
Abstract
Background:
Enhanced-view extended totally extraperitoneal repair (eTEP) technique for laparoscopic retromuscular ventral hernia (VHR) repair is a novel application recently described by some authors. We present our early single institution experience on this technique.
Methods:
Retrospective review of the eTEP technique for laparoscopic retromuscular VHR repair cases at our institution from October 2018 to June 2019 with 1 month follow-up was evaluated. Data analyses include patients characteristics, operative details, and complications.
Results:
A total of 18 patients were treated with eTEP. One patient was reoperated using the same procedure and hospital stay was 6 days. The same patient who had undergone transversus abdominis release developed a seroma that could be observed 20 days after surgery.
Conclusion:
Our short-term experience with eTEP access suggests feasibility of this approach in accordance with results from other authors. We do not think the technique is challenging, but it is necessary for it to be performed by surgeons with skills in laparoscopic abdominal wall reconstruction.
Introduction
Laparoscopic approach to ventral hernia (VHR) and incisional hernia was first described by LeBlanc and Booth in 1993. 1 This technique and its evolution provide information on which mesh is to be placed in the intraperitoneal onlay position and fixed to the abdominal wall through tacks or stick. It is a procedure that in comparison with open mesh repair relates to lower surgical site and mesh infection but requires fixation devices that may cause some acute and chronic pain problems.2–4 Also, despite great progress in mesh technology, nearly all types of meshes have been found to produce a varying level of adhesion or tissue reaction regardless of the material and coating used. Absorbable meshes from some manufacturers promise future good results in terms of adhesion, but even today they are very expensive. The extraperitoneal positioning of the synthetic mesh in laparoscopic inguinal hernia repair or open VHR with closure of the peritoneal flap has been shown to be rarely associated with complications induced by the mesh in terms of adhesion.5–7 Surgeons such as Belyansky et al. and Schwarz et al. have extended the indication to VHRs with the purpose to place the mesh in the retromuscular space, as the Rives and Stoppa technique.8,9 We believe, after experience with the Rives and Stoppa procedure, that mesh in the retromuscular space using the endoscopic technique will have advantages of both laparoscopic and open procedures. The technique has a steep learning curve and we think that it will make surgeons experts in wall reconstruction. In this article we present our short-term results of our experience in extended totally extraperitoneal repair Rives–Stoppa (eTEP-RS).
Materials and Methods
Patients
Between October 2018 and June 2019, 18 patients with VHR were treated with eTEP-RS. We selected all hernias that have a defect >3 cm for eTEP access. Patients were eligible if they met the following criteria: VHR (incisional or primary hernia), age ≥18 years, and American Society of Anesthesiologist (ASA) score I–III. The exclusion criteria were recurrent VHR, ostomy, prior wound complication, poor skin condition, body mass index (BMI) >30 kg/m2, steroid treatment, and noncontrolled hepatic disease. All patients underwent detailed analyses of complication, physical examination, biochemical test, chest X-ray, CT scan of the abdomen for hernia defect measurement, and study of abdominal wall characters. Signed informed consent was obtained from each patient. The same surgical team performed the procedure: 1 senior surgeon and 1 resident surgeon with experience on abdominal wall reconstruction (laparoscopic and open).
Surgical technique
The patient was placed supine with both arms tucked at the sides. The table was flexed. Foley was positioned in all patients. Monitor was placed in front of the surgeon. We marked with ultrasound the following: muscle rectus position, bilateral linea semilunaris, epigastric vessel, and hernia defect. For the eTEP-RS technique, one side retrorectus dissection was performed. For this reason, the port was placed in the opposite side of the hernia location (Fig. 1) We made a small incision for first trocars. The anterior rectus sheath was identified and incised. The space between the muscle rectus and posterior sheath is widened in all directions before with the surgeon's index finger and after with a gauze on a surgical instrument. Using this technical approach, the retrorectus space can be exposed under direct vision through a small skin incision that prevents intraperitoneal flow of air while performing the subsequent endoscopic release (Fig. 2). A first port was placed with gas insufflation up to a pressure of 12 mm Hg carbon dioxide. A 10 mm 30° scope was used for adequate overview of the whole space between muscle rectus and posterior sheath. After this, we placed the other port following the same technique as described by Beliansky et al. 8 (Fig. 3). The dissection was made using energy source. Sometimes to see intestinal adhesions on hernia it is necessary to do pneumoperitoneum through a lateral 5-mm port entry before dissecting the hernia sac. Inspection of the cavity was done using a 5 mm 30° scope, and if necessary, hernia contents were reduced with lysis on hernia sac through a laparoscopic scissor. Posterior rectus sheath defects were closed with 2-0 absorbable suture. The anterior rectus sheath defects were also closed with 0 self-gripping suture. For larger defects or when we have difficulty achieving midline fascial approximation, we performed ipsilateral or bilateral transversus abdominis release (TAR) and ports 4 to 6 were placed following the technique described by Beliansky et al.9–11 The defect area was calculated as given in Qandeel and the dimension of the defect was evaluated as oval. The equation used for oval shape area is 0.5 × horizontal measurement (in vivo) × 0.5 × vertical measurement (in vivo) × Pi. (Pi = 3.14). 12 The mesh area, required to cover the defect, was calculated by adding 5 cm overlap to both directions as an IEHS guideline. 13 This tailor-shaped mesh was used to cover the defect by 5 cm. Low weight large porous polypropylene mesh was positioned and secured using 8 mL fibrin glue (FG). Tacks were used only for pubis bone mesh fixation. All patients were given short-term antibiotic prophylaxis with 2 g cephazoline i.v. We allowed oral food the morning after the procedure. Drains were usually given for 24 hours. Analgesics were used in the first 24 hours routinely through a continuous elastomeric pump. Patients were usually discharged within 72 hours of the procedure and postsurgical abdominal binder was placed for 30 days.
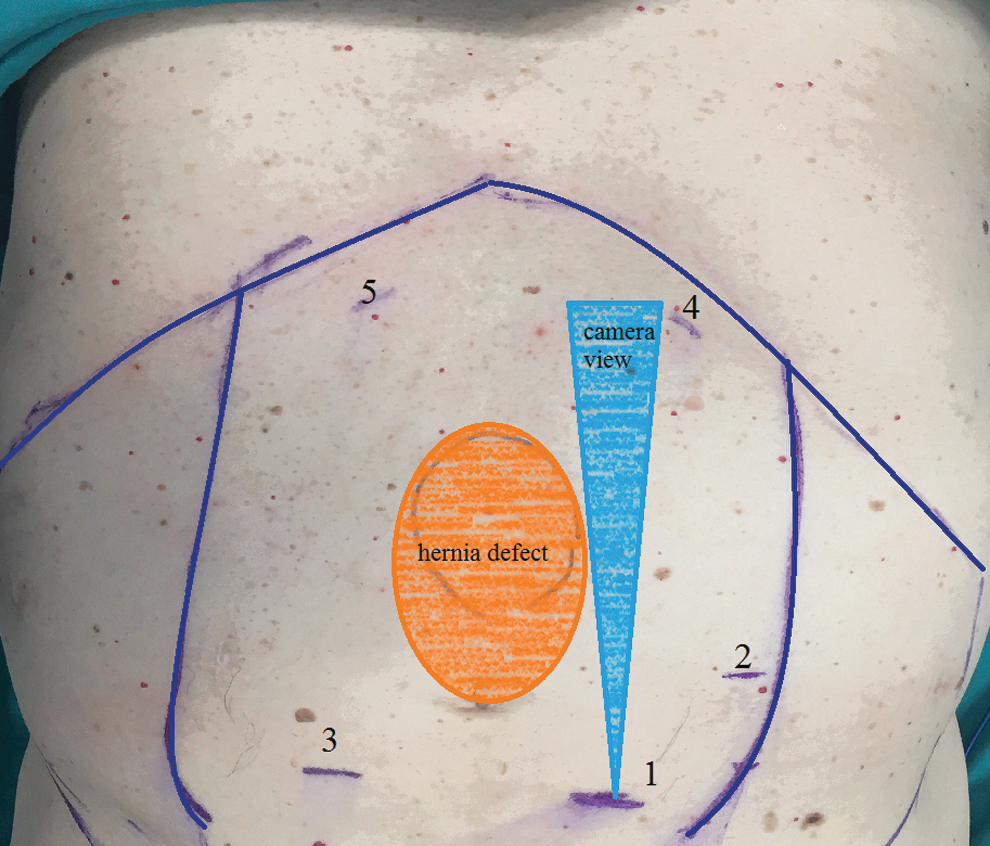
Port placement for upper midline defects.
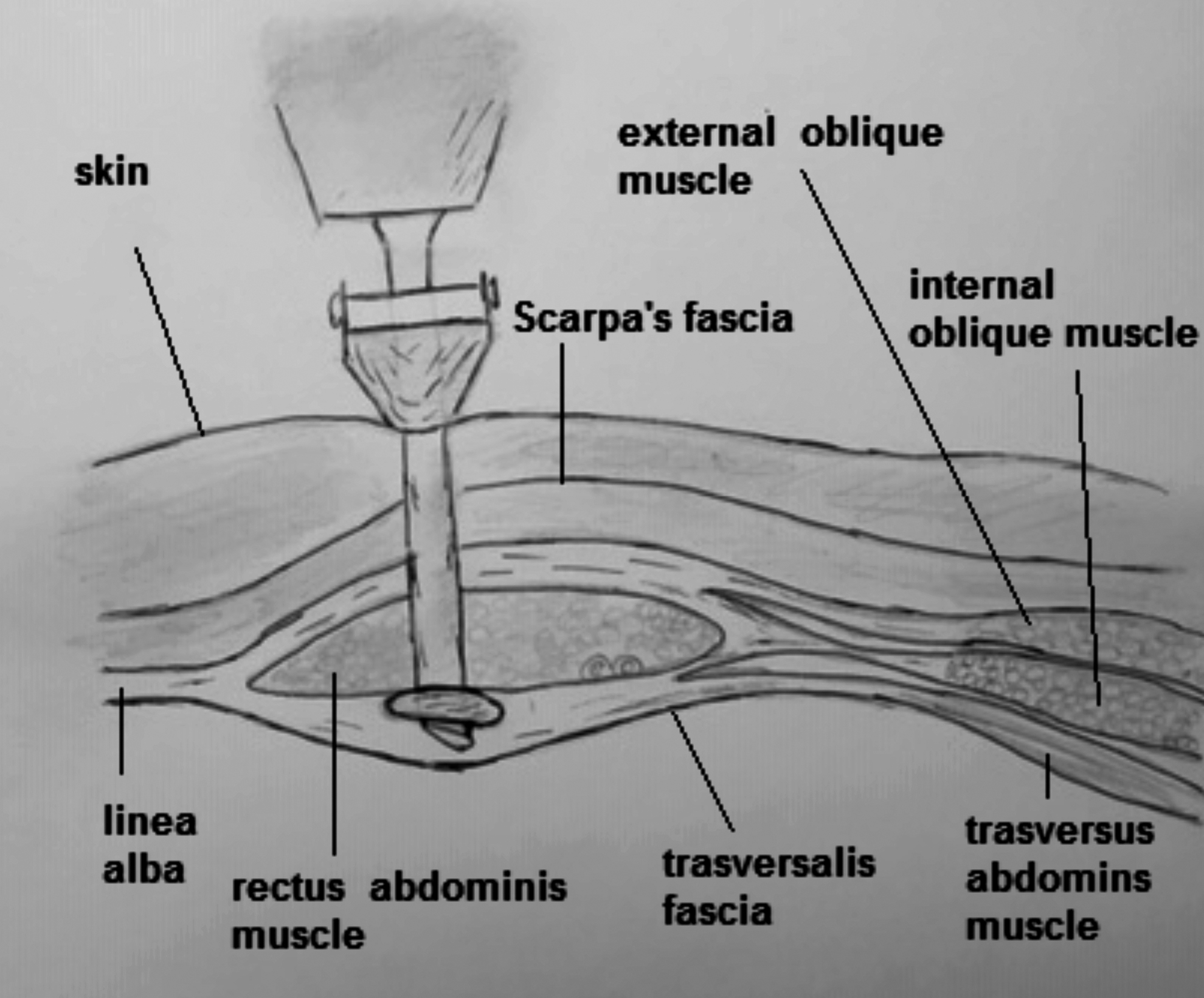
First port placement on abdominal view.
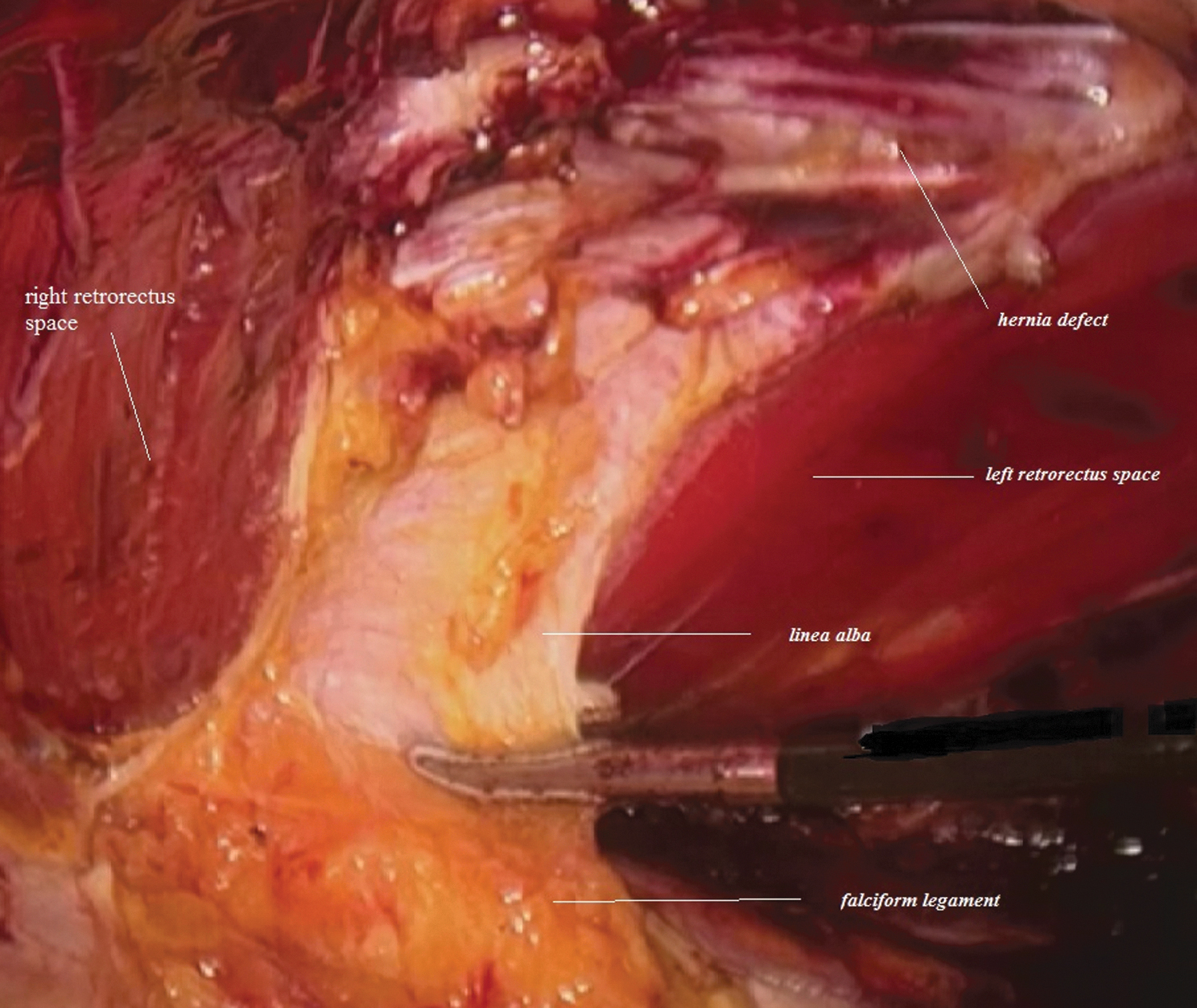
Dissection in upper midline defect.
Data collection and analysis
After each operation, we collected data from all VHR repair patients and entered the data into a database using Microsoft Office Excell® by the 2 surgeons (A.S. and C.C.) and 1 nurse (B.M.).
Results
Between October 2018 and June 2019, 18 patients with VHR were treated with eTEP. Ten were female and 8 were male with mean age 57.05 years. Mean BMI was 26.6 kg/m2 (Table 1). Incisional hernias were in 66.7% of patients and 33.3% of patients had primary VHR (umbilical and epigastric). Fourteen patients were treated with eTEP-RS. Three with eTEP-RS required bilateral transversus abdominis release, and one with eTEP-RS required ipsilateral transversus abdominis release. The mean operating time was 125.64 minutes and ranged from 90 to 178 minutes. Mean defect area was 43.31 cm2. The mean mesh size was 267.47 cm2. Mean hospital stay was 2.76 days and ranged from 2 to 6 days (Table 2). One patient developed a large hematoma, so we had to reoperate with same procedure, and hospital stay was 6 days. The same patient who had undergone TAR developed a seroma that was observed 20 days after surgery. Another 1 patient developed seroma 10 days after surgery. It did not show symptoms, therefore, we decided not to drain it. There was no recurrence at 1 month follow-up (Table 3).
Patients' Demographics
BMI, body mass index.
Perioperative Details
FG, fibrin glue; TAR, transversus abdominis release.
Postoperative Complications
Discussion
Open sublay mesh repairs have evolved during the past 50 years since Renè Stoppa and Jean Rives in France described independently their technique during the 1970s. 14 Open sublay and laparoscopic intraperitoneal mesh repair are common techniques for treatment of VHR, primary or incisional. The highlights for the patients are quality of life, pain recurrence, and hospital of length stay (LOS). With improvement in laparoscopic surgery during the years, quality of life has also improved, decreasing pain and reducing LOS, but in most of this procedure, the meshes were placed onlay. Despite progress in manufacturing technology, with lower risk of adhesion, the potential complication with intraperitoneal mesh has not been eliminated.15–18 In the literature there are increasing evidence suggesting good results in the patients' outcome with laparoscopic retrorectus mesh placement for VHR repair.19,20 Besides, with site of mesh location between anterior and posterior layer, it is possible to minimize complication related to traumatic fixation devices that increase the risk of adhesions, pain (acute or chronic), visceral, and nerve injury. To repair complex abdominal wall defects with sublay mesh, high skill in laparoscopic surgery is required. It is necessary to have good experience in laparoscopic closure of the anterior and posterior defects of the abdominal wall, which many surgeons already have. Before applying some new laparoscopic techniques (eTEP), in our experience, one drawback of laparoscopic surgery sublay mesh placement was the inability to manage larger defects due to the constraints of the workspace and rigid instrumentation, as also described by some authors. 21 We were able to safely repair only small defects with retromuscular techniques. With robotic surgery that allows more degrees of freedom, some of these deficiencies can be corrected. A recent study shows that when comparing robotic surgery with open sublay repairs, despite the size of the defects or use of TAR, there is improvement in hospital LOS for retromuscular hernia repairs. 22 With eTEP, minimal access by Belyansky et al. and other techniques, the retrorectus space must be meticulously developed with good working space and mesh placement from the peritoneal cavity without abdominal visceral contact. There are many different techniques for endoscopic retromuscular procedures (ventral TEP, eTEP, Milos, endoscopic mini/less open sublay technique [EMILOS], and Costa procedure), wherein some of these may be associated with TAR. We were fortunate to observe EMILOS and eTEP access techniques from the authors. We also have 3 years experience with endoscopic anterior component (ECS) separation using the Jörgensen technique. We decided to start with the eTEP technique because we thought that the first step of the ECS procedure is similar to the eTEP technique and that it was possible to reduce the learning curve. The initial reports of the eTEP access demonstrated lower rates of complication, less pain during the immediate postoperative period, and reduction in hospital stay.9,18 The 30 days wound-related complication given in Belyansky et al. was 3.8%, 9 which was 5.5% in our experience. Median LOS in the present experience was 2.76 days, which is comparable with data from other groups.9,19 It is clear that eTEP-RS diminishes LOS as compared with open abdominal wall reconstruction (AWR) because in our experience the patients spent a mean of 5 days in hospital (range 5–11 days).9,18 Postoperative pain in open AWR 23 leads to decreased activity levels 24 and increased LOS. 25 Recent studies have aimed to identify and mitigate factors associated with postoperative pain. Surgical techniques, location of mesh placement, and suture may be related to timing of postoperative pain. Recent studies have demonstrated that FG versus suture fixation (SF) for retromuscular mesh is associated with decrease of postoperative pain and improvement in activity in the short term with LOS of 3.4 days.26,27 This report in quality of life metric is similar to that published by Weltz et al. 28 In their study, le Carolinas Comfort Scale was administered preoperatively and after surgery. Results showed that at 6 months follow-up, patients with SF were 12 times more likely to report chronic pain than patients in the FG. Furthermore, the mesh position in the preperitoneal or retromuscle space allows for intra-abdominal pressure to secure the mesh between the peritoneum or posterior sheath and abdominal wall. Then it is possible, as Belyansky et al. reported, to secure the mesh only with FG. Currently, we have used the eTEP minimal access technique for hernias with a width of >3 cm that involves developing the retrorectus space bilaterally to duplicate the open RS repair. Those possible benefits in the use of this novel technique to duplicate the RS procedure with minimal access come down to merely the reduction in LOS and chronic pain with improvement of quality of life, but studies have to determine this relevance and long-term follow-up is needed to confirm whether applicability and efficacy of eTEP access VHR is necessary.
Conclusion
Furthermore, with improvement of laparoscopic and robotic surgeries on VHR repairs, until the perfect hernia repairs and perfect mesh were discovered, sublay location mesh placement remains one of the best options. Therefore, we think, based on our short-term experience and the literature data, that the use of eTEP minimal access is an attractive option to make sublay VHR repair in modern surgery. Prospective studies with larger patient groups and follow-up are needed to clarify its possible advantages.
Footnotes
Acknowledgments
The authors are grateful to Miss B. Mantovan for drafting the article and to all surgeons and nurses from the participating surgical departments for collecting the data.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.