
Abstract
Purpose:
Many laparoscopic repair techniques are available for treating pediatric inguinal hernias. The development of a cord hydrocele (CH) after laparoscopic pediatric inguinal hernia repair (LPIHR) in male patients can lead to reoperation. We performed the present study to evaluate the effects of hernial sac removal on the occurrence of CH after laparoscopic transabdominal inguinal hernia repair in male patients.
Materials and Methods:
This retrospective study included 3145 male pediatric patients aged <10 years who underwent LPIHR from January 2014 to March 2017. We categorized patients into two groups according to the operative technique: Group 1 (high ligation without hernial sac removal, 1592 patients) and Group 2 (high ligation with hernial sac removal, 1553 patients). We removed the hernial sacs in the first half of the study period and not in the second half of the study period. We analyzed the surgical outcomes in both groups after the same follow-up period of ≥2.5 years.
Results:
We found no significant differences in demographic or clinical parameters between the treatment groups. CH occurred in 6 patients in Group 1 only; no patients in Group 2 developed CH (0.38% [6/1592] versus 0.00% [0/1553], respectively; P = .044). The interval from the initial hernia repair to the hydrocelectomy in 6 patients was 20.8 months. The recurrence rate was higher in Group 1 (0.4%, 7/1592) versus Group 2 (0.0%, 0/1553) (P = .025). In the logistic regression test, Group 2 predicted a lower CH occurrence rate than Group 1 (odds ratio = 1.004, 95% confidence interval = 1.001–1.007; P = .016).
Conclusion:
Our findings indicated that hernial sac removal resulted in a small but significant decrease in the risk of postoperative CH.
Introduction
Inguinal hernia is one of the most common pediatric diseases requiring surgical correction, and performing laparoscopic pediatric inguinal hernia repair (LPIHR) has become widespread in pediatric surgery. Although complications following LPIHR are rare, recurrence and cord hydroceles (CHs) occur in some patients. The incidence of hernia recurrence after LPIHR reportedly ranges from 0.0% to 2.6%.1,2 Among patients who underwent reoperations after LPIHR, hydroceles were the reported cause of reoperation in 39.2% (20/51) of patients who underwent laparoscopic transabdominal closure (LTAC) 3 and in 42.8% (9/21) of those who underwent laparoscopic percutaneous extraperitoneal closure (LPEC). 4
We previously reported that of 16/38 boys who underwent reoperation for concurrent hydrocele, none underwent hernial sac removal at the initial surgery. 3 CH and hernia recurrence are causes of reoperation,1,3,4 which involve two widely published surgical methods of LPIHR: LTAC and LPEC.5,6 Several reports have described the results of primary laparoscopic surgery for pediatric inguinal hernia7,8; the present study focused on LTAC. Generally, surgical treatment is indicated when pediatric patients with CH are older than 18 months of age.9,10
One of the reasons for performing the present study was that despite the increasing use of laparoscopic techniques to repair inguinal hernia in infants and children, data on the optimal methods are scarce, and procedural guidelines remain unclear. Although the need for reoperation is rare, a second surgery entails surgical and anesthetic risks and increased medical costs and thus should be avoided whenever possible. We performed the present study to evaluate the effect of hernial sac removal on the incidence of CH after laparoscopic inguinal hernia repair in pediatric patients.
Materials and Methods
This retrospective study included male pediatric patients who underwent LTAC at Damsoyu Hospital, Seoul, Republic of Korea, from January 2014 to March 2017. Inclusion criteria were male pediatric inguinal hernia patients; we excluded female pediatric patients from the study. We also excluded patients with <2.5 years of follow-up, those with cryptorchidism, and those with a hydrocele at the time of the initial surgery. Five patients were excluded from the study because of follow-up failure. From January 2014 to July 2015, 1592 children underwent LTAC without hernial sac removal (Group 1), and from August 2015 to March 2017, 1553 children underwent LTAC with hernial sac removal (Group 2). Before comparing the two groups, we used the G-power software program to derive the sample size required to provide a power of 0.8 at the medium effect size and a significance level of 0.05. The results showed that a sample size of 106 patients was needed for the Wilcoxon–Mann–Whitney test, and we selected a larger sample to perform this experiment. We recorded patients' characteristics, operative findings, and outcomes from their medical records, which we reviewed retrospectively. The cause of reoperation was divided into two types: hernia recurrence (Fig. 1a) and hydrocele occurrence (Fig. 1b). Fluid extracted by needle aspiration was classified as a seroma, and a communicating hydrocele was classified as recurrence. In this study, we included hydrocele only when a CH occurred with a closed internal ring, and we confirmed the diagnosis of CH by ultrasonography. After 1 month of follow-up, we performed hydrocelectomy due to self-limiting failure. Reoperation was performed in children older than 2 years of age who had symptoms or increased size in a newly developed CH after hernia. Routine follow-ups were performed 1 month postoperatively and annually.

Cases of reoperation.
Surgical procedure
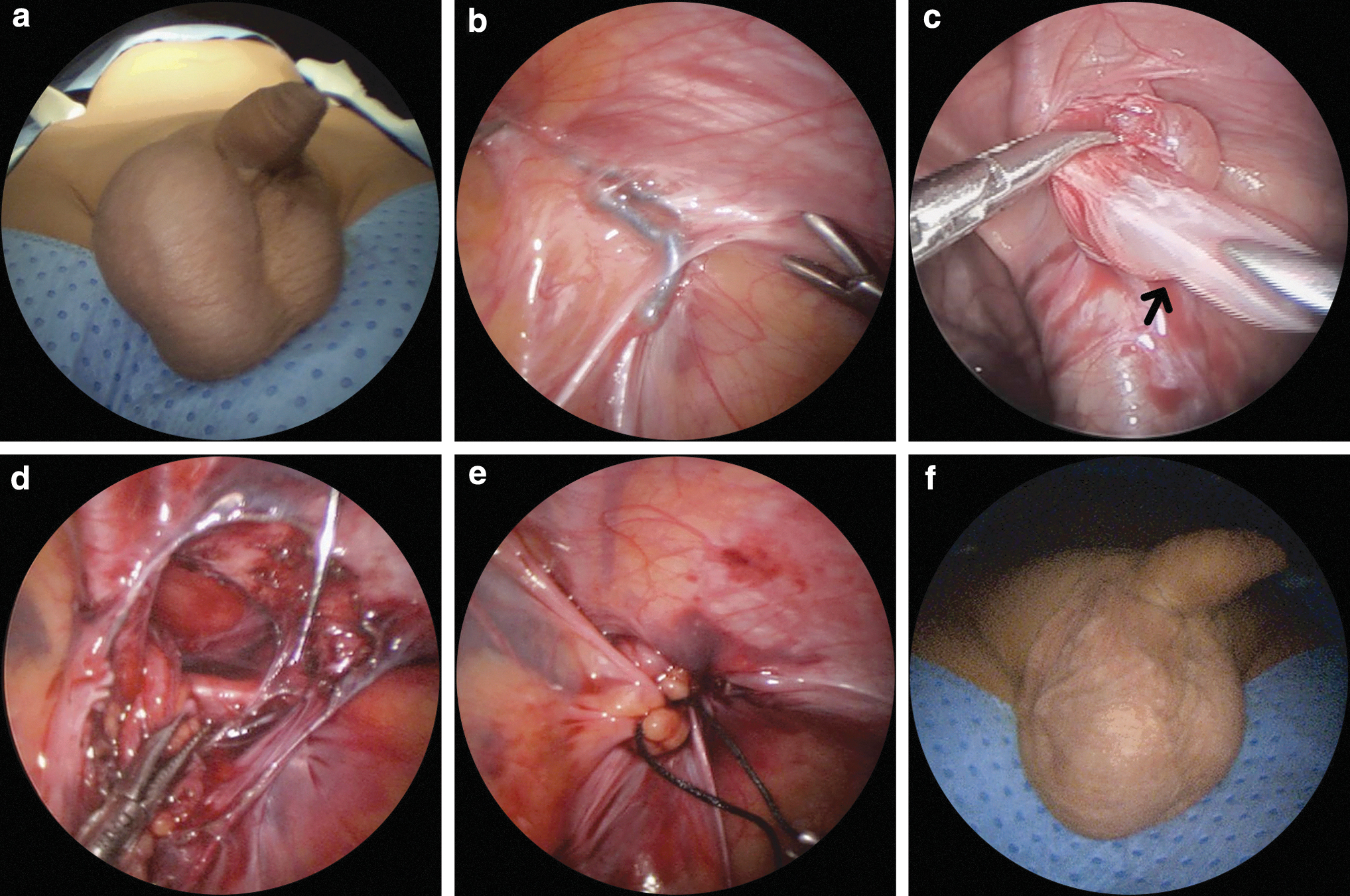
We used previously published techniques in Group 111 and Group 2. 3 The surgical methods were identical in both groups with the exception of whether the sac was removed. A nonabsorbable silk 3-0 suture was used as the suture material, and a multiple-suture linear suture technique was used for the high ligation method in both groups. All operations were performed by a single surgeon under general anesthesia with patients in the supine position. LTAC was performed using a three-port technique with high ligation. The laparoscopic system contained a 2.9-mm camera and 2.7-mm instruments. We used a 3-mm transumbilical incision to establish pneumoperitoneum via a 3-mm trocar, and carbon dioxide pneumoperitoneum was maintained at 5–8 mmHg. We inserted two additional 2.7-mm instruments through a separate incision in the lateral abdomen and performed the iliopubic tract suture technique using nonabsorbable 3-0 silk, as previously reported3,11; the procedures are shown in Figure 2. In the high ligation without hernial sac removal group, we placed multiple linear sutures at the internal inguinal ring with the hernial sac remaining intact (Fig. 2a). In the high ligation with hernial sac removal group, we used the same suture technique after removing the hernial sac (Fig. 2b). We then examined the patency of the contralateral processus vaginalis and simultaneously repaired the open canal. Skin adhesive was used to cover the scar; therefore, no dressing was required after discharge.

Surgical procedure involving high ligation of the internal ring.
We performed reoperation because of hydrocele occurrence as for the initial LTAC method with general anesthesia and a three-port laparoscopic operation. The intracorporeal hydrocelectomy technique was described previously, 12 and the procedures are shown in Figure 3.
Surgical procedure involving laparoscopic intracorporeal hydrocelectomy in a patient with hydrocele occurrence after laparoscopic hernia repair.
Statistical methods
All statistical analyses were performed using R software ver. 3.6.1 (R Development Core Team, Vienna, Austria). Continuous variables are presented as mean and range, whereas categorical variables are presented as frequency and percentage. We used Wilcoxon's rank-sum test to test for normality of continuous variables and Fisher's exact test or the χ 2 test for categorical variables. We chose a P-value threshold of .05, and any univariate P ≤ .05 was considered statistically significant. Finally, we calculated the odds ratios using Fisher's exact test and logistic regression.
Results
Table 1 shows the clinical characteristics of the patients in Groups 1 and 2. A total of 3150 male pediatric patients with inguinal hernias underwent LTAC, and we excluded 5 patients from the study because of follow-up loss, leaving 3145 patients for inclusion. The mean operation time was different between the two groups (12.8 versus 14.9 minutes, Group 1 versus Group 2, respectively; P < .000). The occurrence of CH was higher in Group 1 (0.4%, 6/1592) than in Group 2 (0.0%, 0/1553) (P = .044). The interval from the first hernia repair to the hydrocelectomy in 6 patients was 20.8 months (range, 8–36 months), and CHs in 6 patients developed 8–36 months after the initial hernia repair. The recurrence rate was higher in Group 1 (0.4%, 7/1592) than in Group 2 (0.0%, 0/1553) (P = .025). Table 2 shows the clinical characteristics of the patients who developed CH. The average age of the patients with CH was 25.0 months (range, 12–61 months), and symptoms were pain in 2 patients, discomfort in 3 patients, and increasing size in 1 patient. The symptoms were identified in patients and their parents when CH occurred. The clinical risk factor analysis and logistic regression test results are shown in Table 3. These test results indicated that age, laterality, and incarcerations were not associated with CH occurrence. As a result, leaving the hernial sac was the only significant risk factor for CH occurrence (odds ratio = 1.004, 95% confidence interval = 1.001–1.007; P = .016). In addition, we measured the accuracy of the regression prediction through a receiver operating characteristic curve consisting of an x-axis indicating 1 − specificity and the y-axis indicating sensitivity (Fig. 4). As a result of the model prediction, evaluation of the model and its accuracy rate (area under the curve = 0.747) showed that the derived equation appropriately represented the model. The following equation was derived in the regression test: Hydrocele = 0.003752 × Leaving the hernial sac, indicating that leaving the hernial sac has an influence of 0.003752 probability of hydrocele occurrence.

Logistic regression receiver operating characteristic curve. The x-axis represents 1 − specificity, and the y-axis represents the sensitivity.
Comparison of the Clinical Factors Between the Two Study Groups
Data are presented as mean (range), number (%), or number.
Most of the P-values represent comparisons of categorical variables, which were tested using the χ 2 test.
Continuous variables were tested using the Wilcoxon rank-sum test.
F/U, follow-up.
Clinical Characteristics of the Cord Hydroceles That Occurred in 6 Patients
Data are presented as mean (range).
Logistic Regression Analysis of the Risk Factors for Reoperation to Treat Hydrocele
Data are presented as number (%). Data were tested using logistic regression analysis.
CI, confidence interval; OR, odds ratio.
Discussion
This large-scale single-center study revealed that pediatric patients who underwent hernial sac resection at the time of laparoscopic inguinal hernia repair had a significantly lower incidence of subsequent CH than those who did not undergo sac resection. Hernia recurrence and CH occurrence are major causes of reoperation after LPIHR. A seroma, which is postoperative fluid collection at the surgical site, has no membrane surrounding the fluid and generally resolves with conservative treatments such as aspiration. However, a CH with a membrane surrounding the fluid is treated by hydrocelectomy. Although LPIHR includes both LTAC and LPEC, most comparative studies of reoperation rates have focused on laparoscopy versus open surgery; therefore, only minimal technical details have been given. Many studies have not distinguished the cause of reoperation as actual hernia recurrence versus CH occurrence. To the best of our knowledge, no studies have compared the outcome of LPIHR with or without hernial sac removal regarding CH occurrence.
Hernial sac disconnection and nonabsorbable suture material are reported to reduce the recurrence rate after primary pediatric inguinal hernia repair. 13 The recurrence rate was low in previously reported sac disconnection or removal surgery. 14 In the present study, the recurrence rate was higher in Group 1 than in Group 2, similar to results in other reports.
Most studies have evaluated recurrence after LTAC; few have addressed reoperation secondary to hydrocele occurrence. A meta-analysis of studies involving LPEC revealed a hydrocele occurrence rate of 0.23%. 5 In our group without hernial sac removal, CHs occurred in 6 patients: 5 patients within 2 years and 1 patient within 3 years after the initial operation. However, no CHs occurred in the hernial sac removal group. In our experience, removing the hernial sac is not difficult, and the iliopubic tract is clearly identified during LTAC.
Closing the deep inguinal ring during LTAC can be easily performed simply by leaving the hernial sac. A more advanced technique is to perform disconnection or transection and then remove the hernial sac. However, the standard pediatric inguinal hernia repair method with which most surgeons are familiar is to remove the distal hernial sac after the transection. Generally, surgeons remove the hernial sac during open hernia repair surgery; therefore, we believe that removing the hernial sac in LTAC is equal to open repair. Although some learning time may be required before achieving competency, the learning period may not be long. In this study, the gap in operation time between the two groups was ∼2 minutes. Postoperative early complications were not different between the two groups, and seromas occurred at similar rates in both groups, suggesting that the possibility of over-operation is low.
This study has limitations. First, this study was a historical control design, although a relatively large study population. Second, CH developed in 1/6 patients 36 months after the initial surgery; therefore, the follow-up period of 2.5 months in some of the patients in Group 2 might have been too short for the purposes of this study. Third, although there was no change in surgical staff and facilities during the study, improvement in surgical skills over time may have affected the outcome. Finally, this was a single-center study, and results may not be generalizable to other institutions and populations; therefore, future multicenter studies are needed.
In conclusion, our findings indicated that hernial sac removal resulted in a small but significant decrease in the risk of CH after LTAC in pediatric patients.
Footnotes
Acknowledgments
We thank Sa Rang Kim, Beom Seok Oh, and Young Hyun Lee from the research center of Damsoyu Hospital for assisting with the statistical analysis and organizing the data in this article. We thank Jane Charbonneau, DVM, from Edanz Group for editing a draft of this article.
Ethical Approval
This study was approved by the institutional review board of Damsoyu Hospital: DSY-2019-002.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.