
Abstract
Introduction:
Abdominal wall complications are one of the most controversial issues regarding single-incision endoscopic surgery. The aim of this study was to analyze the incidence and risk factors of incisional hernia after single-incision endoscopic cholecystectomy.
Materials and Methods:
An observational retrospective study was performed, on a cohort of patients cholecystectomized laparoscopically through a transumbilical single incision due to gallbladder lithiasis or polyps. Postoperative complications were analyzed, with special interest in the incisional hernia rate, whose results were assessed in the long-term follow-up. Univariate and multivariate analyses were also performed to evaluate possible variables associated with the appearance of incisional hernia. Cumulative sum charts (CUSUM) were used to identify trends in the incisional hernia risk.
Results:
Some 109 patients were included in the study. With a mean follow-up of nearly 38 months, an incisional hernia incidence of 5.5% was found, with 67% being diagnosed during the first year of follow-up. In the Cox regression analysis, two variables showed an independent association with the emergence of incisional hernia, body mass index (hazard ratio [HR] 1.30; 95% confidence interval [CI 1.053–1.606]; P .015), and wound infection (HR 26.32; [3.186–217.40]; P .002]. CUSUM charts showed a decrease in the risk of incisional hernia after the first 10 cases.
Conclusions:
Single-incision endoscopic cholecystectomy is associated with a substantially high risk of postoperative incisional hernia (5.5%).
Introduction
Single-incision endoscopic surgery (SIES) emerged as a safe technique that achieves similar results to those of the multiport approach. Its main advantage is the need for a single incision compared to the multiple incisions of the conventional laparoscopic approach, with potential benefits in postoperative pain and the aesthetic result.1–3 However, the lack of high-level evidence and the lack of long-term results make it difficult to justify strong recommendations on this topic. 4
Abdominal wall complications are one of the most controversial issues regarding this surgical technique; as the need of a longer incision located in an area of parietal weakness, such as the umbilical region, could be related with an increase in the rate of seroma, wound infection, wound hematoma, and incisional hernia. After SIES, the incidence of incisional hernia varies from 1% to 8.4% in different studies2,5–7; however, most of them have not been designed to evaluate this end-point primarily and the follow-up after surgery has been shorter than a year. This late complication has been usually related to the wound closure technique and the existence of postoperative wound complications by some authors.2,8,9
The aim of this study was to evaluate the incidence of incisional hernia after SIES in a cohort of patients with a long-term follow-up, and to analyze the potential risk factors that influence its development.
Materials and Methods
An observational, analytic, longitudinal, retrospective study was performed on a cohort of patients operated on using the single-incision laparoscopic cholecystectomy technique, between January 2009 and December 2011, due to symptomatic cholelithiasis or gallbladder polyps. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Three surgeons performed all the procedures, all the three were with extensive experience in laparoscopic cholecystectomy (more than 300 cases). This series includes the initial experience of the group for single-incision laparoscopic cholecystectomy. The SILSTM Port device (Covidien; Autosuture, Hamilton, Bermuda) or the TriPortTM device (Olympus, Center Valley, PA) was placed through a transumbilical incision of about 2–2.5 cm. The surgeons utilized a combination of one straight and one curved/articulating instrument to complete the cholecystectomy, being the gallbladder fundus retracted by means of a transparietal suture, a 3 mm epigastric grasper, or the use of a grasper trough an accessory forth port in the single-incision device. The aponeurosis at the umbilical level was closed using three to four interrupted stitches at a distance of 0.5 cm. Synthetic long-term absorbable monofilament suture was used.
After discharge from hospital, patients were monitored for at least 1 year in the medical office. Patients who did not have entries in their clinical record, beyond the first year of follow-up, were contacted by telephone. Besides, appointments for further examination were arranged if an incisional hernia was suspected, followed by image test (ultrasound or abdominal computer tomography) in case of doubt.
Patient demographics, medical history, operative time, conversion rate, and postoperative complications were recorded and graded according to Clavien-Dindo classification.10,11 Regarding to the early complications of the surgical incision, we studied the presence of seroma, defined as the accumulation of serum in the subcutaneous cellular tissue and superficial surgical site infection defined as the infection at the site of the incision that affects only the skin and subcutaneous tissue and that occurs in the first 30 days after the operation. 12 Trocar site incisional hernia was defined as the presence of a hernia in the periumbilical incision area.
Statistical analysis
A descriptive analysis of the variables included in the study was performed. The qualitative variables were summarized with relative and absolute frequencies and the quantitative variables were summarized with measures of central tendency and dispersion according to the distribution of the variable determined by the Kolmogorov-Smirnov test.
The risk of umbilical incisional hernia over time was estimated and represented with risk function curves. A Cox regression model was used to identify the associated variables in the emergence of umbilical incisional hernia with the moment it appears. Hazard ratios (HRs) were calculated with their 95% confidence intervals (95% CIs). Finally, cumulative sum charts (CUSUM) were used to identify trends in the incisional hernia risk over time. For the statistical analysis, the SPSSv18® (SPSS Inc. Released 2009. PASW Statistics for Windows, Version 18.0. Chicago: SPSS Inc.) and STATA/ICv15® software (STATA, College Station, Texas) were used. A value of P < .05 was established as significant.
Results
Some 109 patients were included in this study. The female gender was predominant (77%), mean body mass index (BMI) was 26.69 ± 3.84, and most frequent comorbidities were hypertension (25%) and diabetes mellitus (6%). Seven patients (6%) had a history of previous acute pancreatitis and eight (7%) required an endoscopic retrograde cholangiopancreatography before cholecystectomy. Ten patients (9%) presented with an umbilical hernia which was repaired at the moment of the cholecystectomy. The baseline characteristics of the patients, as well as their clinical features, are described in Table 1.
Demographic and Clinical Characteristics of Included Patients
Mean (standard deviation).
ASA, American Society of Anesthesiologists physical status classification); BMI, body mass index; COPD, chronic obstructive pulmonary disease; N, no; SILS, single-incision laparoscopic surgery; Y, yes.
Technical details and its evolution from the first single-incision laparoscopic cholecystectomy performed at our center are summarized in Figure 1. Mean operative time was 72.26 ± 19.4 minutes. There were no conversions to laparotomy, although 10 patients (9.2%) required conversion to multiport laparoscopic surgery. The most common reason for conversion was the difficulty in dissecting the cystic elements, followed by bleeding. Nearly half of the patients (48%) were operated on in the day surgery unit, with a mean hospital stay of 24.3 ± 16.2 hours in the entire series.
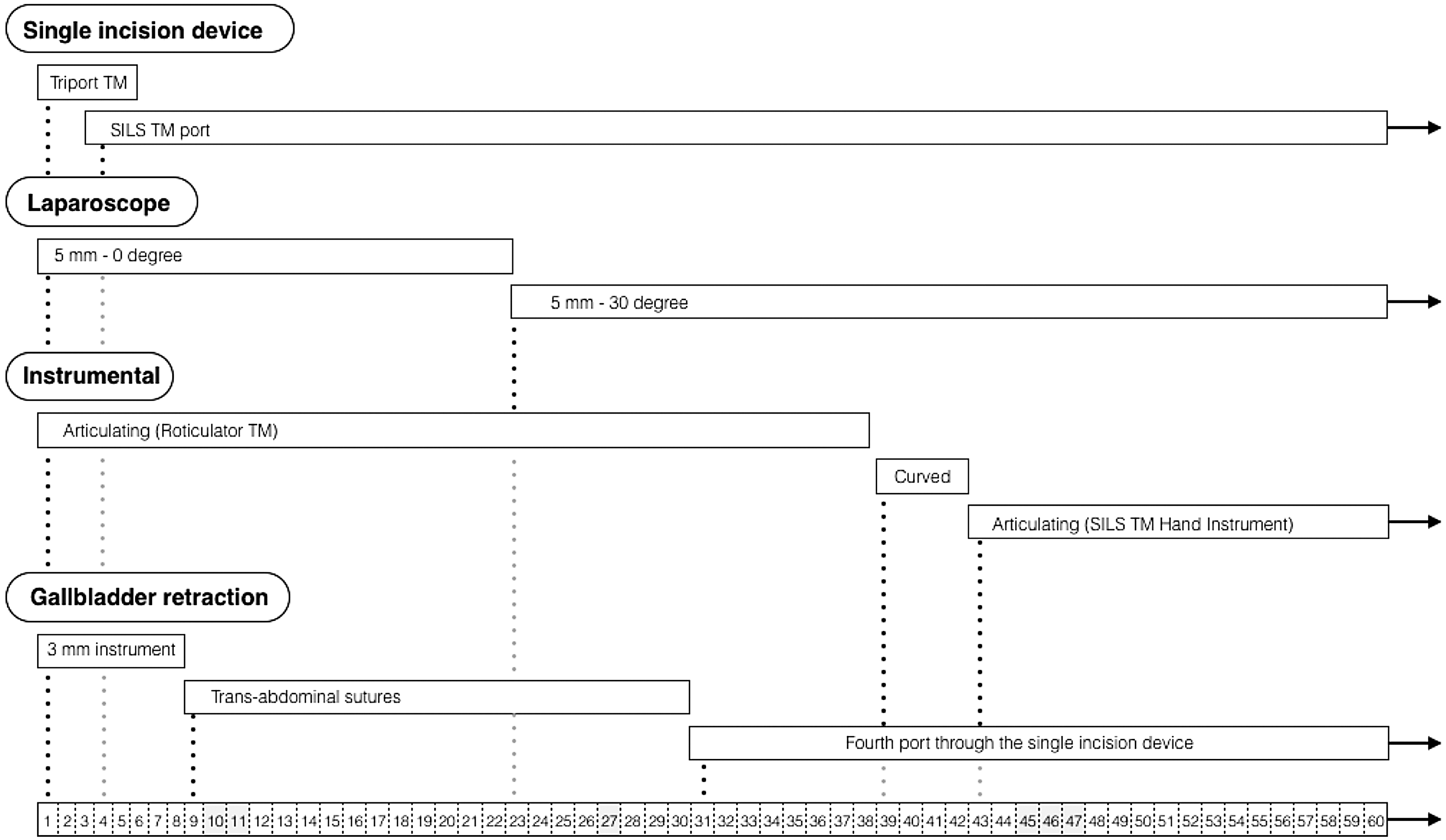
Technical details and its evolution during the implementation of the single-incision laparoscopic cholecystectomy technique.
There were no biliary duct injuries or medical complications in any patient. Regarding acute wound complications, seroma occurred in 17 patients (16%) and wound infection in 8 (7%), all of them were resolved with conservative management (Clavien-Dindo grade I). One patient, who had concomitant cholecystectomy and simple liver cyst fenestration, was reoperated on due to postoperative bleeding at the fenestrated hepatic edges (Clavien-Dindo IIIB). No cases of death were recorded.
Umbilical incisional hernia
With a mean follow-up of 37.6 ± 23.6 months, the overall rate of umbilical incisional hernia in our study was 5.5%, with 67% being diagnosed during the first year of follow-up (Fig. 2). Subsequently, a Cox regression model was applied to identify those risk factors related to the development of umbilical trocar incisional hernia and its relationship with the time to the onset of symptoms. First, a univariate analysis was introduced comparing patients who had an incisional hernia and those who did not, in which surgical site infection was the only variable that reached statistical significance, being BMI and obstructive pulmonary disease very close to significance. These variables and other variables that were considered to be of clinical importance such as gender, age, diabetes mellitus, chronic corticosteroid intake, umbilical hernia, smoking, previous biliary pathology, operative time, and wound seroma were included in the Cox regression model. Finally, two variables showed an independent association with the emergence of incisional hernia: BMI (HR 1.30, 95% CI [1.053–1.606], P .015) and wound infection (HR 26.32, [3.186–217.40], P .002). When evaluating the risk of incisional hernia along this series of patients, the CUSUM charts showed an increased risk in ∼10 cases, after which a decrease in the risk was observed (Fig. 3).
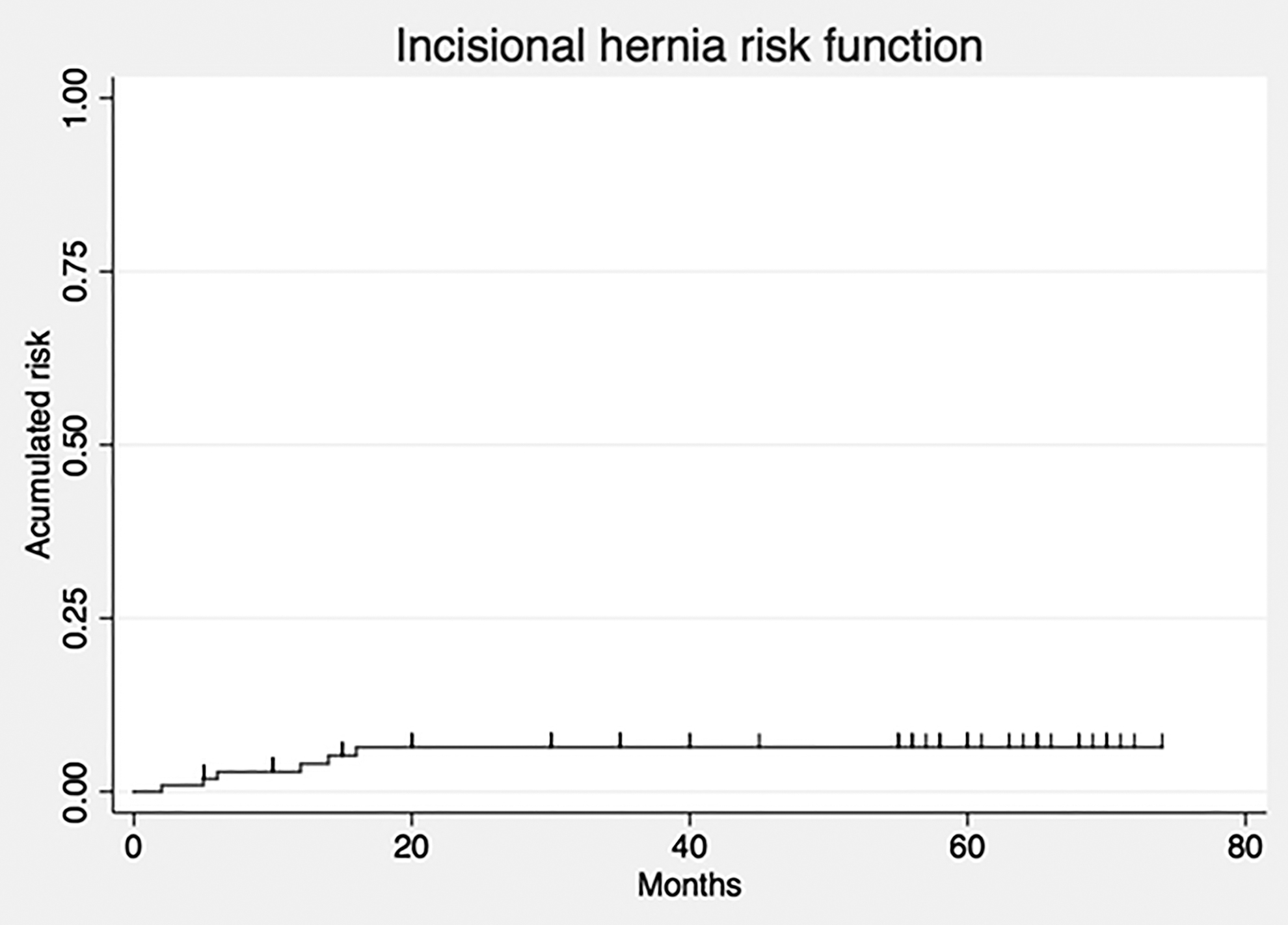
Incisional hernia risk function.
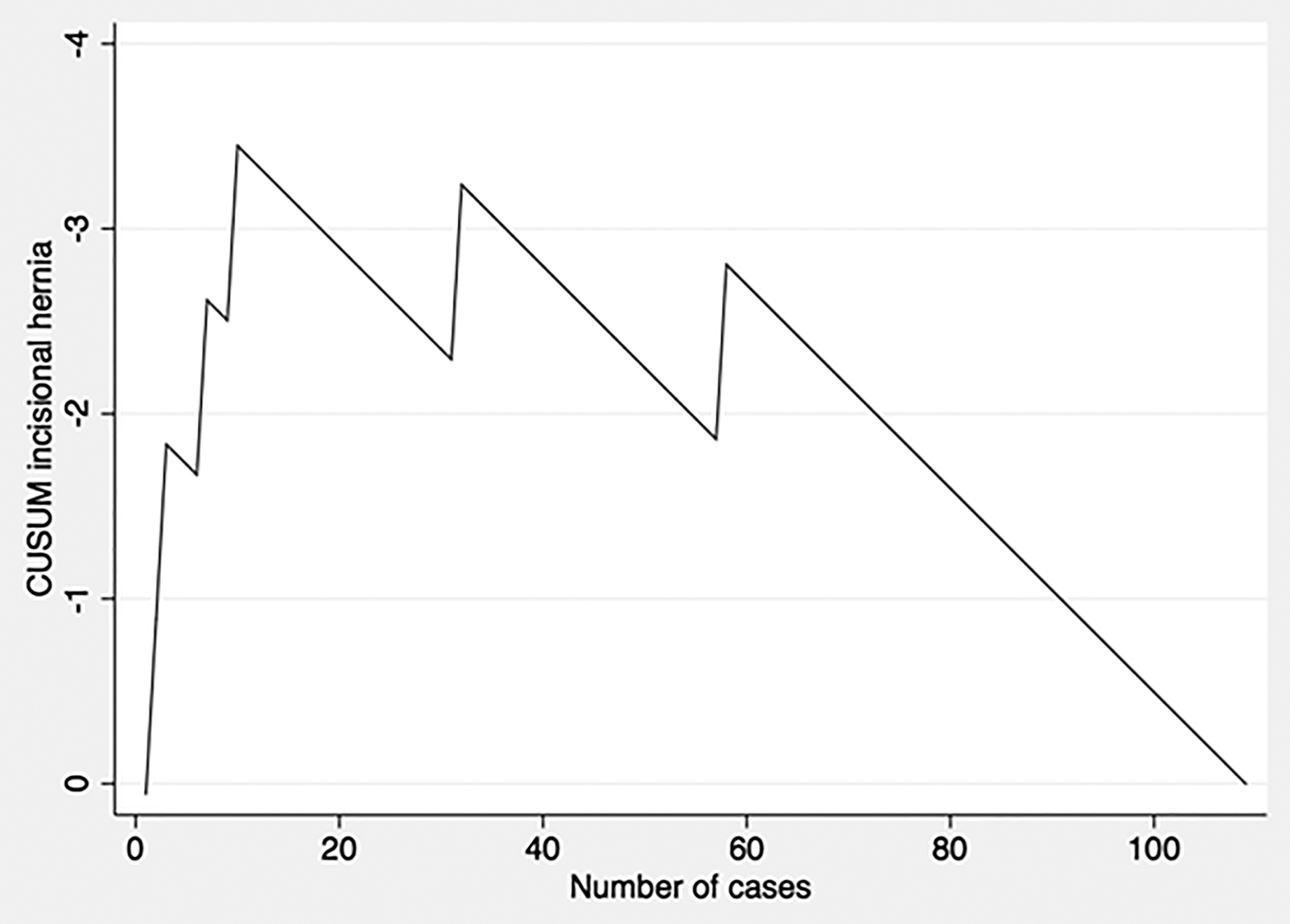
CUSUM incisional hernia. CUSUM, cumulative sum charts.
Discussion
Abdominal wall complications after minimally invasive surgery are currently discussed as an underestimated problem. Some of them, such as seroma, hematoma, or superficial surgical site infection are common but cause little discomfort to the patient, being usually resolved in a short period of time by means of conservative management. Special mention should be given to trocar site hernias, a complication that may require a new operation. Patient and surgery related risk factors can influence the development of these complications. 13
With the objective of reducing trauma to the abdominal wall, a series of access reduction techniques have emerged, among which is SIES. 14 Incisional hernia rate has been the subject of great interest since the conception of this minimally invasive approach, as it is hypothesized that a larger incision and localized at the umbilical level could increase the rate of hernias. This rate varies between 1% and 8.4%, although in recent studies, incidences as high as 21.4% have been reported.6,7,15–21 However, a considerable variability in the follow-up time is found among studies reporting incisional hernia rate after SIES (Table 2). In our study, with a mean follow-up of nearly 38 months, incisional hernia rate was 5.5%, which is in line with some of above mentioned studies.
Studies Reporting Incisional Hernia Rates After Single-Incision Laparoscopic Cholecystectomy, with a Minimum Follow-Up of Twelve Months
BMI, body mass index; n/a, not available; PDS, polydioxanone suture; SILS, single-incision laparoscopic surgery; SSI, surgical site infection.
Marks et al. 7 have compared the incisional hernia rate between single-incision and multiport laparoscopic cholecystectomy 3 months after surgery, but no statistically significant differences were found. In contrast, differences were found when follow-up was extended to 1 year, with a trocar hernia incidence of 8.4% in the single-incision group and 1.2% in the multiport group. 7 Moreover, two recently published meta-analyses describe an increased risk of incisional hernia in the single-incision group, with the authors highlighting, in addition to the variability in follow-up, a significant heterogeneity in the technique and material used in the closure of the trocars.2,22
Different factors have been associated with an increased incidence of umbilical trocar incisional hernia in patients undergoing laparoscopic cholecystectomy, among them are diabetes mellitus, obesity, incision length, and surgical site infection.9,13 More specifically, in the case of single-incision cholecystectomy, Marks et al. found that wound infection was the only predictive variable associated with a higher incisional hernia incidence. 7 These results are in accordance with our findings, with wound infection being also the variable associated with the greatest increase in the risk of umbilical incisional hernia, as nearly 33% of the patients who suffered a surgical site infection in our study developed a hernia. In addition, we observed a discreet increase in the risk of incisional hernia with the increase in BMI. Similar results were described by Julliard et al. 18 in a multivariate analysis of a cohort of 82 patients, where they found BMI and age older than 50 years as independent predictive factors of developing an incisional hernia after SIES cholecystectomy.
Surgical technique can also influence the emergence of incisional hernia. In our study, a trend toward a reduction in the risk of incisional hernia was observed after the first cases, probably due to the inclusion of patients during the learning curve, in which the periumbilical subcutaneous tissue was widely dissected and the skin closure was performed hermetically with a continuous intradermal suture. Other authors have also found a higher rate of wound infections during the SIES learning curve, although not related with an increase in the incisional hernia risk. 23 Taking all this into account, it is worth to mention the importance of small details, such as wound management, during the development and implementation of surgical innovation.
This study has a series of limitations, including its retrospective nature, the inclusion of the single-incision learning curve and the use of telephone interviews to extend follow-up time in some patients. On the contrary, long-term follow-up with few losses during the first 2 years give greater validity to our results.
Finally, we can conclude that single-incision endoscopic cholecystectomy is accompanied by a substantially high incisional hernia rate in the mid–long-term follow-up. Wound complications, including incisional hernia, should be considered during development and implementation of innovations in the field of abdominal minimally invasive surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.