
Abstract
Background:
Laparoscopic sleeve gastrectomy (LSG) is now one of the most common surgical procedures worldwide. It was initially defined for staged procedures in super or super-super obese, or in very complex patients. The primary objective of the study was to assess the safety of LSG for morbid-obese (MO, body mass index [BMI] >40 kg/m2) and super-morbid-obese (SMO, BMI >50 kg/m2) patients in terms of operative and postoperative complication rate.
Methods:
This study involves a retrospective analysis of a prospective database that included data for patients who underwent LSG, between 2008 and 2017, in our institution. All LSG procedures were performed by the same two certified bariatric surgeons following a standardized surgical procedure. Data on operative and postoperative complications were collected for all the patients.
Results:
A total of 713 patients were included in the study 495 (61.42%) were MO (mean age 46.06 ± 11.98 years) and 218 (30.58%) were SMO (mean age 42.98 ± 11.17 years). There were no significant differences between both groups in terms of minor and major postoperative complications or long-term complications. Postoperative mortality was slightly higher in the MO group but without statistically significant differences (MO: 0.2%; SMO: 0%). Long-term reoperation rate and late complications were higher in the MO group 6.12% versus 4.04% and 17.43% versus 15.15%, respectively. Reoperation for gastroesophageal reflux disease was higher in MO patients compared to SMO and weight issues reoperation higher in the SMO.
Conclusion:
We found LSG as a safe procedure in both groups. Interestingly long-term reoperation and complications rates were higher in the MO group.
Introduction
Bariatric surgery (BS) is well recognized as the best treatment for morbid obesity. According to the World Health Organization, the worldwide prevalence of obesity has seen a threefold increase since 1975. Approximately 39% of adults with age ≥18 years were overweight in 2016, and 13% among them were obese. 1 Obesity is the second leading cause (after smoking) of the preventable deaths in the United States. 2 Currently, United States ranks among first in high-income countries for the highest body mass index (BMI), 1 of every 3 adults have a BMI over 30 kg/m2.3,4
Among the different types of bariatric procedures, sleeve gastrectomy (SG) is today one of the most performed worldwide. 5 It was initially designed as a step procedure for super-morbid-obese (SMO) patients; it has become a primary procedure in the last years. Due to its technically feasibility, it was quickly adopted by all the bariatric surgical groups. Different studies have demonstrated its safety and effectiveness. 6
SMO patients become a challenge due to their excess weight and morphological characteristics, but also for the morbidity conditions associated. This group of patients is mostly benefited by procedures with strong malabsorptive component.
Laparoscopic sleeve gastrectomy (LSG) was initially proposed to be a first-step surgery for SMO patients in a staged strategy for a definitive bariatric procedure. However, due to its simplicity and promising results in the management of comorbidities associated with obesity, LSG is now considered a definitive operation.6–8 According to different studies, LSG not only provides satisfactory and durable weight loss but also helps in the resolution of several significant comorbidities, including metabolic, cardiovascular, renal, and respiratory disorders. More importantly, it helps in reducing mortality rate and improves the quality of life in obese patients.7,8
The strategy to manage SMO patients is usually guided by staged procedures. During the first stage a LSG is performed, and several months later, with some weight loss and better control of other comorbid conditions, the definitive procedure is done. This strategy is defined to reduce the risk of complications of a major bariatric procedure in such complex patients. 9 Despite this, there are some voices claiming for the inherent risks of the LSG in this population.6,9
In this study, we aimed to assess the operative and postoperative complications of LSG in SMO patients and compared them with those observed for morbid-obese (MO) patients who underwent LSG.
Methods
Data source and study population
After Board approval, retrospective analysis of a prospective database included data of patients who underwent a LSG, between 2008 and 2018, in Hospital Universitario Vall Hebron de Barcelona, EAC-BS Center of Excellence, Spain. We analyzed operative and postoperative minor and major complications; length of hospital days, weight reduction, and incidence of reinterventions were collected expediently and telephonically during the follow-up period. A multidisciplinary team consisting of nutritionist, psychologist, endocrinologist, and bariatric surgeons was involved in the evaluation and the treatment of all the patients. For long-term follow-up analysis, only patients with a minimum follow-up of 2 years were included.
Statistical analyses
The statistical analyses were carried out using STATA® 13.1 statistical analysis software (StataCorp LLC, College Station, TX). Categorical study variables were presented as counts and proportions, and differences between the groups were evaluated using Pearson's Chi-square test or Fisher exact test, as appropriate. Continuous study variables were presented as mean and standard deviation, and differences between groups were evaluated using the Student's t-test or Mann–Whitney U test. All P values were calculated using two-sided tests and were considered statistically significant at level <.05.
Presurgical interventions
Written informed consent was provided to all the patients before surgery. All patients underwent preoperative and postoperative counseling sessions and were encouraged to complete the periodic examinations; also they were provided with the counseling related to dietary, healthy lifestyle, and exercise for about 3–6 months.
A very low-calorie liquid diet was prescribed for 2–3 weeks before and after the surgery.
Indication was given to introduce them later on a high-protein low-calorie diet and multivitamin supplementation.
Operative and postoperative interventions
All the LSG procedures were performed by four certified bariatric surgeons. A standard 5-trocar technique was used. First, the small vessels of the greater curvature were transected using a harmonic energy; SG was performed starting ∼3 to 5 cm proximal to the pylorus. A linear cutting laparoscopic stapler was used 60 mm (Echelon Endopath EC60TM), with calibration 32 Fr orogastric tube. In the majority, the staple line was reinforced using a running 2/0 polypropylene suture or synthetic copolymer polyglycolic acid with trimethylene carbonate Gore SEAMGUARD™ Bioabsorbable Staple Line Reinforcement (W.L. Gore & Associates, Inc., Flagstaff, AZ).
Gastric leak test was performed with air and methylene blue. We decided to include patients with Robotic SG performed with da Vinci® S Robotic system (Intuitive Surgical, Inc., Sunnyvale, CA). Jackson-Pratt drain was placed at the beginning of the series, along the staple line in the left subphrenic space. Patients were discharged after they tolerate clear liquids without signs or symptoms of bleeding. As a usual practice, the drain was removed 48–72 hours after surgery.
Outcomes
The primary outcome of this study is to assess the safety of LSG in MO (BMI >40 kg/m2) and SMO (BMI >50 kg/m2) patients. We evaluated the incidence of operative and postoperative complications between the two groups.
Results
A total of 713 patients were included in the study. Four hundred and ninety five (61.42%) were MO and 218 (30.58%) were SMO; their age was 46.06 ± 11.98 and 42.98 ± 11.17, respectively.
The mean length of hospital stay was 2.92 ± 7.41 days for the MO group and 4.66 ± 11.14 days in the SMO group. Five hundred and ninety-three (73.2%) underwent laparoscopic and 120 (16.8%) underwent a robotic procedure. Both groups were comparable in terms of comorbidities at baseline (Table 1).
Baseline Demographics and Characteristics of Body Mass Index <50 kg/m2 and Body Mass Index >50 kg/m2 Patients, Undergoing Laparoscopic Sleeve Gastrectomy
BMI, body mass index.
Operative and postoperative outcomes
No patient requires conversion to open surgery in the laparoscopic group or to laparoscopic in the robotic one. Operative time, length of hospital stay, and time to recovery were comparable for patients in MO and SMO groups. Regarding postoperative complications, there were 5 (2.3%) versus 4 (0.8%) leaks, respectively, and 2 (0.9%) versus 9 (1.8%) bleedings. There was only 1 death in the MO group due to a massive myocardial infarct 3 weeks after patient discharge (Table 2). No diarrhea, ulcer, digestive tract hemorrhage, dumping syndrome, or Wernicke was reported for any patient in SMO or MO group in the long term. No statistical difference was observed in the long-term follow-up. There was significant difference among groups in reoperation rate, and indication of MO patients tend to have more reoperations due to gastroesophageal reflux disease (GERD) (which was confirmed with phmetry and manometry during the follow-up period) (5.5% versus 2.3%) and SMO patient for insufficient weight loss (6.4% versus 1.8%) (Table 3). Distribution of complications over time and number of cases showed no statistical difference among groups. However, observed percentages of complications decrease during time with number of cases. Leak rate decreases from 3.5% to 0.6% during time, and hemorrhage decreases from 2% to 1% during the study (Table 4).
Early Postoperative (<30 Days) Complications of Body Mass Index <50 kg/m2 and Body Mass Index >50 kg/m2 Patients, Undergoing Laparoscopic Sleeve Gastrectomy
BMI, body mass index; PTE/DVT, pulmonary thromboembolism/deep venous thrombosis.
Late Postoperative (>30 Days) Complications of Body Mass Index <50 kg/m2 and Body Mass Index >50 kg/m2 Patients, Undergoing Laparoscopic Sleeve Gastrectomy
BMI, body mass index; GERD, gastroesophageal reflux disease.
Early Postoperative (<30 Days) Complication Distribution Over Time According to Number of Patients Undergoing Laparoscopic Sleeve Gastrectomy
PTE/DVT, pulmonary thromboembolism/deep venous thrombosis.
Most of the complications appeared in the first 100 cases; after those, the complication rate dropped significantly. The leak rate in the first 200 cases was significantly higher (3.5%) in the first 200 patients compared to the last 300 patients where the leak rate was 0.6% (Table 4).
Patients were followed up for an average time of 32.6 ± 18.4 months after surgery. A total of 6 patients, 3 in each group, were lost to follow-up. The total weight loss expressed in kilograms was 34.1 ± 14.3 and 48.7 ± 18.1; and the percentage of excess weight loss was recorded as 66.3 ± 24.3 and 73.9 ± 213.8 for the patients in the MO and SMO groups, respectively (Fig. 1).
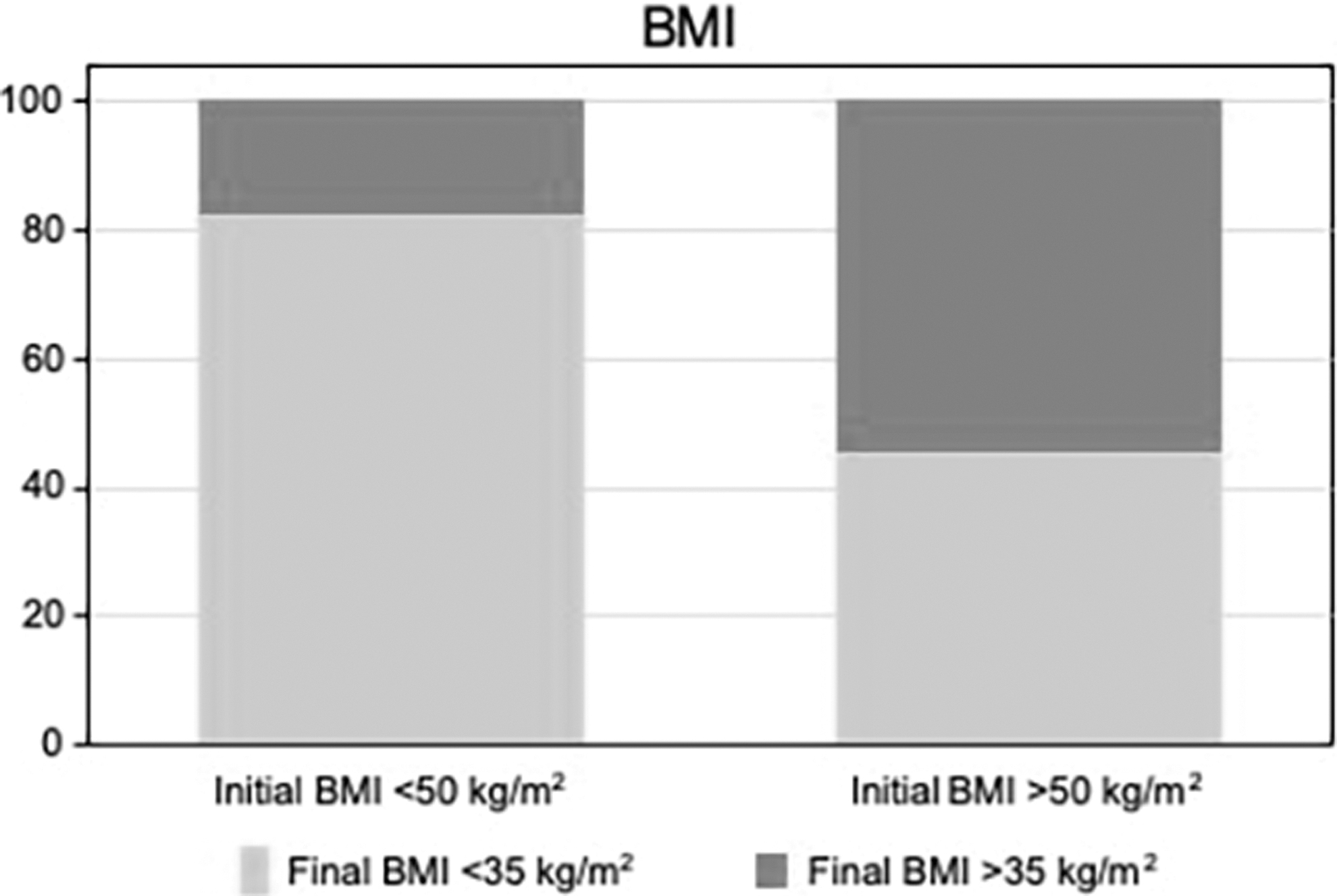
Percentage of patients with final BMI <35 kg/m2 or >35 kg/m2, during follow-up according to groups of MO or SMO patients. BMI, body mass index; MO, morbid-obese; SMO, super-morbid-obese.
Discussion
We present a retrospective study of complications after LSG comparing among MO and SMO patients. We presumed that according to the technical complexity derived of more weight per square meter and intra-abdominal fat morbidity would be increased in this group. We found that the SMO didn't have higher morbimortality.
Nowadays LSG has gained popularity in the bariatric community due to its several benefits over laparoscopic adjustable gastric band and Roux-en-Y gastric bypass, which include technical simplicity, fewer major and minor complications, as pylorus is preserved dumping syndrome is avoided, and maintenance of nutrient absorption without implantation of any foreign material in the body with a smaller remnant ghrelin-producing gastric tissue to reduce appetite.2,3,9,10
Results obtained from a recent meta-analysis for seven randomized clinical trials (RCTs) evaluate major complications and six RCTs evaluate minor complications. They conclude that LSG is associated with significantly lower rate of major and minor complications compared to RYGB. However, results obtained for other safety-related parameters, such as readmission rate, reoperation rate, and 30-day mortality rate, were comparable for both surgical procedures. 10 LSG has been reported to be a feasible and relatively safe definitive surgical option for rapid weight reduction in high-risk patients who require a secondary nonbariatric procedure, such as knee replacement, nephrectomy, or spine surgery.3,11
LSG is associated with acceptable morbidity and mortality and is effective in providing sustainable weight loss and controlling the comorbidities associated with obesity such as diabetes, cardiovascular disorders, obstructive sleep apnea, dyslipidemia, and nonalcoholic fatty liver in MO patients. 12 It has also been reported that LSG provides a significant improvement in the quality of life among MO patients. Due to all these benefits, LSG has become progressively popular among global patients and surgeons, as a definitive BS for weight reduction, especially during the last decade. 13 This is reflected in the data showing a significant increase in the number of LSG procedures carried out in different countries.2,8,9,14
With the increase of LSG in MO patients, the safety and efficacy of LSG for SMO patients (BMI >50 kg/m2) remain in controversy. Multiple studies have questioned the safety and efficacy in SMO patients. Larger clinical trials are needed to evaluate LSG as a routine BS in this patient population.
Moreover, some studies have reported that SMO patients tend to regain weight after 1 year of the LSG. Thus, many researchers have proposed to utilize LSG as a first step procedure for the management of SMO patients.3,6,15–19
The main outcome of our study is to evaluate the safety of LSG in this patient population in terms of complications and secondary to assess the efficacy of procedure in terms of percent weight loss after surgery. Another interesting aspect is the apparent learning curve for LSG in terms of major postoperative complications. The incidence of leakage and hemorrhage in our series decreases over time; we suggest that this finding is derived of acquisition of better technical skills and expertise during the time decreasing the morbimortality (Fig. 2 and Table 4). Some authors have considered that 60 cases are required to reach experience in reducing postoperative complications and costs after LSG. 20
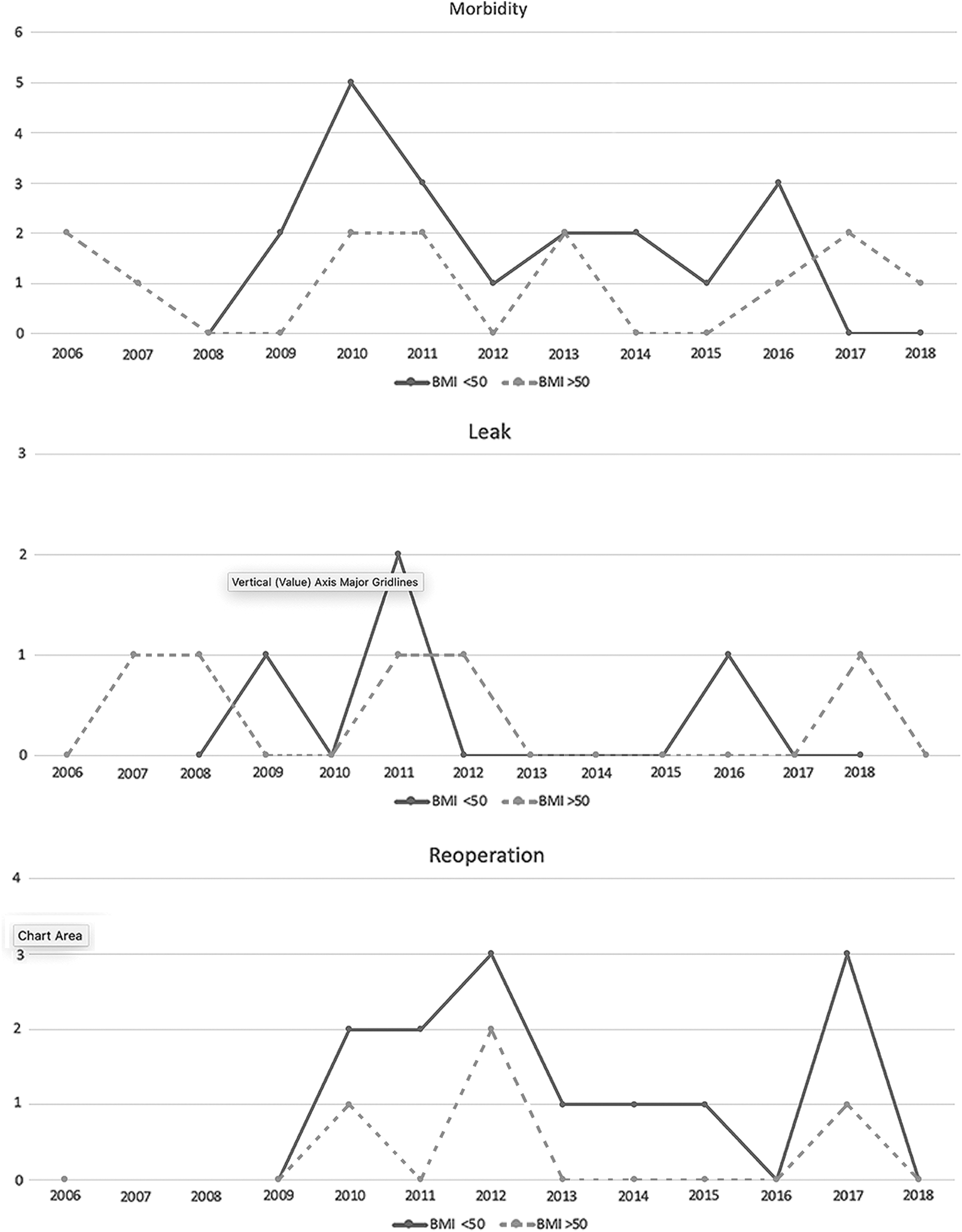
Distribution of morbidity, incidence of leakage, and reoperation among time comparing patients with MO and SMO. MO, morbid-obese; SMO, super-morbid-obese.
Regarding complications after LSG, literature reports a wide range, from 1% to 29%. Most common postoperative complications reported include leakage, hemorrhage, fistula, abscess, gastric dilatation, stricture, wound complication, and nutritional deficiencies.7,8,14,17
Results obtained in our study are similar with previously reported data. Leakage, bleeding, diarrhea, ulcer, digestive tract hemorrhage, dumping syndrome, or Wernicke syndrome was examined; our series presented low incidence for other major complications.
In t2 patients, laparoscopy exploration in reoperative setting did not find any leak, showing that the fast management provides better results to patients. In the long-term reoperation, for MO patient the main indication was GERD symptoms. These data might be related to technical issues, such as long-term stenosis. A recent systematic review and meta-analysis evaluated exposure to distal esophagus to severe reflux. Thirty-five studies were included; pooled random effects analysis of the change in the percentage of patients reported to have reflux between pre- and postoperative groups showed an increase of 19% following SG (85% confidence interval [CI] 15%–22%, P .0001). High heterogeneity among studies was I2 95.4%. This review also evaluated the incidence of the novo Reflux in 35 studies at a rate of 23% (95% CI; 17%–29%, P = .0001) also with high heterogeneity among the studies. 21
Multiple mechanisms are related to GERD, including the changes due to operative procedure as normal architecture of antireflux barrier and even technical surgical problems as stenosis in the gastric tube. Compared to SMO patients, the LSG was also considered as staged approach for “inadequate” weight loss. SMO patients have major excess weight and higher BMI that's the reason they are a population more exposed to have residual BMI over 35 kg/m2.
From our point of view, these data reflect the need of a staged strategy during the first year, when weight loss falls, promoting a conversion of LSG to a malabsorptive procedure such as Duodenal Switch or Single Anastomosis Duodeno Ileal-SG.
In cases of insufficient weight loss patients' behavior, technical aspects of the previous LSG must be considered to define the better strategy in revisional surgery. At our institution a prospective study is running comparing single anastomosis duodeno–ileal bypass with sleeve gastrectomy as a first step or staged procedure in patients with SMO.22,23
It is also important to remark that most of the complications in both groups were collected during the first 100 cases of LSG at the institution. Learning curve is a very important concept to take into account even in experienced surgical groups. This finding also translates the potential complexity of the LSG technique. Apparently, advanced surgical skills are not needed to perform LSG, but the lack of experience always can lead to complication even for a more feasibly not technically challenging procedure. Experienced bariatric surgeons advice excellent skills in bariatric field. The special morphological and anthropometric characteristics of MO and SMO demand specific training.
The robotic experience has been previously published by our group and we did not see any differences in complications during the learning curve compared to laparoscopy sleeve gastrectomy; the only difference was in operative time. Being the initial series and considering SO as more surgically demanding, in the 100 robotic SG the mean preoperative BMI was 48.8 kg/m2 in the robotic arm and 47.6 kg/m2 in the laparoscopic.24,25
This study has a number of strengths. The study population is large; reliable results can be drawn. All the procedures were carried out by the same experienced surgeons following a standardized procedure at the same institution. All the patients had long followed up for up to 64 months to evaluate long-term results. Our follow-up protocol is 3, 6, 9, 12, 18 months and after 2 years consecutively until postoperative year 5 besides the efforts of the multidisciplinary team. Of the total population, 40.49% was lost at 5 years.
The limitations relied that it is not a randomized single-center study, in which unintentional selection bias exists. Even in our cohort population the percentage of woman was higher comparing to male population; the percentage comparing our groups did not reach statistical significance.
The patients correspond to a single geographical location. Therefore larger, randomized, long-term comparative study might provide more inputs about the safety and efficacy of LSG for SMO patients.
Conclusion
No significant difference in the operative and postoperative complications was observed between the MO and SMO patients who underwent LSG. The procedure was effective in long-term weight and BMI reduction for patients included in both the groups. In our experience LSG can be performed safe and effective as a definitive bariatric procedure for the management of obesity and associated comorbidities in both settings, MO and SMO.
Footnotes
Disclosure Statement
None of the authors have any conflict of interest for this article.
Funding Information
No funding was received for this article.