
Abstract
Background:
Thoracic outlet syndrome (TOS) results from compression of neurovascular structures supplying the upper extremity as they exit the thoracic outlet. Depending on the clinical presentation, surgical decompression may be required.
Objectives:
Transaxillary (TA) and supraclavicular (SC) approaches are both widely utilized and deemed effective. Our objective was to review the outcomes for both approaches at our institution.
Methods:
A retrospective review was conducted on patients who underwent thoracic outlet decompression between 2010 and 2015. Data on demographics, comorbidities, presenting symptoms, and type of TOS (neurogenic, venous, or arterial) were collected. Operative times, length of hospital stay, perioperative complications, and outcomes were also studied.
Results:
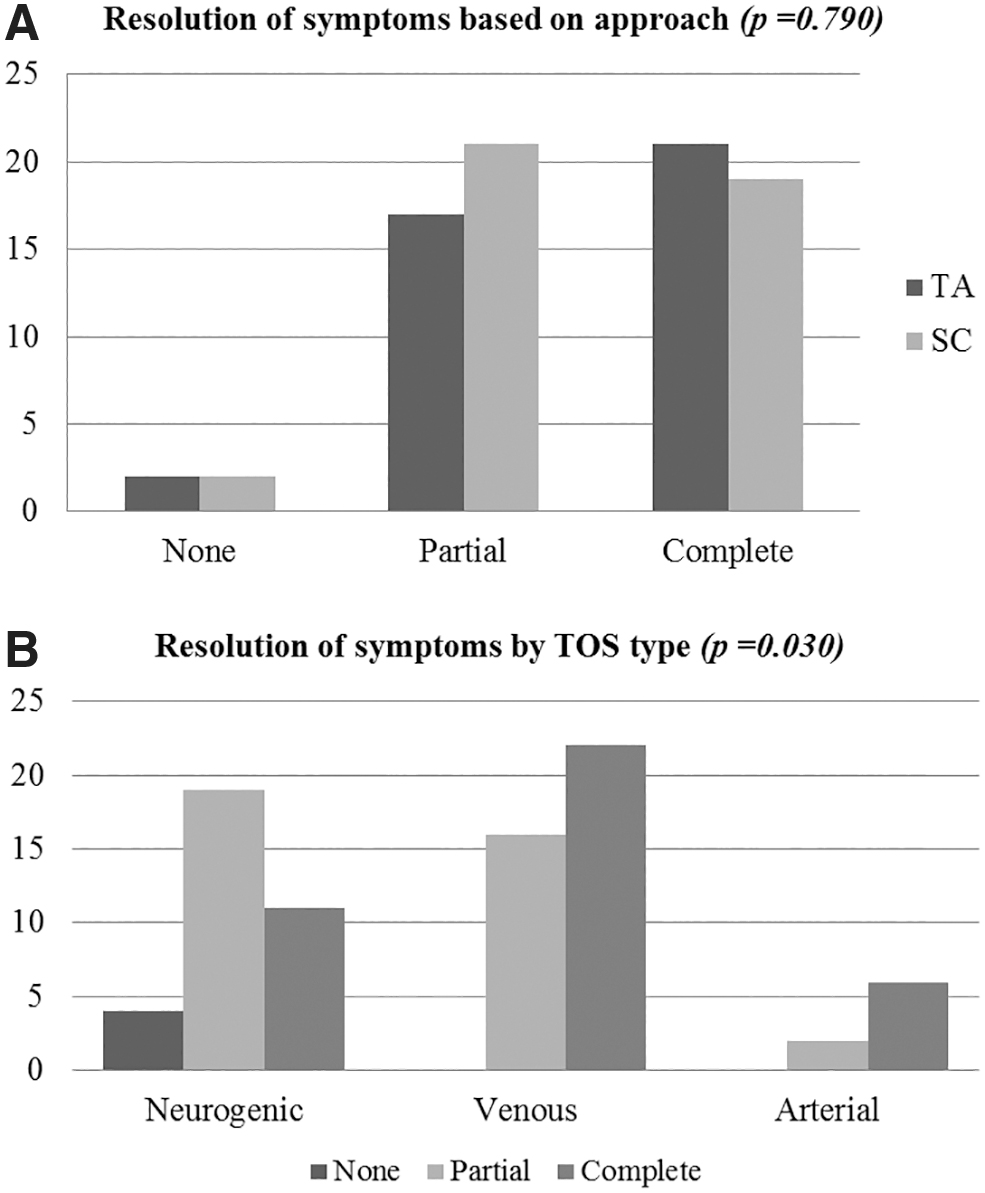
A total of 82 thoracic outlet decompression procedures were performed during the study period: 42% neurogenic TOS, 46% venous TOS, and 12% arterial TOS. In total, 49% underwent TA approach and 51% underwent SC approach. Adjunct procedures were performed in 13% of patients. There were no significant differences in average operative time (151.3 ± 54.1 minutes versus 126.1 ± 36.1 minutes, P = .11) or hospital stay (2.3 ± 1.9 days versus 2.4 ± 1.4 days, P = .23) between both groups, respectively. Minor complications were seen in 6% of patients with no significant difference in both groups, whereas 6% had major complications. No perioperative or 30-day mortalities were observed. In total, 49% of patients had complete resolution of symptoms, 46% had partial improvement, and 5% had no improvement. There was no difference in symptom resolution between either group.
Conclusions:
TA and SC approaches are equally safe and effective for the treatment of TOS. SC decompression allows for adjunct procedures and vascular reconstructions.
Introduction
Thoracic outlet syndrome (TOS) is described as a group of symptoms resulting from compression of the neurovascular structures supplying the upper extremity as they exit through the thoracic outlet. 1 It comprises three distinct conditions depending on the affected structures. These include the neurogenic, venous, and arterial TOS (aTOS). Neurogenic TOS (nTOS) involves the brachial plexus and is by far the most common form of TOS affecting >90% of patients. Venous TOS (vTOS) and aTOS are seen in 5 and 1%–2% of patients with TOS, and affect the subclavian vein and artery, respectively. 2
The most initial diagnosis of TOS is clinical, based on a detailed history and physical examination. The diagnostic workup depends on the involvement of each component of the neurovascular bundle at the thoracic outlet. Arterial and venous duplex ultrasound may be initially performed upon clinical suspicion. Cross-sectional imaging through computed tomography or magnetic resonance angiography is tailored to evaluate the vasculature of the chest and upper extremity. It is also performed to identify any possible underlying causes of compression that include but are not limited to compression from first rib and accessory or cervical ribs, anomalous cervical bands from an elongated cervical transverse processes, hypertrophic scalene and subclavius muscles and their corresponding tendons, and neck trauma. 3 Arteriography and venography are recommended for confirmation of diagnosis and initiation of catheter-directed thrombolysis and mechanical thrombectomy, when indicated. The diagnosis of nTOS is more complex. Cross sectional imaging is used to identify possible intrinsic brachial plexus pathologies and, as previously mentioned, any causes of underlying compression. Staged scalene and pectoralis minor blocks confirmed diagnosis and provide information regarding outcomes after thoracic outlet decompression. Although physical therapy with dedicated postural exercises is considered the first line of treatment for neurogenic TOS, patients with severe or recurrent symptoms may require surgical decompression with removal of the first rib. 4
The two common surgical approaches for first rib resection include the transaxillary (TA) and supraclavicular (SC) approaches with each having its own pros and cons with regard to area exposure, extent of rib resection, and performance of adjunct procedures when needed. 5 Both approaches have been shown to result in effective thoracic outlet decompression and symptom resolution with low complication rates. 6 Since both TA and SC are practiced in our institution, the aim of this study was to analyze the short- and long-term outcomes of both approaches utilizing our institutional database.
Methods
Patient population
A retrospective chart review of patients who underwent surgical decompression for TOS between January 2010 and June 2015 at the University of Iowa Hospital and Clinics was performed. All patients had undergone a full workup for TOS and the indications for surgery were failure of conservative treatment, worsening symptoms despite physical therapy, and radiologic evidence of vascular compression or compromise. Only patients with at least 6 months of follow-up were included. Data on demographics, comorbidities, presenting symptoms, and type of TOS (neurogenic, venous, or arterial) were documented. Operative times, length of hospital stay, perioperative complications, and outcomes were also collected from patients' charts. Minor complications were those that were managed conservatively and did not require interventions. These included small hematomas or collections, superficial surgical site infection, and small pneumothoraces. Large collections requiring drainage, bleeding requiring re-exploration, major nerve or thoracic duct injury, pneumothorax requiring thoracostomy, and any complication requiring readmission within 30 days were considered as major complications. Data on symptom resolution were collected by reviewing outpatient records and by contacting patients directly when needed. Complete resolution was defined as no residual symptoms pertaining to thoracic outlet compression on follow-up visits. Patients who reported improvement in their initial symptoms but without complete resolution were labeled as having partial improvement. Patients with no improvement were those with no change in their symptoms after decompression.
Statistical analyses
Demographic and clinical variables were described utilizing simple summary statistics; categorical and continuous variables of interest were analyzed with chi-square/Fisher's exact test, and student's-t/Mann–Whitney test, based on sample size. Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) software (version 23.0; SPSS, Inc., Chicago, IL); all tests were two sided, and a P-value <.05 was set for statistical significance. This study was granted approval from the institutional review board.
Results
A total of 82 thoracic outlet decompression procedures were identified in our database. The male to female ratio was 36/46. There were no significant demographic or comorbidity differences between the two groups. Forty-two percent (n = 34) of procedures were done for neurogenic TOS, 46% (n = 38) for vTOS, and 12% (n = 8) for aTOS. Forty-nine percent (n = 40) of the patients underwent TA approach and 51% (n = 42) underwent an SC approach. Adjunct procedures in addition to decompression were performed in 13% of the patients, who all underwent SC decompression. These included neurolysis, venolysis, vascular reconstruction, or bypass and intraoperative angiography/angioplasty. There were no significant differences in average operative time (126.1 ± 36.1 versus 131.3 ± 34.1, P = .11) or length of hospital stay (2.3 ± 1.9 versus 2.4 ± 1.4, P = .23) between the TA and SC groups, respectively (Table 1).
Demographics, Comorbidities, and Perioperative Characteristics of the Study Population
LOS, length of stay; OR, operative room; SC, supraclavicular; SD, standard deviation; TA, transaxillary; TOS, thoracic outlet syndrome.
Minor complications were seen in 6% (n = 5) of patients with no significant difference in both groups. These included three minor hematomas/seromas, one small apical pneumothorax, and one upper extremity partial deep venous thrombosis. Six percent (n = 5) had major complications that were 3 cases of large hemo/pneumothorax, 1 thoracic duct injury, and 1 case of pneumonia that necessitated readmission. In total, 4 patients required re-exploration (3 TA and 1 SC). There were no perioperative or 30-day mortalities.
On follow-up, 49% (n = 40) of patients had complete resolution of symptoms, 46% (n = 38) had partial improvement, and 5% (n = 4) had no improvement with an average follow-up time of 7.9 ± 1.6 months. There was no difference in symptom resolution based on the type of procedure performed (Fig. 1). Symptoms resolution was also compared based on the type of TOS involved. In patients with nTOS (n = 34), 32% (n = 11) had complete resolution, 56% (n = 19) had partial improvement, and 12% (n = 4) had no improvement. All patients in the vTOS and aTOS, on the other hand, had some degree of improvement noted. With vTOS (n = 38), 61% (n = 23) had complete resolution and 39% (n = 15) had partial improvement, whereas in the aTOS group (n = 8), 75% (n = 6) had complete resolution and 25% (n = 2) had partial improvement. The difference between the nTOS group and the other two groups was statistically significant (P = .03, Fig. 1).
Discussion
This study analyzes a single institutional experience with surgical decompression for TOS, comparing TA versus SC approach. We identified no significant differences in average operative time, length of hospital stay, and resolution of symptoms. Also, no perioperative or 30-day mortalities were observed in the entire cohort.
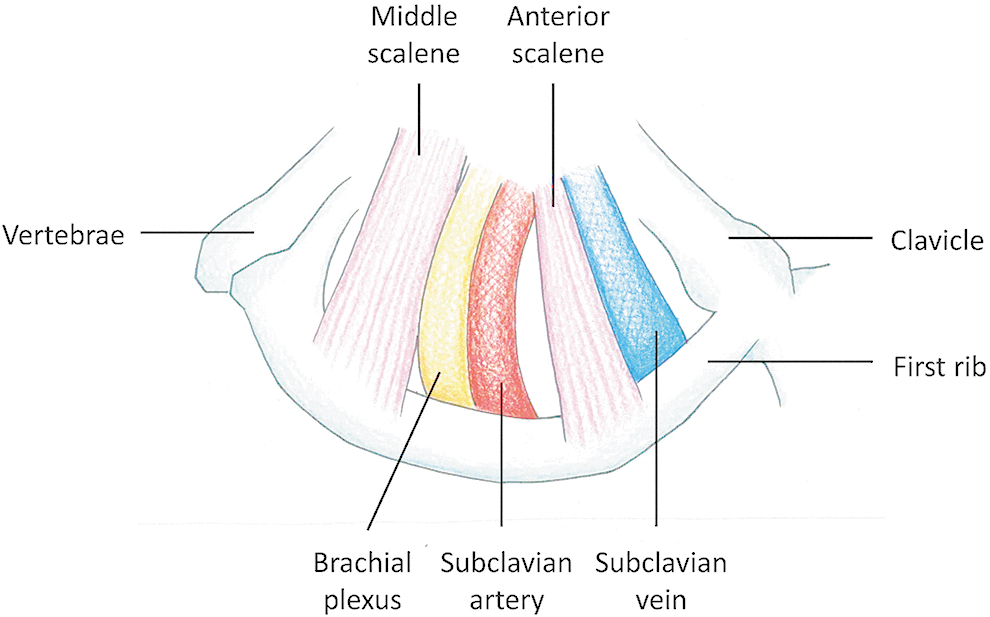
TOS generally refers to pathologic compression of the neurovascular structures supplying the upper extremity as they pass between the clavicle and the first rib. It can be differentiated clinically into different categories depending on whether it affects the brachial plexus, subclavian vein, subclavian artery, or a combination of these structures. The underlying etiology can vary from accessory or cervical ribs, anomalous cervical bands, hypertrophic scalene, and subclavius muscles to repetitive stress and neck trauma. 7 Anatomically, there are three pertinent “spaces” through which these structures pass that are pertinent to the thoracic outlet pathology, especially when considering surgical decompression (Fig. 2). The scalene triangle is bound by the first rib, anterior scalene muscle, and middle scalene muscle through which the brachial plexus and subclavian artery run. This triangle is, therefore, one of the principal sites for nerve and blood vessel compression implicated in TOS. The costoclavicular space, in contrast, is made up by the clavicle and cartilaginous insertion of the first rib into the sternum as well as the subclavius muscle and the costoclavicular ligament on the undersurface of the clavicle. Narrowing in this space typically affects the subclavian vein. Finally, the subpectoralis space is the area formed underneath the pectoralis minor tendon as it attaches to the coracoid process and is another site for potential neurovascular compression in TOS.8,9 Although the diagnosis of TOS is clinical, a comprehensive workup is typically performed to identify the type and extent of the pathology and this includes provocative maneuvers, imaging, noninvasive vascular laboratory studies, and electromagnetic testing. 10 Surgical decompression is reserved for patients with confirmed TOS with recurrent or worsening symptoms or those who have failed to improve with physical therapy. Both the TA and SC approaches have been effectively utilized for surgical decompression and first rib resection. TA approach (Fig. 3) is ideal for exposure of the anterior first rib and freeing compressive structures from around the subclavian vein, but the limited exposure may not allow for complete resection of the entire posterior portion of the first rib. SC approach, in contrast, provides the best exposure of the scalene triangle and the roots and trunks of the brachial plexus and allows for resection of the anterior and middle scalene muscles as well as cervical ribs and the posterior part of the first rib. 11 It may be difficult to achieve complete resection of the anterior posterior portion of the first rib without an additional infraclavicular incision.

Anatomical illustration of the thoracic outlet.
Anatomic view of the thoracic outlet through a transaxillary approach.
There are multiple published series documenting the safety and effectiveness of both approaches. Maxwell-Armstrong et al. published their data on 126 SC procedures for TOS decompression and described improvement and/or resolution of symptoms in 86.5% of patients at 6 weeks. Their reported complication rate was 11% and mean duration of hospital stay was 2.1 days. 12 Another series by König et al. describing 50 SC decompressions showed 80% improvement in symptoms at 24 months with a complication rate of 4%. 13 These results are comparable with our study population in which 95% of patients who underwent SC had partial or complete resolution of their symptoms with a mean hospital stay of 2.4 days and a combined complication rate of 12%. One of the largest series on SC decompression was published by Hempel et al. on 770 procedures. In this study, significant improvement was noted in 86% of patients with an impressive complication rate of 2%, further validating the safety and efficacy of this approach. 14 Series published on the TA approach also show excellent results. Karamustafaoglu et al. reported on 131 TA procedures in 109 patients with TOS with a favorable outcome seen in 95.4% of patients. Their complication rate was 28.4% although most of these were due to apical pneumothoraces (24.6%). 15 Another series of 40 TA procedures documented improvement of symptoms in 97% of patients, although the complication rate was not reported. 16 These results are also comparable with our series of 40 patients who underwent TA, in which improvement was seen in 95% of cases and the complication rate was 12.5%. Only 7.5% of patients had a major complication, requiring re-exploration.
Studies comparing both approaches are scarce. However, in a series of 668 cases, Sanders and Pearce performed a retrospective review comparing the results of 111 patients who underwent TA first rib resection with 279 patients undergoing anterior and middle scalenectomy and 278 SC first rib resections with scalenectomy. There were no major differences between the three groups with significant improvement at 3 months seen in 91%, 93%, and 92% of patients, respectively. 17 A randomized trial comparing 24 TA and 25 SC procedures in patients with nTOS and arm pain, however, reported better relief of symptoms in the TA group. In that study, pain relief was seen in 75% of TA patients compared with 48% in the SC group. 18 Nevertheless, the small number of patients and inclusion of nTOS only preclude generalization of these results. Our results showed no significant difference between the two groups with respect to operative times, perioperative complications, length of hospital stay, and symptom resolution. However, the exposure demonstrated by an SC incision appears to allow for more surgical options, especially when adjunct procedures, such as neurolysis and vascular reconstruction, are required. This is confirmed by the fact that the 13% of patients who underwent adjunct procedures in addition to decompression in our study all belonged to the SC group.
Interestingly, when comparing symptom improvement based on the type of TOS rather than the surgical procedure, it was noted those with nTOS tend to have worse outcomes compared with those with vTOS and aTOS. Indeed, in the nTOS group, 32% had complete resolution, 56% had partial improvement, and 12% had no improvement, whereas in vTOS and aTOS groups, complete resolution was seen in 61% and 75% and partial improvement seen in 39% and 25%, respectively. This highlights the difficulty in diagnosing true nTOS and identifying those who would truly benefit from surgical decompression. In one study of 409 patients with nTOS, 21% had complete relief postoperatively, 32% had good relief, 25% had fair relief, and 22% showed no improvement. 19 These results further emphasize the importance of proper diagnosis that remains the most debated and challenging aspect of nTOS. Despite multiple maneuvers and studies, the test results still rely mostly on patient symptoms. 20
We recognize that our study has its limitations mainly pertaining to its retrospective design and relatively small number of patients. In addition, since it includes all three forms of TOS, all of which have their own workup and indications for intervention with no standardized approach, the results are not generalized to cover all TOS cases. Moreover, the analysis of symptom resolution postoperatively was based on patients' subjective input rather than a standardized questionnaire. Although this allowed for the possibility of over- or underestimation of the impact of surgical decompression, it would be expected to affect both the TA and SC groups in a similar proportion. Finally, as the procedures were performed by different surgeons, there was no standardized operative technique in regard to the surgical technique and the postoperative management.
Conclusions
Although diagnosis of TOS remains challenging, both TA and SC approaches for surgical decompression appear to be safe and effective in most patients with comparable perioperative complications, length of stay, and improvement of symptoms. Although either approach has its advantages, SC decompression should be considered when adjunct procedures and vascular reconstructions are contemplated.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.