
Abstract
Background:
Data following laparoscopic sleeve gastrectomy (LSG) for type 2 diabetes mellitus obese patients are extremely variable and we herein present our results.
Methods:
The data of 320 (90 diabetic) obese patients who had LSG were retrieved from prospectively collected database. Postoperative weight loss and glycemic control were evaluated during 24 months follow-up.
Results:
Diabetic patients had a significantly higher percentage excess weight loss (%EWL) (60.21 ± 11 and 72.9 ± 13) than nondiabetics (53.4 ± 12 and 62.5 ± 29) at 12 and 24 months post LSG, respectively. Diabetic patients with body mass index (BMI) >40 kg/m2 had significantly higher %EWL (64.17 ± 13 and 75.2 ± 16) than patients with BMI ≤40 at 12 and 24 months, respectively. The mean glycated hemoglobin and fasting blood glucose were 6.6% ± 1.4%, 6.1% ± 1.1%, 5.9% ± 1.2%, 5.8% ± 0.5%, and 110 ± 1.6 mg/dL, 106.7 ± 1.8 mg/dL, 99.2 ± 1.9 mg/dL, and 98.1 ± 1.2 mg/dL at 1, 6, 12, and 24 months, respectively. All patients had complete diabetes remission at 12 months, and this was maintained at 24 months.
Conclusion:
Diabetic obese patients with BMI >40 kg/m2, had a better %EWL compared with nondiabetics and to diabetics with lower BMI. Diabetes remission started early at 1 month. At 12 months, all diabetics had complete diabetes remission and this was maintained at 24 months. Our results need to be validated in a larger study, which evaluates impact of gastrointestinal motility on diabetes control.
Introduction
Over the past decades, obesity and type 2 diabetes mellitus (T2DM), has been considered the two most common metabolic disorders. 1 T2DM was estimated in 2010 at 8.3% of the adult population and obesity is considered a primary risk factor for T2DM; 90% of all patients with T2DM are overweight or obese. 2
Currently, all nonsurgical treatment are falling short of controlling diabesity 3 ; this could be attributed to the fact that many of the pathophysiological responses, including incretin enhancement, which follows bariatric surgery, are missing following calorie restriction diet alone. 4 Bariatric surgery, on the other hand, has been well established as an effective treatment for morbid obesity. 4 Significant weight loss and diabetic control following bariatric surgery were demonstrated in large studies3,5,6; however, data following laparoscopic sleeve gastrectomy (LSG) are extremely variable among published studies.7,8 The aim of the present work is to present our results on the effect of LSG on T2DM obese patients.
Methods
The present work was carried on all the patients who underwent LSG during the period from March 2016 to March 2017. Selection criteria for surgery were based on the recommendations of the American Association of Clinical Endocrinologists, the Obesity Society, the American Society for Metabolic and Bariatric Surgery,8,9 and the National Institute of Health (NIH) criteria for bariatric surgery. 10 Patients excluded from this study were those with obesity related to a reversible endocrine disorder, drug or alcohol abuse, noncompliance with the required postoperative lifestyle changes, and patients with severe uncontrolled and complicated diabetes; the latter are recommended for Roux-en-Y gastric bypass (RYGB) at our and many other centers. 11
The present study included 320 patients: 230 nondiabetic and 90 diabetic patients with no statistically significant difference in the mean age, body mass index (BMI), and sex incidence. Data for all the 320 patients were retrieved from prospectively collected database at the main University Hospital. Surgery was performed by the same bariatric surgeon. Clinical and demographic characteristics, preoperative weight, and BMI were recorded. In the diabetic group, the duration of diabetes and medications used to control it were noted and serum levels of biological markers, fasting blood glucose (FBG), glycated hemoglobin (HbA1c), and lipid profile, were measured. Both groups of patients (nondiabetics and diabetics) were further subdivided into two subgroups (subgroup A), where BMI was ≤40 kg/m2 and (subgroup B) with BMI >40 kg/m2. The effects of LSG on weight loss and glycemic control status were then evaluated.
LSG technique
LSG was performed to all patients as previously described. 12 In LSG, we routinely removed the esophageal fat pad. The first firing of the linear stapler was started 2 cm from the pylorus. We used a blue load (3.5 mm) for the entire stapling except for the first fire where we used a green load (3.8 mm). No buttress material was used. After completion of the stapling, we cover the suture line with a running 3-0 Prolene (Ethicon, Inc.) suture. The specimen of the stomach was then removed. Bougie size used was of 40 FFR.
Perioperative care
Operative time, hospital stay, and intraoperative complications were recorded. Follow-up of the patients were carried at the main University Obesity Clinic at 1, 6, 12, and 24 months following LSG; during the visits all the patients were assessed for any complications, BMI changes, and percentage excess weight loss (%EWL). Laboratory tests for the diabetic patients included FBG and HbA1c.
Postoperative %EWL was recorded at 6, 12, and 24 months; %EWL was calculated using the formula: (weight loss/baseline excess weight) X100, where excess weight = initial weight – ideal weight (ideal weight = 25 kg/m2). 13 Postoperative weight loss success was defined as %EWL over 50% maintained at least for a year. 14 The results of %EWL were compared between the different groups.
Following surgery all diabetic patients were put off antidiabetic medications and were observed for glycemic control (FBG and HbA1c). Complete T2DM remission was defined as FBG <100 mg/dL and/or HbA1c <6% and partial remission as FBG <126 mg/dL and/or HbA1c <6.5% and both off antidiabetic medication.4,15
Statistical analyses
Continuous variables were summarized as mean and standard deviations. The groups were compared using Mann–Whitney U test for continuous variables. The serum HbA1c levels were measured before surgery and at 1, 6, 12, and 24 months after LSG and compared with the Wilcoxon test. Statistical significance was considered at P < .05. Statistical analyses were performed using SPSS IBM® statistics version 24 (IBM Corporation, Armonk, NY).
Results
All 320 patients were included; the mean age was 42 ± 11 years, and 259 (80.9%) patients were females. Mean preoperative BMI was 48.99 ± 7.2 kg/m2. The mean age, BMI, and female sex incidence for the nondiabetic and diabetic groups were: 39.8 ± 4 and 43.3 ± 9 years, 48.59 ± 6.2 and 49.22 ± 6.1 kg/m2, and 80.4% and 82.2% respectively; the differences between the two groups were not statistically significant (P > .05). The mean duration of surgery and hospital stay were 70 ± 29 minutes and 1.1 ± 0.23 days, respectively. In the diabetic group, the mean preoperative FBG and HbA1c were 155.8 ± 2.4 mg/dL and 7.8% ± 1.6%, respectively. We had no mortality and a total of 12 complications (3.8%) occurred within the first 30 postoperative days. Minor complications included 5 patients (1.5%) with superficial surgical site infections that resolved with conservative management, 3 patients (0.9%) had bleeding during the first 24 hours. Two of these responded to conservative treatment and in only one laparoscopic reintervention revealed a perigastric hematoma with minimal collection (aspirated) with no active bleeder identified. Three patients (0.9%) had urinary tract infection that was managed with appropriate antibiotics. One patient (0.3%) had portal vein thrombosis that was managed conservatively.
Postoperative follow-up carried at the main University Obesity Clinic showed the following: in the diabetic group (90 patients), the number of patients who attended the 1, 6, 12, and 24 months visits were: 90 (100%), 84 (93.3%), 88 (97.7%), and 81 (90%), respectively; in the nondiabetic group (230 patients) these figures were: 202 (87.8%), 190 (82.6%), 209 (90.86%), and 184 (80%), respectively. The overall follow-up rate was 96.6%.
The mean preoperative BMI were 48.59 ± 6.2 kg/m2 and 49.22 ± 6.1 kg/m2 for the nondiabetic and diabetic groups, respectively. Successful postoperative weight loss (>50 %EWL) occurred in all the studied groups; the results of %EWL at 6, 12, and 24 months are illustrated in Table 1 and Figure 1. At 12 months %EWL was 53.4 ± 12 and 60.21 ± 1 for the nondiabetic and diabetic groups, respectively, while at 24 m it was 62.5 ± 29 and 72.9 ± 13. Diabetic subgroup B patients (BMI >40 kg/m2) had significantly higher %EWL (P < .05). In the nondiabetic group, we had 136 patients with BMI ≤40 kg/m2 (subgroup A) and 94 patients with BMI >40 kgm2 (subgroup B); %EWL for these patients were not significantly different.
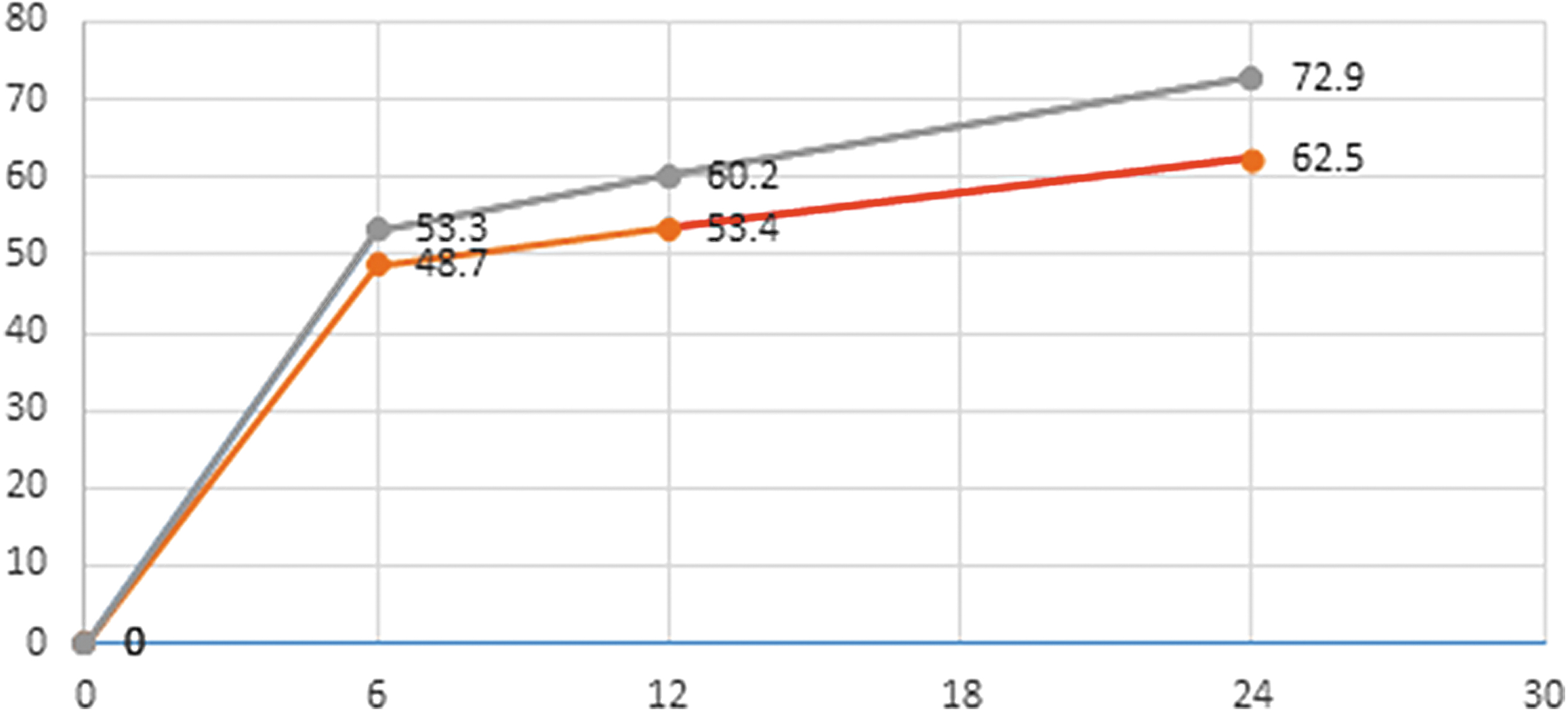
%EWL post LSG. Red line, nondiabetic; Gray line, diabetic; %EWL, percentage excess weight loss; LSG, laparoscopic sleeve gastrectomy.
Percentage Excess Weight Loss Post Laparoscopic Sleeve Gastrectomy
Nondiabetic versus diabetic.
Subgroup B (BMI >40) versus subgroup A (BMI ≤40).
BMI, body mass index; %EWL, percentage excess weight loss; LSG, laparoscopic sleeve gastrectomy.
A total of 90 patients (28%) were identified as T2DM at baseline. The mean diabetes duration was 7 ± 6.8 years and all the patients were preoperatively on antidiabetic treatment: (54 [60.6%]) patients were on oral antidiabetic drugs, 14 [15.5%] on insulin, and 22 [24.5%] on oral antidiabetics [OAD] plus insulin). Patients were taking between 1 and 3 medications with a mean of 1.4 medication. Evaluation of postoperative glycemic control for all diabetic patients showed that mean HbA1c changed from 7.8% ± 1.6% preoperatively to 6.4% ± 1.4%, 6.1% ± 1.1%, 5.9% ± 1.2%, and 5.8% ± 0.5% at 1, 6, 12, and 24 months post LSG, respectively (Table 2). Similarly the mean FBG changed from 155.8 ± 2.4 mg/dL preoperatively to 110 ± 1.6 mg/dL, 106.7 ± 1.8 mg/dL, 99.2 ± 1.9 mg/dL, and 98.1 ± 1.2 mg/dL at 1, 6, 12, and 24 months post LSG, respectively (Table 2).
Changes in Mean Glycated Hemoglobin and Fasting Blood Glucose Post Laparoscopic Sleeve Gastrectomy
FBG, fasting blood glucose; HbA1c, glycated hemoglobin; LSG, laparoscopic sleeve gastrectomy.
The response of DM to surgery in our study started early; all the 90 diabetic patients attended the 1-month follow-up visit and 74 of these patients (82.22%) had complete diabetes remission, whereas the remaining 16 patients (17.8%) had partial remission; these partially remitted patients did not receive any antidiabetic medication and were managed by strict diet control. At 6 months post LSG, only 6 patients were still having partial remission and were also managed by diet control only. All the patients who attended the 12 and 24 months follow-up visits (88 and 81 patients, respectively) had complete diabetes remission (Table 3 and Fig. 2).
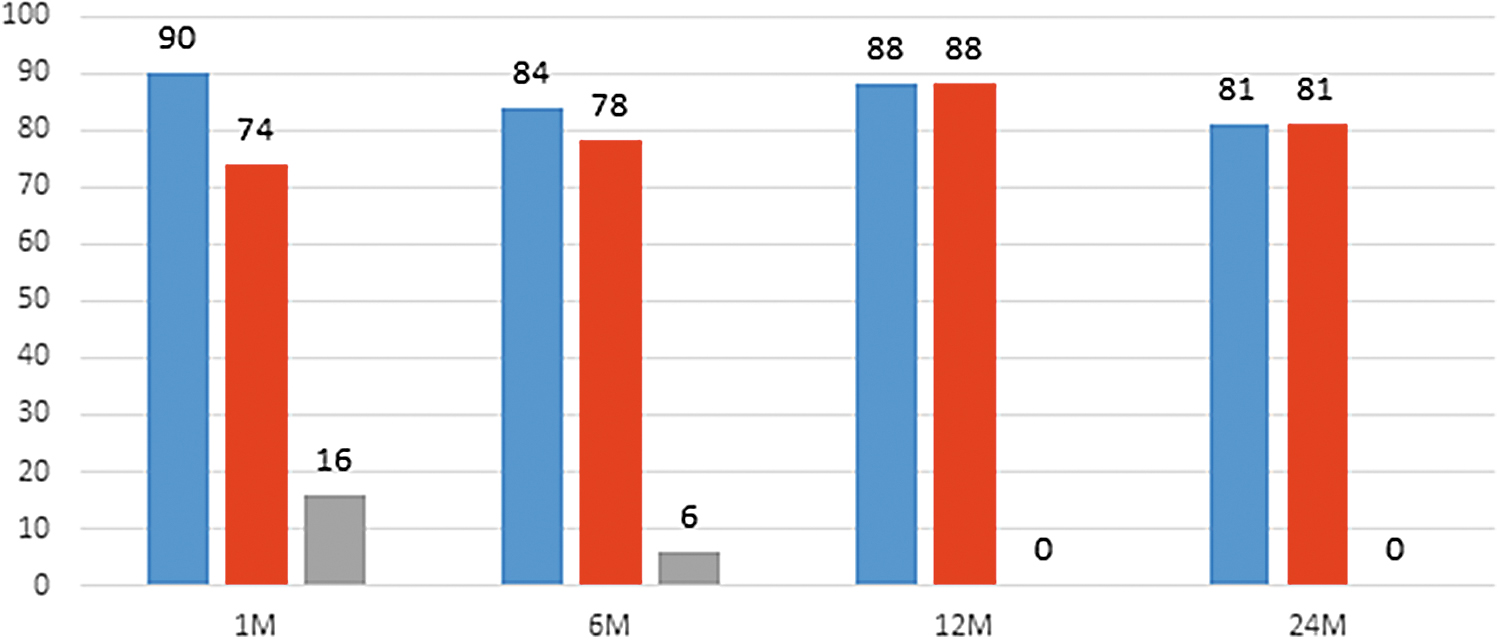
Remission of T2DM post LSG. Blue, patients attending; Red, complete remission; Gray, partial remission. LSG, laparoscopic sleeve gastrectomy; T2DM, type 2 diabetes mellitus.
Postoperative Glycemic Control
LSG, laparoscopic sleeve gastrectomy.
Discussion
Several surgical procedures have been tried to control obesity and T2DM with variable outcome as regards weight loss, diabetes control, and side effects. The two most commonly performed procedures in this respect are LSG and RYGB. 16 Published studies revealed extremely variable results on the control of T2DM following LSG.6,7 We herein present our preliminary results on the use of LSG for the treatment of diabetic obese patients.
In the present work the mean age, BMI, and sex incidence were not significantly different (P > .05) in the diabetic and nondiabetic groups of patients, The operative time, hospital stay, and complications were within the accepted values for this procedure. 13 We had no mortality or major complications and most of the patients attended the scheduled follow-up visits; the overall follow-up rate was 96.6%.
There was no significant difference in the preoperative BMI of diabetic and nondiabetic patients in the present study (P = .2). Weight loss started soon after surgery and the mean %EWL in the nondiabetic group is consistent with that reported in the literature by Hoogerboord et al.13,17 However, in the diabetic group the %EWL were significantly higher (P < .05). When we further subdivided the diabetic patients according to the preoperative BMI it was found that diabetic patients in subgroup B with BMI >40 kg/m2 had significantly higher %EWL compared with subgroup A with BMI ≤40 kg/m2 (P < .05). In the nondiabetic patients, the differences in %EWL between patients with BMI ≤40 and >40 kg/m2 were not statistically significant (>0.05). These findings suggested that obese diabetic patients with BMI >40 kg/m2 had a better loss of weight following LSG compared with nondiabetics and diabetics with BMI ≤40 kg/m2. The results obtained in the present work are different from what previous studies have showed, where preoperative BMI was not predictive of weight loss following bariatric surgery.4,15,17
Our findings could be attributed to the discrepancy in the motility changes in the nondiabetic and diabetic obese patients: In nondiabetic obese patients small intestinal transit time is similar to that in normal-weight subjects, whereas in diabetic patients gastric and small intestinal motility are decreased. 18 As LSG leads to accelerated gastric and small intestinal motility 19 associated with an impact on the intestinal metabolic functions,20,21 it would therefore be expected that weight changes in diabetics will be more marked.
In the present work, there was a significant postoperative decrease in the mean HbA1c and FBG; the response of diabetes started early with complete remission in 82.2% and 92.8% of the patients at 1 and 6 months post-LSG, respectively, whereas the remaining patients had only partial remission and were managed by strict diet control and received no antidiabetic medication. At 12 months all the patients had complete diabetes remission and this was maintained at 24 months. Our findings confirm previous results reported in the literature.6,7,22,23 An explanation to the good glycemic control seen in our and other studies could be attributed to multiple factors, including technical factors such as meticulous and complete resection of the ghrelin secreting gastric fundus and to the small size of antrum left with its effects on gastric emptying and intestinal motility. LSG with antral resection leaving 2–3 cm antrum (compared with antral preservation 6 cm) was found in a meta-analysis 24 to be associated with accelerated gastric and intestinal motility, whereas the initiation of cecal filling and ileocecal valve transit are delayed; the fast delivery of nutrients to the distal intestine where it stays stimulates increased release of Glucagon-like peptide-1 GLP-1 and peptide YY, which have antidiabetic effects (suppressing glucagon and increasing insulin secretion). All this contributes to improved glucose control, reduced food intake, and decreased weight.19,25–27 Moreover, our study group included young patients with a low HbA1c and a short duration of diabetes.
The rates of diabetes remission following LSG varied in the literature; Pham et al. 22 found a 62.5% remission, Leonetti et al. 7 reported an 80% resolution after 18 m, and Pournaras et al. 3 noted a 26% remission rate at a median of 23 m. Several other studies and systematic reviews showed similar remission rates varying between 66.2% and 96%.6,7,28,29 Dillon et al. 2 in a prospective, single-center cohort study reported that 1 month following LSG 50% of his 30 T2DM patients discontinued all antidiabetic medications, with a further decline at 3 and 6 months. Discrepancy in the rate of diabetes remission following LSG reported in the different studies could be due to the lack of standardization for the criteria of remission and the technique of the sleeve gastrectomy itself; rapid good remission in the first postoperative month could however be due to the strict all-fluid diet the patients get during these early weeks. Although laparoscopic Roux-en-Y gastric bypass (LRYGB) is associated with a higher diabetes remission rate and more loss of weight compared with LSG, yet, LSG is technically simpler, safer, induces less vitamin and micronutrient deficiency, and is a cost-effective treatment.11,30
The Look AHEAD trial (Action for HEAlth in Diabetes) 31 and several other studies underlined that weight loss alone does not explain the improvement in glycemic parameters and diabetes remission following LSG and that T2DM resolution occurred before a significant weight loss suggesting underlying physiopathological changes in gut hormone secretion 22 ; Hoogerboord et al. as well as several previous studies attributed the metabolic effects of LSG to the reduction of ghrelin, the increased levels of hindgut hormones enhancing glucose dependent insulin and to the postoperative changes in gut micobiome.11,18,32
To increase the benefit to risk ratio of bariatric surgery, many studies tried to find the best predictors of T2DM remission after surgery and found, among many factors, that shorter T2DM duration <8 years, preoperative good glycemic control without insulin, patient compliance, lower baseline HbA1c, and profound postsurgical weight loss, have been all associated with favorable outcome.3,5,31 The degree of weight reduction rather than preoperative BMI, which is of no predictive value, has been shown to play a central role in predicting responders versus nonresponders.4,33 Many of these favorable factors were present among our cases hence the good remission of diabetes in our study. In search of the ideal procedure for diabetic obese patients, we agree with Milone et al. on the need for more characterization of T2DM remission determinant, including several published scoring systems.24,25,33
Limitations
Because of the relatively small sample of severely obese diabetic patients, our results need to be validated in a larger study, which should include gastrointestinal motility assessment.
Conclusion
Diabetic obese patients with BMI >40 kg/m2 achieved a significantly higher %EWL following LSG compared with nondiabetic patients and to diabetics with lower BMI. A BMI of more than 40 kg/m2 in diabetic obese patients may predict a higher weight loss. Diabetes remission started early at 1 month and all diabetic patients had complete remission at 12 m and this was maintained at 24 m post LSG. Our results need to be validated in a larger study, which evaluates impact of gastrointestinal motility on diabetes control. This study was approved by the Ethics Review Committee.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.