
Abstract
Background:
This study represents a prospective analysis of a series of laparoscopic ultra low anterior resection (ULAR) done at a laparoscopic surgical center to assess the surgical outcome, oncological efficacy, and quality of life after surgery.
Methods:
Over a period of 6 years (2013–2018), 43 patients aged between 40 and 68 years, with very low rectal cancers (3–6 cm from the anal verge), within T3N1M0 stage, assessed by positron emission tomography–computed tomography and pelvic magnetic resonance imaging, underwent neoadjuvant chemoradiotherapy (nCRT) followed by laparoscopic ULAR and simultaneous diversion ileostomy.
Results:
The overall complication rate was low and there was an overall leak rate of 9.3% with a radiological leak (Grade A) in 3 of the 43 patients (7%), but only 1 (2.3%) patient required a local lavage and a resuturing for secondary hemorrhage. Recurrence was seen in 2/43 (4.7%), one of whom had a conversion to abdominoperineal resection. The other had distant metastasis and refused further treatment. The functional outcome is assessed in 41 (95.3%) patients by low anterior resection syndrome (LARS) score and a reasonable quality of life with major LARS was seen in only 7.3% of the patients at a follow-up ranging from 1 to 6 years.
Conclusion:
The nCRT followed by laparoscopic ULAR is a feasible option for operable very low rectal cancers and is associated with minimal postoperative events, a low local recurrence and less incidence of LARS.
Introduction
Colorectal cancer (CRC) is the fifth most prevalent cancer in India with a low 5-year survival rate owing to late detection of cancer. CRC is the third most common cancer and the fourth leading cause of deaths due to cancers all over the world.1,2 In India and the developing countries, CRC is becoming prevalent in low and middle income group population and signals the need for aggressive screening programs that should be integrated into the existing health care system. 3 Since the advent of minimally invasive surgery, rectal cancer has been increasingly dealt with laparoscopically.
The ultra low anterior resection (ULAR) has been defined varyingly, as when the anastomosis is within 2–5 cm from the anal verge. For this study, low rectal tumors 3 to 6 cm from the anal verge were selected. The common concerns with these operations are a high leak rate, local recurrence, and the low anterior resection syndrome (LARS)4–6 that encompasses a variety of symptoms including increased gas, urgency, frequency, stool fragmentation, and gas and stool incontinence after low anterior resection or ultra low anterior sphincter preserving surgeries. Laparoscopic approach to colorectal cancer has permitted excellent visualization of pelvic structures, and a complete total mesorectal excision (TME) is made easier, without compromising circumferential resection margins using circular stapler. But if the anastomosis is close to the dentate line, then the pull through of the colon, with a hand sewn coloanal anastomosis, is the ideal choice.
To preserve continence, when the colon is pulled through for a coloanal anastomosis, a major concern is whether compromise of the distal line of resection would increase local recurrence postoperatively. Another major issue is the increased frequency of defecation because of loss of reservoir function of the rectum. In this study, the incidence of leak, recurrence rate, and LARS were the important end points in the follow-up of patients undergone ULAR. Thus, surgical feasibility, oncological efficacy, and the functional outcome (quality of life) after ULAR were assessed in this study.
Materials and Methods
Based on the positron emission tomography–computed tomography (PET-CT) and pelvic magnetic resonance imaging (MRI), very low rectal cancers situated 3–6 cm from the anal verge, with a grading up to T3N1M0 patients were taken up for the study. We did not do endorectal ultrasound, which may be an inferior tool to assess early rectal cancer. 7 Forty-three patients underwent totally laparoscopic ULAR over a 6-year period, between 2013 and 2018. The age range was 40–68 years with 25 men and 18 women. All patients had surgery after neoadjuvant chemoradiotherapy (nCRT) consisting of 25 fractions of external radiotherapy and chemotherapy based on capecitabine and oxaliplatin concomitantly. All 43 patients had a diversion ileostomy along with the ULAR, and the stomas were closed at varying periods, from 12 weeks up to 12 months. All patients were followed up with telephonic interview about the questionnaire of LARS scoring 4 at frequent intervals and at the end of 1 year of surgery.
Results
A perioperative data were available for all 43 patients (Table 1). There was no mortality and the radiological leak (Grade A) rate was 7% and the clinical leak (Grade C) rate was 2.3% with an overall leak rate of 9.3%. Major complications were seen in none of these patients. Return to the operating room was in 1 patient for securing hemostasis who had secondary hemorrhage at the suture line. Two out of 43 patients (4.7%) had a local recurrence. An abdominoperineal resection (APR) was performed in 1 of the patients. The other patient presented with combined local and metastatic disease, and opted out of all treatment. A total of 41 patients were followed up in frequent intervals and at the end of 1 year by a telephonic questionnaire about LARS scoring. Sixteen per 41 patients (39%) had no LARS, 22/41 (53.7%) had minor LARS, and 3/41 (7.3%) had major LARS. Stoma closure was done in 12–24 weeks in 26/41 patients (63.4%), in 24–32 weeks in 10 patients (24.4%), 32–40 weeks in 4 patients (9.8%), and at 1 year (52 weeks) in 1 patient (2.4%). The last patient had the leak that required washout in the operating room, and the secondary bleed requiring resuturing, and had persistent perirectal sepsis that settled after 3 months. One patient had bloody mucus and pain, and colonoscopy showed features of ischemic colitis of the mobilized descending colon that settled spontaneously with conservative management.
Results After Ultra Low Anterior Resection
LARS, low anterior resection syndrome.
Discussion
The baton in colorectal surgery has been successfully passed from Miles, 8 Goligher et al., 9 Lyttle and Parks, 10 Parks and Percy, 11 Heald, 12 Schiessel et al., 13 and Rullier et al. 14 The standardization of ULAR or the sphincter preserving surgery by Rullier et al. 15 narrowed down the indications for APR, a fitting tribute to Miles. 8 The ULAR is a low anterior resection that entails an anastomosis that is 3 cm or less from the dentate line. It involves extensive mobilization of the transverse colon and the splenic flexure, TME, partial excision of internal sphincter, resection of specimen, and a hand sewn or circular stapler anastomosis. We routinely adopt nCRT comprising of 25 fractions of external radiotherapy (total = 50 Gy) and a concomitant chemotherapy based on capecitabine and oxaliplatin in view of the established value of nCRT.16,17 Six weeks18–21 after nCRT, PET-CT and pelvic MRI are done, before taking up for sphincter saving ULAR with a distal margin of 1 cm that is oncologically sound and acceptable.22,23 The role of endorectal ultrasound is limited in early rectal cancers 7 and hence MRI is preferred for staging and follow-up.
Technique
Our preoperative bowel preparation entails the administration of oral antibiotics and polyethylene glycol based mechanical bowel lavage that may potentially alleviate surgical site infections in elective colorectal surgery. 24 The patient is given oral neomycin 1 gm tid and tinidazole 500 mg bid the day before surgery. Our patients take 50 gm (400 mL) of complex carbohydrate (maltodextrin 12.5%) drink 3 hours before the surgery that pre-empts metabolic response to surgery and thus helps to maintain whole body protein balance and improves insulin sensitivity perioperatively.25,26 Since there is an embryonic fusion between endoderm and ectoderm in the anorectal region, the idea is to remove the diseased rectum without disturbing the external anal sphincter. 10 The operative strategy in our institute involves a five port approach consisting of a 10 mm supra umbilical port, a 10 mm right midclavicular line port, a 12 mm right iliac fossa port, a 5 mm port along the left midclavicular line at the level of the umbilicus, and a 10 mm epigastric port. The procedure involves diagnostic laparoscopy to rule out metastasis and clipping of the inferior mesenteric artery after the first proximal branch to preserve the blood supply to the marginal artery via the left colic artery. Splenic flexure and the distal half of the transverse colon are mobilized by releasing the gastrocolic ligament and complete paracolic mobilization of the left colon is done after identification and preservation of the ureters. TME is performed by entering into the holy plane of Heald. 12 Complete rectal mobilization (Fig. 1) is done in this avascular plane after releasing the lateral ligaments on both sides while preserving the pelvic plexuses. The dissection is continued anteriorly to develop a plane between the anterior wall of the rectum and the apex of the prostate gland in men and the posterior wall of vagina in women, that is, upper part of external sphincter and puborectalis muscle posteriorly. The dissection is continued with the circumferential mobilization of the rectum up to the pelvic floor as low as possible to facilitate perineal dissection. The perineal dissection is commenced by putting purse string sutures transanally (Fig. 2), which helps to bring down the anastomotic line as close as to the anal verge and a circumferential incision of mucosa and the internal sphincter, 1–2 cm below the lower edge of tumor, and continued cranially in the intersphincteric bloodless plane in a circumferential manner, until the proximal dissection is encountered. The tumor-bearing segment is removed transanally (Figs. 3 and 4) followed by pull through of the proximal segment down into the anal verge and a single layered coloanal anastomosis using 3-0 poly dioxanone interrupted sutures, starting with the 12, 3, 6, and 9 O'clock positions, and then putting the sutures in the quarter segments in between. In some select cases, the surgery is performed using circular stapler where the anastomosis is 3 cm from the dentate line.27,28 The procedure is completed with a drain in the pelvis and a diversion ileostomy in the right iliac fossa. Thus, the entire abdominal dissection is done laparoscopically that is inclusive of TME (Fig. 5) and that is the key to prevent local recurrences. 29 The perineal part of dissection is done with the partial excision of internal sphincter and complete preservation of external sphincter thus reducing the LARS significantly.
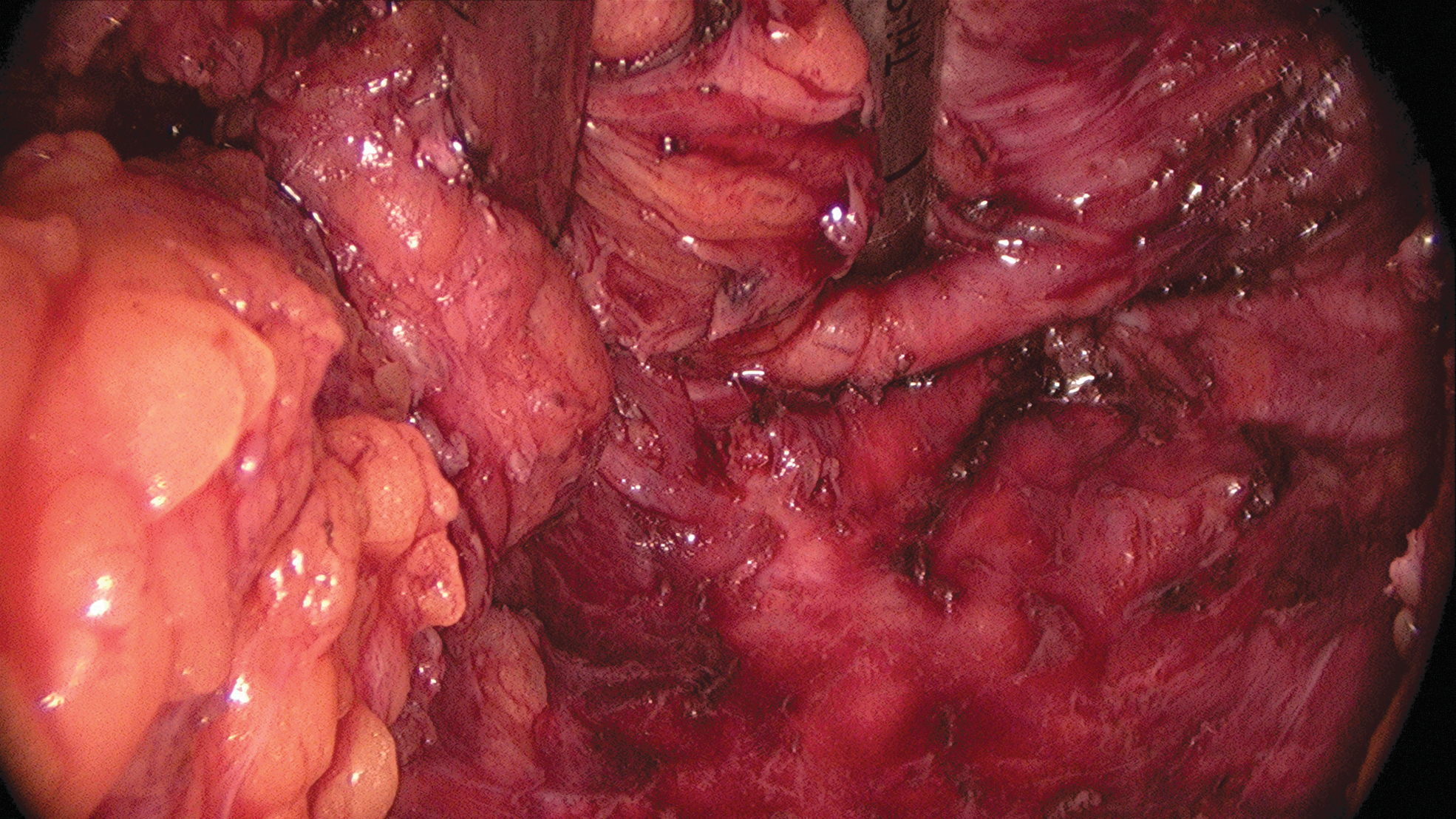
Intraoperative total mesorectal excision.

Perianal purse string sutures.
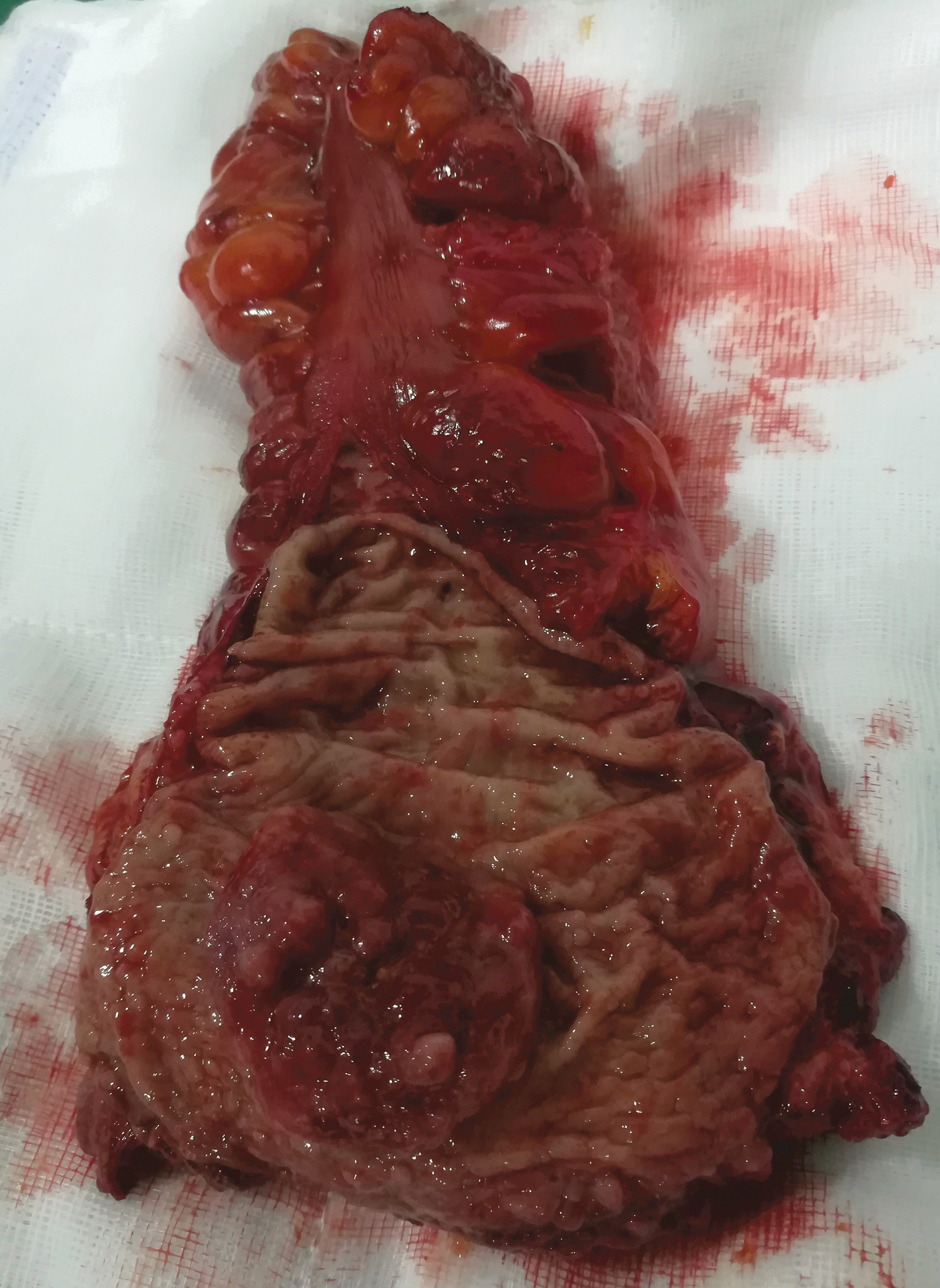
Specimen with 1 cm distal margin.

Transanal extraction of specimen.

Total mesorectal excision with the specimen.
Anastomotic leak
The International Study Group of Rectal Cancer proposed a definition and grading system (Table 2) for anastomotic leaks (ALs).30,31 Although the radiological leak rate (Grade A) in our series was 7%, only 1 patient actually required return to the theater for a local lavage without need for a relaparotomy, denoting a clinically significant (Grade C) leak rate of 2.3% with an overall leak rate of 9.3%. In a a systematic review of 930 articles, done by Cong et al., 32 the pooled rate of leak requiring another abdominal exploration was actually lowest in ULAR (1.81%) compare to anterior resection and low anterior resection, at 5.4% and 4.7%, respectively. The value of the proximal diversion was emphasized in this seminal article. Another pivotal article studying ALs by Damen et al., considered 2944 anastomoses with a leak in 82 patients. 33 A multivariate analysis showed that ischemia and radiation were independent predictors of a leak, apart from surgical experience. The AL rates of various authors have been compiled here (Table 3).23,32–43 In most of the available articles in literature, the patients undergoing rectal resections are a heterogeneous sample if radiotherapy is taken into account. In this series, it is notable that every single patient had nCRT and that too, of the 25 days course and not the 5 days course. It is also worth pointing out that only 64.3% of the ULARs had diversionary stomas in the Australian series, vis-a-vis 100% in our series. The functioning stoma could certainly mitigate the septic complications of a possible AL, with a definite recommendation for the same in ULAR. 44 Valvular heart disease, renal failure, and packed cell transfusion adversely influence AL and mortality. 45
International Study Group of Rectal Cancer Definition of Anastomotic Leak Grades
Anastomotic Leak Rates After Ultra Low Anterior Resection
AL, anastomotic leak.
Closure of stoma
Regarding the closure of the diversion stoma, there has been a recent advocacy for early closure of the stoma, that is, 2–6 weeks after surgery. But ALs and preoperative radiotherapy were found to negatively impact early stoma closure. 46 In our series, every patient had radiation before surgery and hence the closure of the stoma was planned only after 2 months. Second, 4 of our patients had leaks, although they were clinically significant only in 1 case. Moreover, the one AL patient also had secondary hemorrhage at the anastomotic line that required reoperation and this patient was found to be fit to close the stoma only after 1 year.
Local recurrence
In this series of 43 patients, 2 patients presented with local recurrence (4.7%), and an APR was performed in 1 patient. At follow-up, 24 months after surgery, with adjuvant chemoradiation, he remains disease free on PET-CT scan. The other was found to have widespread metastatic disease and refused all forms of treatment. Several studies have confirmed that the survival is significantly increased after surgical resection is completed for local recurrence (Table 4).23,36,38–40,42,47–55 In terms of local recurrence after ULARs, Yun et al., 56 doing a retrospective review of 2485 patients, reported a local recurrence in 147 patients (5.9%). The nCRT significantly reduces local recurrence and improves overall survival as did the tumor location and proximity to the anal verge.16,17 Some feel that local recurrences are much lesser in ULAR than APR. 57
Local Recurrence Rate After Ultra Low Anterior Resection
Low anterior resection syndrome
Despite a sphincter sparing rectal resection, a proportion of patients suffer from fecal urgency or incontinence, fragmented motions, or evacuating difficulties, the constellation of which is referred to as LARS. 4 There are so many scoring scales to assess the fecal incontinence/LARS.4,58–61 We adopted LARS score by Emmertsen and Laurberg 4 (Table 5) that is simple and effective. In this series of 41 patients that we evaluated by a telephonic LARS scoring questionnaire, 16/41 patients (39%) had no LARS, 22/41 (53.7%) had minor LARS, and 3/41 (7.3%) had major LARS. And we have seen the improvement in LARS scoring over the years. These results are acceptable in terms of good quality of life. However, these patients did not seem to particularly mind this, and it is possible that the survival from the rectal cancer and the avoidance of the stoma outweighed, perceptually, the need to frequently visit the toilet! However, anorectal manometric studies were not obtainable in these patients at this point of time. The etiopathogenesis of LARS is complex and multifactorial ranging from neoadjuvant chemoradiation, external anal sphincter complex disruption during anastomosis construction, alterations in anorectal reservoir physiology, development of a pudendal neuropathy, and sepsis caused by AL. 62 The 25 patients in the series (61%) of patients with LARS were enrolled in LARS comprehensive treatment algorithm inclusive of pelvic floor muscle training, oral 5-HT3 receptor antagonists, biofeedback training, and rectal balloon training.62–64 Some authors point out the higher incidence of LARS in sphincter preserving surgeries (Table 6).65–73 Preoperative counseling should include the functional outcome of the surgery in detail. In terms of sexual pleasure, ULAR outscored APR. 74 Various authors have established that lower rectal cancers can be cured with sphincter preserving ULAR with a better quality of life.75–80 The prospective multicenter, phase 2 trial designed by the American College of Surgeons Oncology Group 81 has proven the feasibility of using nCRT and local excision in very low rectal cancers thus vindicating our stand.
Low Anterior Resection Syndrome Score
Adopted LARS score by Emmertsen and Laurberg. 4
Low Anterior Resection Syndrome Score After Ultra Low Anterior Resection
Conclusion
In this prospective analysis of 43 patients 41 undergone laparoscopic ULAR at a single center, there was no immediate postoperative mortality, a clinical leak rate of 2.3%, an acceptable degree of LARS, and reasonable oncological outcome. The stoma free quality of life on follow-up for 1–6 years was reasonable. Although major LARS was found in 7.3% of the patients initially, it tended to decrease over the years. The nCRT and laparoscopic ULAR with diversion ileostomy that entails laparoscopic TME with partial excision of internal sphincter and complete preservation of external anal sphincter is oncologically sound and a viable alternative for patients with operable very low rectal cancers, historically managed by APR.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.