic procedure for a 15-month period. Six patients (54.6%) presented axillary, inguinal, and inframammary localization, 3 patients (27.2%) presented axillary and inguinal localizations, and 2 patients (18.2%) presented only inguinal localization (Figs. 1 and 2). No associated comorbidities were recorded in our series. All patients were candidate to surgery after failure of previous medical therapy, including topical and general antibiotics, anti-inflammatory drugs, and the anti-TNFα agent, adalimumab. All patients and their parents signed a specifically formulated informed consent preoperatively.

Distribution of lesions in our series.

Different localizations of HS: axillary
Follow-up included clinical controls at 1, 2, and 4 weeks postoperatively, then every 3 months for the first year after surgery. All patients were evaluated postoperatively for healing, pain, complications, recurrence, and satisfaction. Primary outcome parameters included complete wound healing, defined as closure of all external holes in the first 60 days after surgery and disease recurrence. Secondary outcome parameters included length of surgery, healing time, and intra- and postoperative complications such as wound infections.
The study received the appropriate Institute Review Board (IRB) approval at Federico II University of Naples, Italy.
Operative technique
All patients were operated under general anesthesia and an antibiotic prophylaxis was administered intraoperatively. They were placed supine on the operative table with the legs and the arms opened to have an easy access to all affected areas and avoid changing the patient's position during surgery (Fig. 3). Two monitors, one placed at feet and the other at the head of the patient, were alternatively adopted to have a perfect view of all operative fields. The surgeon's position changed according to the location of the disease. Pediatric endoscopic hidradenitis treatment (PEHT) followed the same technical principles that we already described for endoscopic treatment of pilonidal sinus disease in pediatric patients (PEPSiT).19–21 Regarding the instrumentation, a 9.5F fistuloscope, manufactured by Karl Storz and equipped with a monopolar electrode, an endoscopic brusher, and an endoscopic grasper, was adopted in all patients (Fig. 4). As we already described,19–21 the fistuloscope presents an optical channel and a working and irrigation channel. In addition, it has a removable handle that can be moved in different positions to provide a better ergonomics to the surgeon (Fig. 4).

Patient's position during PEHT. PEHT, pediatric endoscopic hidradenitis treatment.
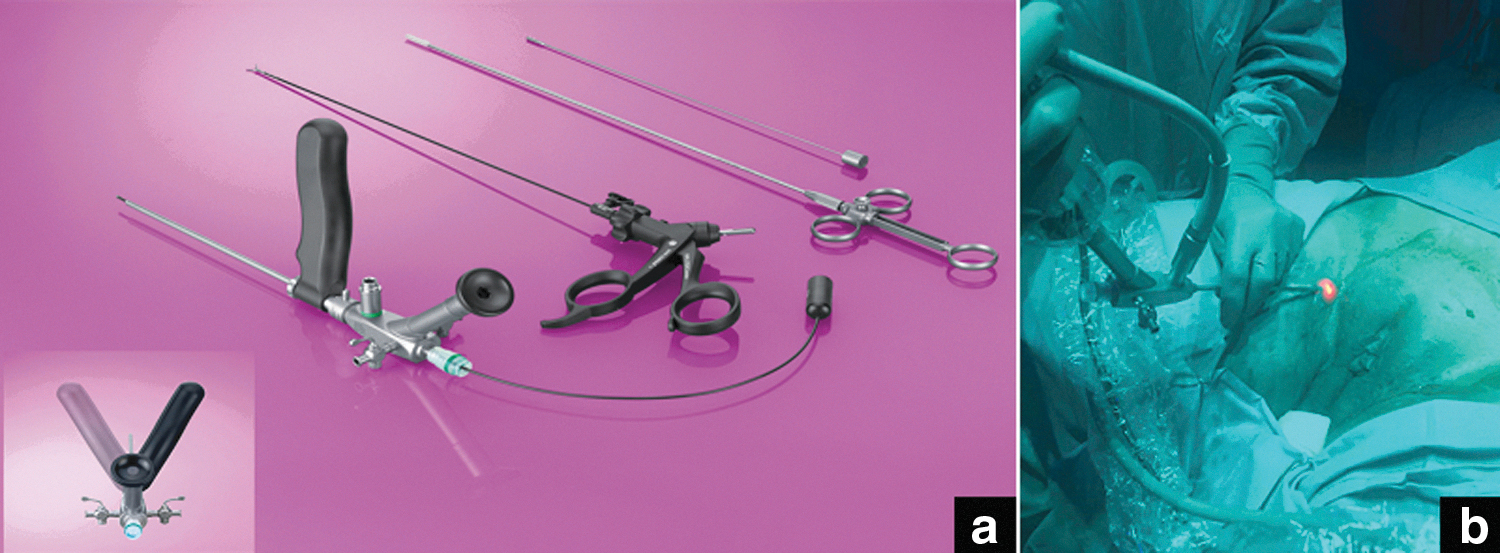
Instrumentation needed for PEHT
During the procedure, the fistuloscope was introduced in the different external holes and a perfect view of the inner aspect of the tracts was allowed by continuous irrigation of sorbitol/mannitol solution. After using an endobrush, all the tracts were cauterized using monopolar electrode or holmium laser energy and finally the residual granulation tissues were removed using grasping forceps. At the end of the procedure, all the holes were filled with oxygen-enriched oil-based gel and covered with fat gauze (Fig. 5).

Final results after surgery
The different steps of the operative technique are reported in Supplementary Video S1.
Postoperative treatment
Full oral intake and early patient mobilization and ambulation were restarted 2–3 hours after surgery. Patients could keep a normal decubitus immediately after surgery. After hospital discharge, the parents were instructed to treat the wound by applying a 2% eosin topical solution, silver sulfadiazine spray, and oxygen-enriched oil-based gel positioned on a wet gauze two times a day for at least 4 weeks postoperatively. All patients returned to their daily activities with no restrictions.
Results
The length of procedure varied between 30 and 80 minutes (average 47 minutes) according to the number of localizations. No intraoperative neither postoperative complications occurred in our series.
All patients scored postoperative pain using the visual analogue pain scale and the average score was 0.7 (range 0–4) during the first 24 hours postoperatively. The average analgesic requirement (paracetamol 15 mg/kg) was 9.8 hours (range 6–20).
All procedures were performed in a day-surgery setting or in few cases with an overnight hospitalization. Parents were instructed about wound management to be performed after hospital discharge by applying a 2% eosin topical solution, silver sulfadiazine spray, and oxygen-enriched oil-based gel positioned on a wet gauze two times a day for at least 4 weeks postoperatively.
The average time to restart work and/or school and daily activities was 1.8 days (range 1–4) and all patients were highly satisfied with the postoperative course, especially for the complete absence of pain postoperatively.
The overall healing rate was 100% and the average time for complete wound healing was 32.5 days (range 30–45) (Figs. 6–8). At the longest follow-up of 1 year, no disease recurrence occurred, but 2 patients (18.2%) developed further lesions in different untreated localizations ∼6 months after the first surgery and were successfully treated using PEHT, with no further recurrence.
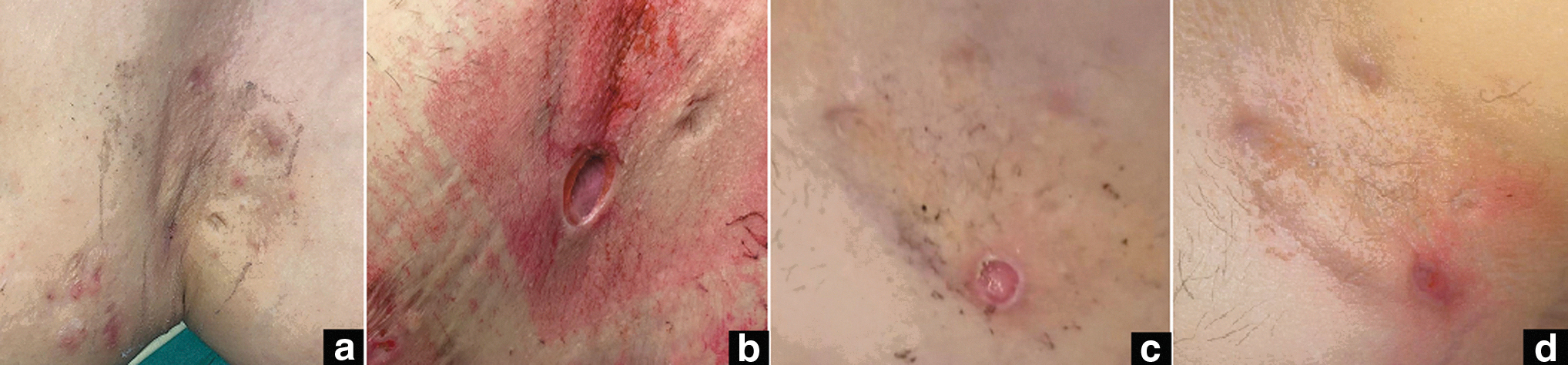
Healing process of axillary HS: preoperative

Healing process of inguinal HS: preoperative

Healing process of inguinal HS: 1 week
Patients' demographics and results are reported in Table 1.
Patients' Demographics and Results
VAS, visual analogue scale.
Discussion
HS is a chronic inflammatory disease that affects the apocrine glands and is characterized by chronic or recurrent nodules that tend to suppuration and rupture with subsequent formation of abscesses, sinus tracts, and scarring.1,2 The lesions are most commonly located at the axillae, inframammary folds, and inguinal and anogenital regions, but can affect other body areas as well. 1 No gold standard treatment protocol supported by robust scientific evidence is currently available.1,15,16 Treatment recommendations for children and adolescents affected by HS are only based on case reports and clinical data extrapolated from the adult population.1,22 Management of these patients should be selected on individual basis according to the location and the extent of the disease.1,15
Conservative therapeutic options range from topical antiseptic agents to general antibiotics, anti-inflammatory drugs, and anti-TNFα agents such as adalimumab and infliximab. Most of these drugs are used off-label, whereas adalimumab is the only drug that has gained until now the FDA approval for treatment of moderate and severe HS.16,22
Several surgical procedures have been described for treatment of HS, such as incisional drainage or wide excisions closed by primary intention using skin grafts or flaps, or left open for secondary intention healing.16,23 Also tissue-sparing methods such as deroofing and skin tissue-saving excision with electrosurgical peeling, lesions' vaporization with carbone-dioxide laser, or Nd:YAG laser have recently been reported even if the real efficacy of these approaches remains unclear.15,24,25 These tissue-sparing techniques reported lower postoperative morbidity and residual scars but higher recurrence rates than wide excision repairs.1,15,18 Analyzing the international literature, the reported recurrence rates are ∼100% after incisional drainage, 42.8% after limited excision, and 27% after wide excisions.1,26
Considering that patients were highly dissatisfied with the results and the painful postoperative course of the standard surgical treatment, we decided to apply for HS treatment the same endoscopic technique that we already adopted in our center to treat pilonidal sinus disease (PEPSiT) and anorectal fistula (Video-assisted Anal Fistula Treatment - [VAAFT]).19–21,27 This technique consists in introducing the fistuloscope through the holes of HS and sterilizing the disease tracts using monopolar coagulation or holmium laser energy after removing the inflammatory tissues using endobrush and graspers. At the end of the procedure, all treated lesions were filled with oxygen-enriched oil-based gel and covered with silver micronized spray and a wet gauze.
The main advantage of this technique is that it is minimally invasive, is a tissue-sparing technique, and above all it is associated with a fast (day surgery or maximum an overnight hospitalization) and painless postoperative course. The postoperative dressings with ozone oil gel and silver sulfadiazine spray guarantee a fast healing of all lesions. Another advantage of this technique is that it can be easily repeated with no contraindication in case of metachronous lesions in untreated locations or in case of disease recurrence in the same area. PEHT does not involve any tissues excisions and sutures; as a consequence, there are no risks of suture dehiscence.
If the external orifices of the tracts are too small for the size of fistuloscope, a technical trick is to enlarge the external holes using urethral dilators or spreading clamps to ease the introduction of the fistuloscope. Another trick is to inject the tract with a syringe filled with saline to enlarge the cavity and remove infected tissues and to have a better view with the fistuloscope.
However, this technique is linked to the technology, because the fistuloscope and the related instrumentation are needed to perform the procedure. In addition, at least two monitors in the operative room are needed because the majority of patients had several localizations in the upper and lower part of the body; in such cases one monitor is placed at the patient's head and another one at the patient's feet to achieve a good vision of all operative fields.
An important aspect that we would underline was the high patients' satisfaction with this procedure, especially for the painless postoperative course, the fast return to full daily activities, and the good cosmetic results. Most patients, who had been already operated with the standard surgical technique, asked to be treated with the endoscopic technique because they considered the standard surgical repair too invasive and painful. Also, the 2 patients already operated on using PEHT, who presented metachronous localizations of the disease, asked to be treated endoscopically due to the painless and fast postoperative period of the previous surgery.
Obviously, we believe that these complex patients should be managed in collaboration with pediatric dermatologists so as to integrate surgery with a concomitant or subsequent medical therapy.
In conclusion, our preliminary experience showed that PEHT can be considered an excellent alternative to traditional surgery in patients with HS. PEHT is a minimally invasive, effective, and safe treatment option for pediatric patients with HS. All patients reported a painless postoperative period and excellent results. We underline the importance of postoperative local dressings using oxygen-enriched oil-based gel and silver sulfadiazine spray to achieve complete healing. However, further evidence with a larger series and longer follow-up is required to confirm these preliminary results.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.