
Abstract
Aim:
To present outcomes of single trocar thoracoscopic surgery in the treatment of pleural empyema (PE) in children.
Patients and Methods:
The thoracoscopic surgery was performed using a single trocar inserted through the fifth intercostal space. A conventional rigid scope with a working channel was used. Pleural fluid was aspirated, followed by debridement and ablation of all septa using one instrument through the working channel.
Results:
Sixty patients from 1 month to 14 years of age underwent surgery without any intraoperative complications or death. The mean operative time was 67 ± 21 minutes. There was no conversion to open thoracotomy. Postoperative complications occurred in 4 patients. Reoperation was required in 1 patient. Mean duration of postoperative hospitalization was 15 ± 9 days. Follow-up was obtained in 57 patients and resulted in normal clinical and chest X-ray findings in all patients.
Conclusion:
Single trocar thoracoscopic operation is safe, feasible, and effective in the treatment of PE in children. A future study with control group is required to draw accurate conclusions.
Introduction
Pleural empyema (PE) is defined as purulent fluid in the pleural cavity. 1 This condition is a common complication of bacterial pneumonia in children. In the United States, the hospitalization rate associated with empyema was 3.7 per 100,000 children during 2006, an increase of 70% in comparison with the rate in 1997. 2 PE is classified into three phases, including the early exudative (Phase I), intermediate fibroproliferative (Phase II), and late organized Phase III. 3 In the exudative stage, thoracocentesis combined with antibiotics is the first-line treatment. 4 For the fibrinopurulent Phase II, closed chest drainage combined with antibiotic and fibrinolytic agents has been performed with good outcomes.5–10
In the past, thoracotomy was the treatment of choice to perform a debridement and decortication when initial noninvasive treatments fail or in organized Stage III.11–13 At present, the minimally invasive video-assisted thoracoscopic surgery has become the gold standard in the management of PE in late stages.14–21 However, there have been no publications reporting single trocar thoracoscopic surgery using a rigid scope with a working channel in the management of PE. Since January 2013, this technique has been used at the National Children's Hospital of Vietnam for the treatment of PE.
The aim of this report is to present our thoracoscopic technique using single trocar and a rigid scope with a working channel (Fig. 1) and to evaluate its safety, feasibility, and effectiveness in the management of PE in children.

Rigid scope with a working channel.
Patients and Methods
Inclusion and exclusion criteria
Patients ≤15 years of age with PE due to community-acquired pneumonia were included in this study. The diagnosis of empyema was confirmed by chest X-ray plus ultrasound and then further verified by intraoperative findings.
Exclusion criteria were an existing contraindication to thoracoscopy, necrotizing pneumonia, and pneumonia due to nosocomial infection.
The following data parameters were collected: patients' demographic data, duration from the onset of symptoms to the surgery, chest ultrasound findings, chest X-ray findings, chest computed tomography (CT) findings, operating time, rate of conversion to thoracotomy, perioperative complications or death, duration of thoracic drainage, duration of postoperative fever, duration of postoperative hospitalization, and follow-up results.
Interventions
The patient underwent general anesthesia and was then placed in the lateral decubitus position on the opposite side of the empyema. An 11-mm skin incision was carried out on the fifth intercostal space. Muscles were separated, and dissecting forceps were introduced into the pleural cavity, followed by insertion of a 10 mm trocar. A 10 mm scope with a working channel (Stema autoclave) was used. A carbon dioxide pneumothorax (4–6 mm Hg CO2) was maintained to collapse the lung. Pleural fluid was aspirated followed by extensive debridement and ablation of all septa, and pleural peel was performed using one instrument inserted through the working channel (Fig. 2) to allow the whole pleural cavity to be unified and the lung to be expanded (Fig. 3). A chest tube was placed through the trocar incision.

Extensive debridement and ablation of all septa.

Pleural cavity was unified and lung was expanded.
Ethics
Before the intervention, a careful explanation of the risks and benefits of the operation was given to parents. Written consent was obtained in all cases. The study protocol was approved by the Hospital Board.
Results
From January 2013 to December 2014, 60 patients, including 30 boys and 30 girls were enrolled in this study. The youngest patient was 1-month-old and the oldest patient was 14 years old. Twenty-two patients were less than 12 months and 38 patients were older than 12 months. Patient weight varied from 4.7 to 52 kg (median: 10 kg).
All patients received antibiotics and two of them underwent chest tube drainage before admission to the National Children Hospital.
Empyema was located on the right side in 31 patients (51.7%) and the left side in 29 patients (48.3%), assessed by chest X-ray. On chest ultrasound, pleural septa were found in 48 patients (80%) and dense fluids were observed in 12 patients (20%). Pleural septations were observed in all 37 patients who had a chest CT. Pleural septa, pus, and pleural peel were found in all patients upon thoracoscopy. Cultures from pleural fluids were negative in 50 patients, while among 10 positive cultures, the most frequent bacterium was Staphylococcus aureus, followed by Streptococcus pneumonia.
Mean operative time was 67 ± 21 minutes (ranged: minimum 40 minutes to maximum 135 minutes). Conversion to open thoracotomy or additional trocar was not required in any patient. There were no intraoperative complications. No adverse events or deaths occurred either intraoperatively or postoperatively. Postoperative complications occurred in 4 patients, including pneumothorax in 3 patients, and subcutaneous emphysema in 1 patient. Reoperation was required in 1 patient due to obstruction of chest drainage.
Durations for postoperative chest drainage, fever, and hospitalization are shown in Table 1.
Duration of Postoperative Chest Drainage, Fever, and Hospitalization
There were significant differences for operating time, duration of postoperative fever, duration of postoperative chest drainage, and postoperative hospitalization between patients who underwent surgery before 2 weeks from the onset and those later than 2 weeks from the onset (Table 2).
Outcomes According to Duration from the Onset to Operation
In contrast to the duration from the onset to surgery, the results did not significantly differ between children <12 months old and those ≥12 months (Table 3).
Outcomes According to Patient's Age
Follow-up exams occurred from 1 to 27 months (median: 12.9 months) and relevant data were obtained from 57 patients (95%). Normal clinical and chest X-ray manifestations were observed in all patients (Fig. 4) at the time of their respective follow-ups.
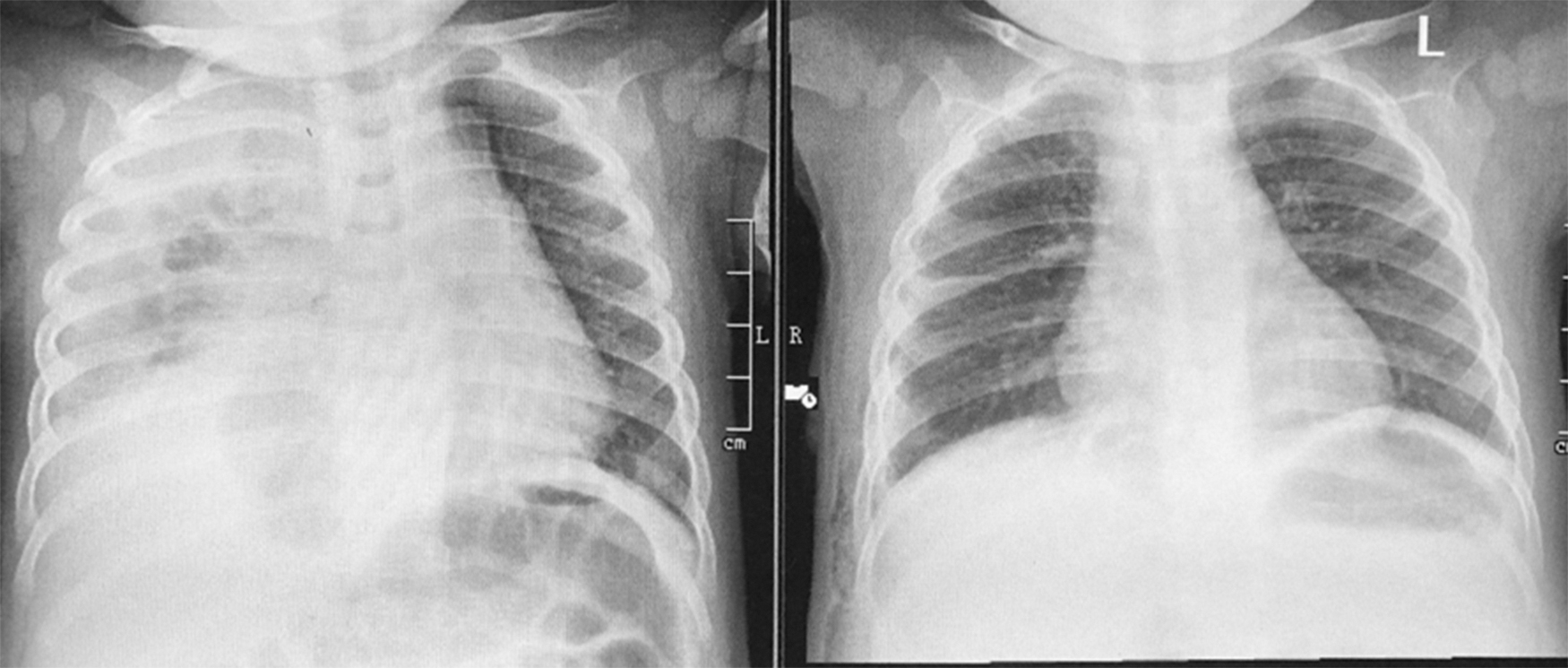
Chest X-ray before and after operation.
Discussion
To our knowledge, this is the first report on patients suffering from PE who underwent thoracoscopic surgery using single trocar with a rigid scope to manage advanced empyema in children. Our results demonstrated that this approach is feasible. The operations were completed in all patients successfully. Conversion to open surgery or additional trocar was not required in any patient. Evacuation of pus, removal of all fibrous tissue from the pleura, ablation of all septa, and removal of pleural peels were accomplished with a single instrument through a working channel. The lung was well expanded at the end of the surgery in all patients.
The operating time in our study was relatively short (67 ± 21 minutes) and significantly shorter compared with other studies using three trocars (Table 4).
Comparisons of Outcomes Between Different Series
No information.
The results demonstrated that the approach is safe. There were no intraoperative complications or deaths. The rate of postoperative complications was low. Four patients (6.6%) had postoperative complications and one among them required a second operation due to obstruction of the thoracic drain. The rate of postoperative complications in our series was lower than that of reported series where the operation was carried out using three trocars.20–25
Our results favor an early intervention in PE. Operating time, complication rate, duration of fever after the operation, and duration of chest tube drain in patients who were operated within 2 weeks from the onset were shorter than in patients operated after 2 weeks (Table 2). Other studies also demonstrated that earlier intervention is associated with better outcomes for PE.8,24–27 However, the definition of early thoracoscopic surgery has not yet been clearly defined. A 4-day limit was proposed by Kalfa et al., whereas a 2-day limit was recommended by Schultz et al.23,27
Our results revealed that there are no differences in operating time, complication rate, duration of fever after the operation, or duration of chest tube between patients who were <12 months old and patients ≥12 months old. This finding demonstrated that single trocar thoracoscopic surgery can be carried out safely and effectively for children regardless of age.
Normal clinical and radiologic manifestations were obtained for all patients with a mean follow-up time of 12.9 months, demonstrating that single trocar thoracoscopic surgery provided not only good early outcomes but also satisfactory results in a subsequent follow-up.
From our results, we can conclude that single trocar thoracoscopic surgery with a rigid scope is safe, feasible, and effective in the management of PE in children. However, a future study with the control group is necessary to draw accurate conclusions.
Footnotes
Acknowledgment
The authors would like to express their gratitude to Dr. Michael Heke, Department of Biology, Stanford University, USA, for editing the English version.
Disclosure Statement
No competing financial interests exist.
Funding Information
The author(s) received no specific funding for this work.