
Abstract
Background:
As minimally invasive pediatric surgery becomes standard approach to many surgical solutions, access has become an important point for improvement. Laparoscopic cholecystectomy (LC) is the gold standard for many conditions affecting the gallbladder; however, open cholecystectomy (OC) is offered as the initial approach in a surprisingly high percentage of cases.
Materials and Methods:
The Kids' Inpatient Database (1997–2012) was searched for International Classification of Disease, 9th revision, Clinical Modification procedure code (51.2x). LC and OC performed in patients <20 years old were identified. Propensity score-matched analyses using 39 variables were performed to isolate the effects of race, income group, location, gender, payer status, and hospital size on the percentage of LCs and OCs offered. Cases were weighted to provide national estimates.
Results:
A total of 78,578 cases were identified, comprising LC (88.1%) and OC (11.9%). Girls were 1.6 (CI: 1.4, 1.7) times more likely to undergo LC versus boys. Large facilities were 1.4 (1.3, 1.7) times more likely to perform LCs than small facilities. Children in lower income quartiles were 1.2 (1.1, 1.3) times more likely to undergo LC compared with those in higher income quartiles. Rates of LC were not affected by race, hospital location, or payer status.
Conclusions:
Risk-adjusted analysis of a large population-based data set demonstrated evidence that confirms, but also refutes, traditional disparities to minimally invasive surgery access. Despite laparoscopic gold standard, OC remains the initial approach in a surprisingly high percentage of pediatric cases independent of demographics or socioeconomic status. Additional research is required to identify factors affecting the distribution of LC and OC within the pediatric population.
Introduction
Since the advent of minimally invasive surgery, laparoscopic cholecystectomy (LC) has become the standard of care for the majority of gallbladder disease. The first LC in North America was performed in 1989 and it rapidly evolved into standard practice—by 1992, >80% of cholecystectomies being performed laparoscopically. 1 In today's adult population, >95% of cholecystectomies are approached laparoscopically. 2
Pediatric surgery was slower to adopt minimally invasive approaches. The first LC in a child was performed in 1991. 3 Subsequently, several reviews proclaimed that laparoscopic cholecystectomies were safe and effective in the pediatric population.4–6 Nevertheless, practice patterns lagged behind, as the incidence of laparoscopic cholecystectomies plateaued in 2006. 1 At the time, reasons suggested for slower adoption included pediatric size, physiology, rarity of disease, lack of training, and the steep learning curve. 1 Even today, despite widespread acceptance that laparoscopy is the gold standard for cholecystectomy, open cholecystectomy (OC) is offered as the initial approach more frequently than in the adult population.
We used a large retrospective database to compare the incidence of laparoscopic versus open cholecystectomies in the pediatric population, and investigated disparities associated with each approach.
Materials and Methods
The Kids' Inpatient Database is a population-based data set sponsored by the US Agency for Healthcare Research and Quality. We used the years 1997–2012, available in triennial releases, to construct our study data set. Each release provides data on up to 7.5 million weighted cases. The data points are standardized and cleaned before each release. Quality is ensured using the guidelines set forth by the Healthcare Cost and Utilization Project (HCUP). Diagnoses and procedures are coded using the International Classification of Disease, 9th revision, Clinical Modification (ICD-9-CM).
We identified cases of cholecystectomy using ICD-9-CM code 51.2x. Cases of LC and OC for patients <20 years were included in the data set. Patients who were coded as “transfer to short-term hospital” and “other transfers, including skilled nursing facility, intermediate care, and other type of facility” were excluded to avoid duplicate reporting. All cost values were derived from the cost-to-charge ratio values provided by the HCUP and dollar amounts were standardized to 2012 USD, according to inflation rates provided by the US Bureau of Labor Statistics. Cases were weighted to provide national estimates.
Individual propensity score (PS)-matched analyses were used to demonstrate differences in the use of LC versus OC given similar circumstances (clinical, demographic, and hospital characteristics), with the exception of the socioeconomic variable under examination. We performed additional risk adjustment using a standard set of Elixhauser comorbidities, which includes fluid and electrolyte disorders, coagulopathy, and other comorbid conditions. A total of 39 variables were included. We completed additional PS-matched analyses for additional socioeconomic variables to determine whether disparities exist, given that LC is the standard approach in modern health care.
MatchIt, version 2.4-20 (Cambridge, MA), a supplemental module for R, version 2.14.2 (R foundation for Statistical Computing, Vienna, Austria), was used for PS value assignment, case sorting, and matching. Statistical analyses were performed using SPSS Statistics, version 21 (2012, IBM, Armonk, NY). This retrospective study was deemed to be exempt from full review by the Institutional Review Board at the University of Miami Miller School of Medicine (Miami, FL).
Results
Overall, 78,578 cases of cholecystectomy were identified within the data set. The majority (88.1%) were performed using laparoscopy as the initial approach. Laparoscopy as the initial approach has increased over time (Fig. 1). Demographic, socioeconomic, and hospital variables are presented in in Table 1. As demonstrated by the baseline comparisons using chi-square analyses, the variable distribution differed significantly between those undergoing laparoscopic and OC as initial approach.
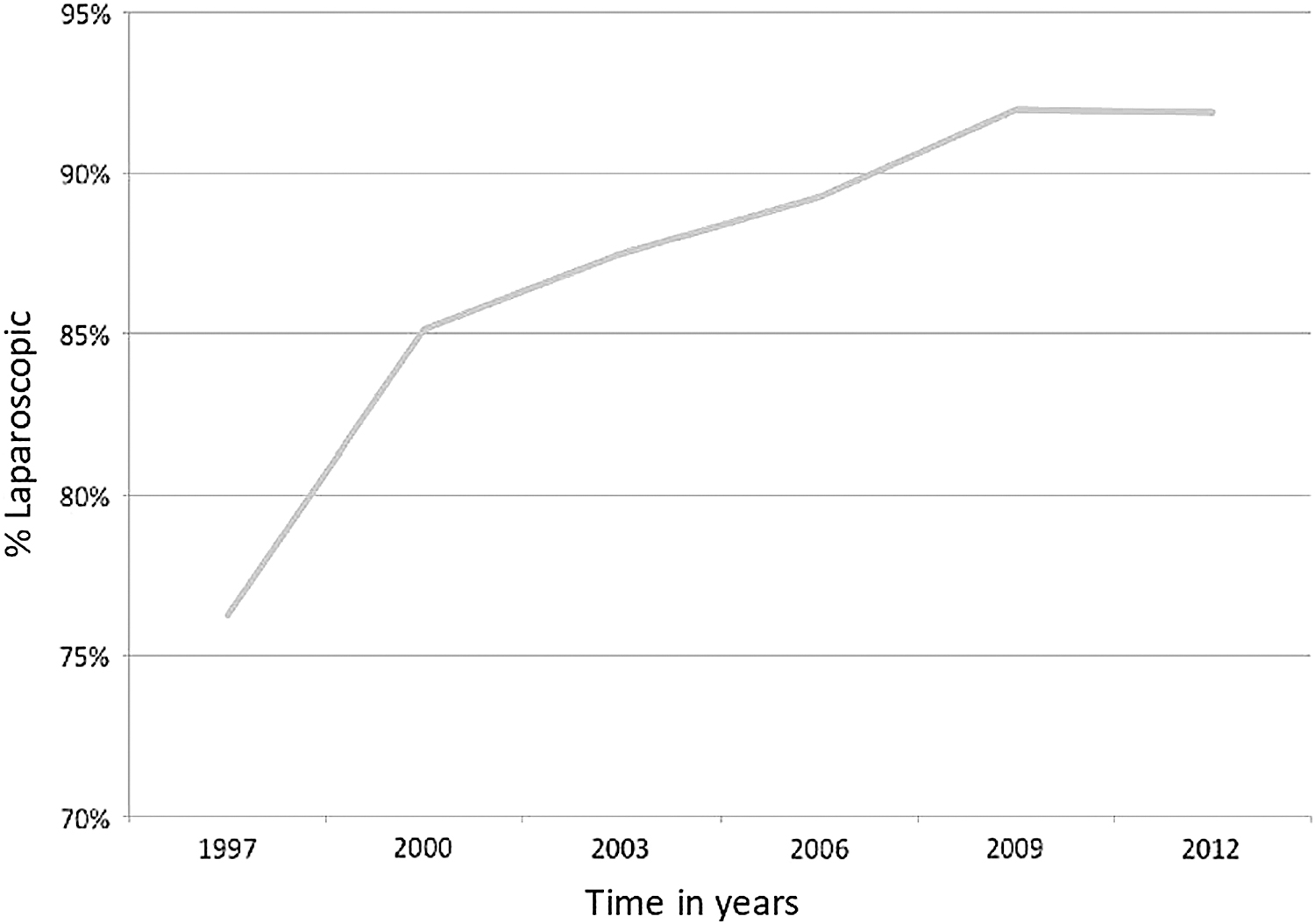
Proportion of cholecystectomy being performed using an initial laparoscopic approach, 1997–2012. Kids' Inpatient Database.
Demographic, Socioeconomic, and Hospital Characteristics of Study Cohort, 1997–2012
Kids' Inpatient Database. Baseline chi-square comparisons are made between laparoscopic and open initial approaches.
Indications documented as associated diagnosis codes are not mutually exclusive.
Six categories were chosen for PS-matched analyses: gender, race, median income quartile, payer status, hospital location, and hospital bed size.
Overall cohort
Boys had a higher rate of OC (odds ratio [95% confidence interval]: 1.57 [1.43, 1.72]) versus girls, P < .001. Patients from higher income quartiles had higher rates of open approach (1.17 [1.09, 1.25]) versus lower income quartiles, P < .001. Procedures performed in smaller facilities also had a similar trend (1.45 [1.27, 1.64]) versus larger facilities, P < .001. For a graphical representation (Fig. 2). Race, hospital location, and payer status had no effect with regard to the initial approach.

Odds of OC as initial approach, compared with LC as initial approach, 1997–2012. Kids' Inpatient Database. LC, laparoscopic cholecystectomy; OC, open cholecystectomy.
Subanalysis: <12 years of age
Rural hospitals were more likely to perform laparoscopic cholecystectomies (2.57 [1.29, 5.14]) versus urban hospitals, P = .0067. Boys had a higher rate of OC (1.25 [1.08, 1.44]) versus girls, P = .0027. Insured patients were more likely to undergo laparoscopic cholecystectomies (2.71 [1.29, 5.73]) versus self-pay patients, P = .0081.
Subanalysis: 12–18 years of age
Lower income quartiles had higher rates of OC (1.12 [1.02, 1.24]) versus higher income quartiles, P = .0210. Boys had higher rates of OC (1.94 [1.67, 2.25]) versus girls, P < .0001. Small facilities were more likely to perform open cholecystectomies (1.42 [1.19, 1.71]) versus larger facilities, P < .0001.
Subanalysis: ≥18 years of age
Lower income quartiles had higher rates of LC (1.21 [1.01, 1.46]) versus higher income quartiles, P = .0423. Boys were more likely to undergo OC (3.58 [2.50, 5.13]) versus girls, P < .0001. Insured patients were more likely to undergo OC (1.53 [1.13, 2.07]) versus self-pay patients, P = .0061.
Discussion
LC is the gold standard of care for most gallbladder disease in the pediatric population. This has been a consensus since the operation was both safe and effective in the pediatric population back in 1991.1,3–6 Compared with OC, LC boasts improved cosmesis, lower postoperative pain scores, decreased analgesia requirements, a lower incidence of ileus, shorter length of stay, and faster return to normal activity.6–10 Although LC has an aggregate higher operative cost, overall hospital cost is significantly lower due to the diminished length of stay.7–9 Most LC complications are minor, such as cystic duct leak, gallbladder perforation, dropped stones, and trocar incision site infections. 11 The most significant complication, common bile duct injury (CBDI), was reported to occur in 0.36%–0.44% of patients, higher than the OC incidence of 0.1%.7,11–13 A recent analysis of a statewide registry demonstrated that the incidence of CBDI appears to be approaching the same as that in OC. 14
Despite LC's obvious benefits and low risks, surgeons are still performing OC as their initial approach in >10% of pediatric cases. In our study, 12% of the cholecystectomies were performed through an initial open approach, a percentage similar to Kelley-Quon et al.'s 7%–12%. 15 In the adult population, <5% of cholecystectomies are performed open as the initial approach. 2 Moreover, our study also demonstrates that an initial laparoscopic approach increased before plateauing in the mid to late 2000s. This finding echoed previous research, as well. 1
Generally, pediatric surgeons have been slower to adopt minimally invasive surgical methods. Reasons are multifactorial and may include a lack of training, less comfort level of either surgeon or anesthesiologist, and surgeon attitudes toward minimally invasive approaches. 16 In comparison with the adult general surgeon, pediatric surgeons perform fewer cholecystectomies per year, due to the relative rarity of gallbladder disease in the pediatric population.1,17 Surgeons with lower volumes of laparoscopic cholecystectomies have longer operating times and more complications. 17
We performed propensity matching to determine which variables were associated with an initial open approach cholecystectomy. This is the first disparities study examining cholecystectomies in the pediatrics population. Males and smaller volume facilities had higher incidence of undergoing an OC. The association between males and open cholecystectomies was previously observed in the adult population.17,18 As a limitation of this database study, we can only speculate that there were clinical variables responsible for this but not accurately identify them. We also cannot differentiate between adult and pediatric surgeons and their operative practice regarding cholecystectomies in children. The association of OC with smaller facilities may be explained by lower operative volumes. Interestingly, patients in the highest income quartile were associated with OC, as well. This observation runs counter to what might be expected and requires additional inquiry.
Two additional findings were noteworthy. First, there was no difference between urban and rural hospitals in surgical approach—reflecting multiple adult studies that have demonstrated that hospital setting does not affect the safety, efficacy, and feasibility of the laparoscopic choleycstectomy.18–20 Second, our results identified no differences in surgical approach between white and nonwhites. Studies in the adult population have demonstrated conflicting findings on the subject.17,21
We have found evidence that confirms, but also refutes, previous assumptions regarding disparities for laparoscopic cholecystectomies. Once an infrequent pediatric operation, cholecystectomies are becoming more commonplace. Hemolytic diseases and biliary dyskinesia are now indications for cholecystectomy, and the epidemic of childhood obesity has dramatically accelerated the incidence of surgical disease.22–26 Therefore, it is imperative that we identify disparities regarding access to minimally invasive surgery.
Our study has limitations. It is a database study with the inherent weaknesses of retrospective studies. The study's quality is limited by the variables available for analysis. It is possible that including additional variables would further clarify the observations of this study.
Conclusion
In this risk-adjusted analysis of a large population-based data set, we have found evidence that both confirms and refutes, traditionally held disparities in access to minimally invasive surgery. Despite the LC gold standard, OC remains the initial approach in a surprisingly high percentage of cases. Additional research may more comprehensively identify the factors predisposing surgeons to pursue an OC in this era of minimally invasive surgery.
Footnotes
Acknowledgments
The authors thank Dave Primm for the help in editing this article.
Disclosure Statement
Samir Pandya is a consultant for TransEnterix.
Funding Information
No funding was received for this article.