
Abstract
Introduction:
Laparoscopic cholecystectomy (LC) is the gold standard performed by the majority of surgeons worldwide, and the use of single-port cholecystectomy remains a matter of debate. Single-port magnetic-assisted cholecystectomy (SPMAC) was described as an alternative because of its ability for proper triangulation and the advantage of reducing port surgery. The objective of this study is to describe the initial experience of SPMAC and evaluate the surgical learning curve.
Materials and Methods:
A prospective cohort was conducted between February 2017 and August 2018; 60 patients completed the inclusion criteria. Variables analyzed were gender, age, body mass index, American Society of Anesthesiologist (ASA) classification, operative time, hospital stay, intraoperative bleeding, and conversion rate. Postoperative pain was measured with a visual analogue scale (VAS). Aesthetic perception was measured by the cosmetic visual analogue scale (CVAS). The postoperative complications were graded according to Clavien–Dindo classification, and the cumulative sum (CUSUM) model was used for evaluating the learning curve.
Results:
The mean operatory time was 56.1 minutes. With regard to the postoperative pain variable, the VAS value was 2 out of 10 in 78.33% of patients. With regard to aesthetic satisfaction, CVAS was reported to be 10 out of 10 in 96.67% of patients. Conversion rate was 0%. The learning curve of operative time was reached at the 22nd patient, according to the CUSUM chart.
Conclusions:
SPMAC is feasible and effective; in our consideration, an acceptable learning curve considering benign gallbladder pathology is one of the most prevalent in general surgery. Further comparative studies with conventional LC and SPMAC need to be performed to conduct a proper comparison.
Introduction
Carl Langebuch undertook in Berlin the first cholecystectomy in July 1882 through a right subcostal incision; after a century, Eric Muhe performed the first laparoscopic approach, followed by the rapid adoption of the technique. 1 Nowadays, laparoscopic cholecystectomy (LC) is the gold standard treatment of symptomatic gallstone diseases, and it is well implemented by the majority of the surgeons worldwide. Usually, three or four ports are used as a standard technique. 2
A constant effort that allows access to the abdominal cavity, thereby reducing surgical trauma has led to the creation of techniques such as single-port surgery, mini laparoscopy, and natural orifice transluminal endoscopic surgery (NOTES).
Single-port laparoscopic cholecystectomy (SPLC) is a technique in which laparoscopic instruments are introduced by a single port for gallbladder removal.
This technique has the advantage of reducing the need for additional ports with less trauma to the abdominal wall; reducing bleeding by working through a single incision has technical concerns, because it requires the learning curve and can be challenging due to the low ability for instrument triangulation, leading to an increase in the operative time.
SPLC requires specific technology, the main reason for the biomedical industry to develop new devices, especially ports with multiple working channels.
Regarding the concerns, a single port requires a larger umbilical incision for port placement with the risk of port-hernia incidence; some authors have reported this to be around 13%. 3
Studies for SPLC report that this technique reduces the trauma of the surgical access with improvement in postoperative pain and cosmetic results, 4 but because of the incisional hernia risk (listed earlier) have led to a low spread in the surgical community worldwide.
Magnetic surgery is referred to as a surgical procedure in which a magnet is used to assist the operation, usually to expose surgical anatomy for dissection. Regarding gallbladder surgery, neodymium magnets allow grasping the fundus without the need for additional port placement. This results in a better cosmetic outcome and lower postoperative pain.
We started utilizing magnetic instruments in LC since 2017 with excellent results. The objective of this prospective cohort is to describe our experience for the first 60 cholecystectomies by a single surgical group and to evaluate the learning curve.
Materials and Methods
This article is reported according to the STROBE criteria for observational studies. 5
After ethical general surgery department committee approval, a prospective study between February 2017 and August 2018 was undertaken. Sixty patients were included in Fleming Clinic (Lima, Peru) for single-port magnetic-assisted cholecystectomy (SPMAC).
Inclusion criteria
Patients with calculous chronic cholecystitis and a body mass index (BMI) less than 35 kg/m2 were included. The diagnosis of cholelithiasis was obtained by an abdominal ultrasound; indications for cholecystectomy were patients who presented two or more biliary colics.
Exclusion criteria
Pediatric patients, pregnant women, BMI more than 35 kg/m2, and a previous episode of acute cholecystitis, malignancy, and prior abdominal surgery.
Collected data
Variables include clinical variables: gender, age, BMI, American Society of Anesthesiologist physical status classification system (ASA SCORE), and comorbidities.
Operative variables
Operative time, intraoperative bleeding, need for an additional port, and conversion rate.
Outcome data
Length of hospital stay and postoperative pain were measured by the visual analogue scale (VAS); complications and the cosmetic result were measured by the cosmetic visual scale (CVS), an appearance scale that measures cosmetic outcomes of healed scars (mostly used in the plastic surgery field). All patients were informed about the procedure, and information consent was signed.
The patients were followed at an outpatient visit on postoperative days 7 and 30.
Technical aspects and operative technique
The patient was placed in a supine position and was submitted to general anesthesia. Abdominal cavity access was achieved by Hasson technique, a 12-mm working port was placed at the umbilicus, and the pneumoperitoneum was maintained at 12 mm Hg during the entire procedure. A 5-mm, 50-cm-long trans-facial rigid grasper was introduced near the optic working port (Fig. 1), and this grasper was used for Hartman's pouch traction.
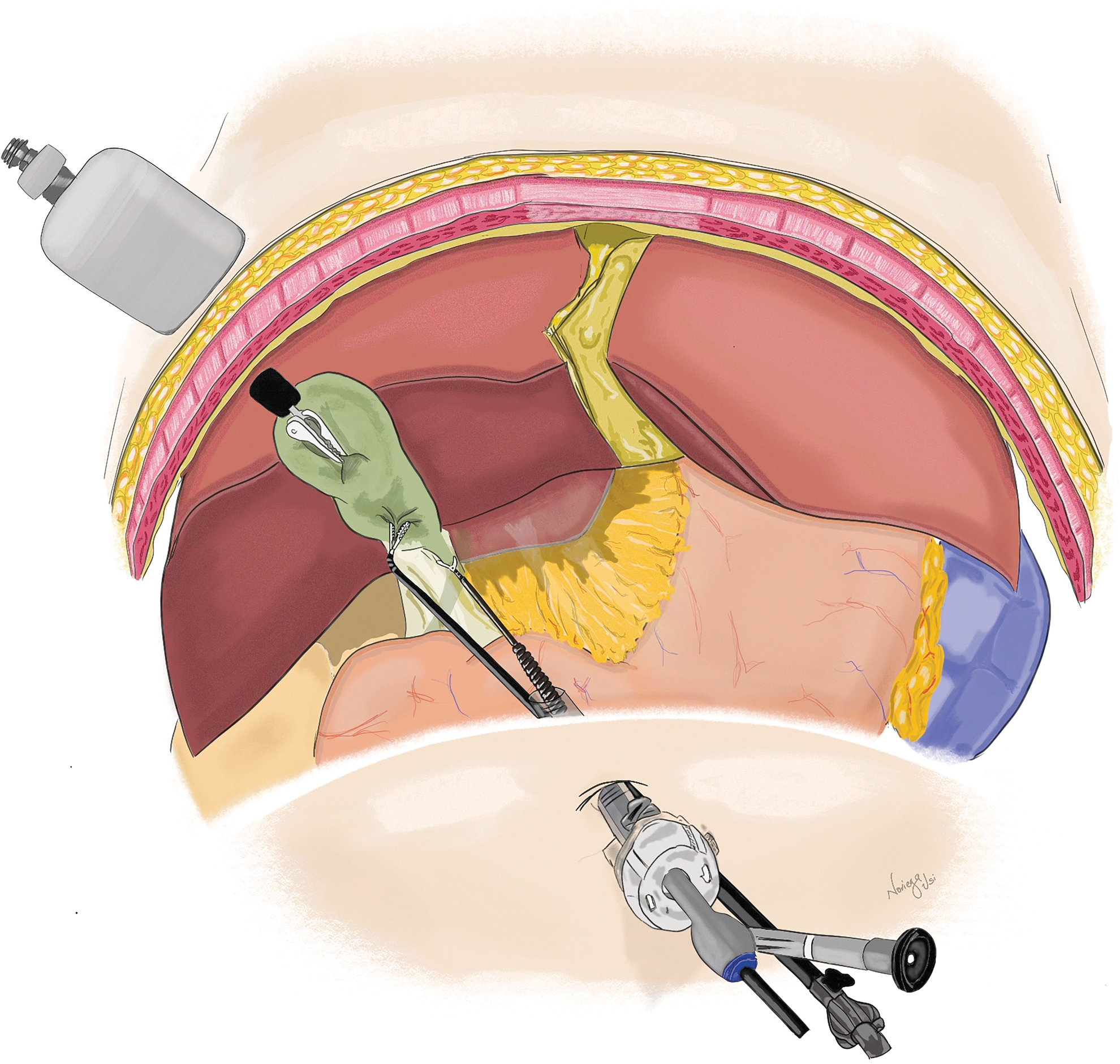
Shows optic port of 12 mm in the umbilicus with a working channel, below a 50-cm 5-mm percutaneous rigid grasper. The neodymium magnet is placed in the fundus and the handhold right abdominal wall for anatomical exposure (Figure by Victor Manuel Noriega Usi).
The magnetic device (IMANLAP, Buenos Aires, Argentina) is composed by a two-part system: the magnetic grasper that is introduced to the abdominal cavity through the 12-mm working port, and the handhold that is placed on the surface of the abdominal wall, at the right hypochondrium to modify the position of the magnetic grasper and anatomical exposure (Fig. 2).

Intraoperative view of single-port magnetic-assisted cholecystectomy achieving a critical view of safety.
The Hartmann's pouch was grasped, the hook was introduced through the working channel of the scope, and Calot's triangle was dissected in a regular fashion to achieve a critical view of safety (Fig. 3). The cystic duct and artery were clipped with a 5-mm Grena ML clip (Nottingham, United Kingdom), and the cholecystectomy was completed with a hook with monopolar energy.
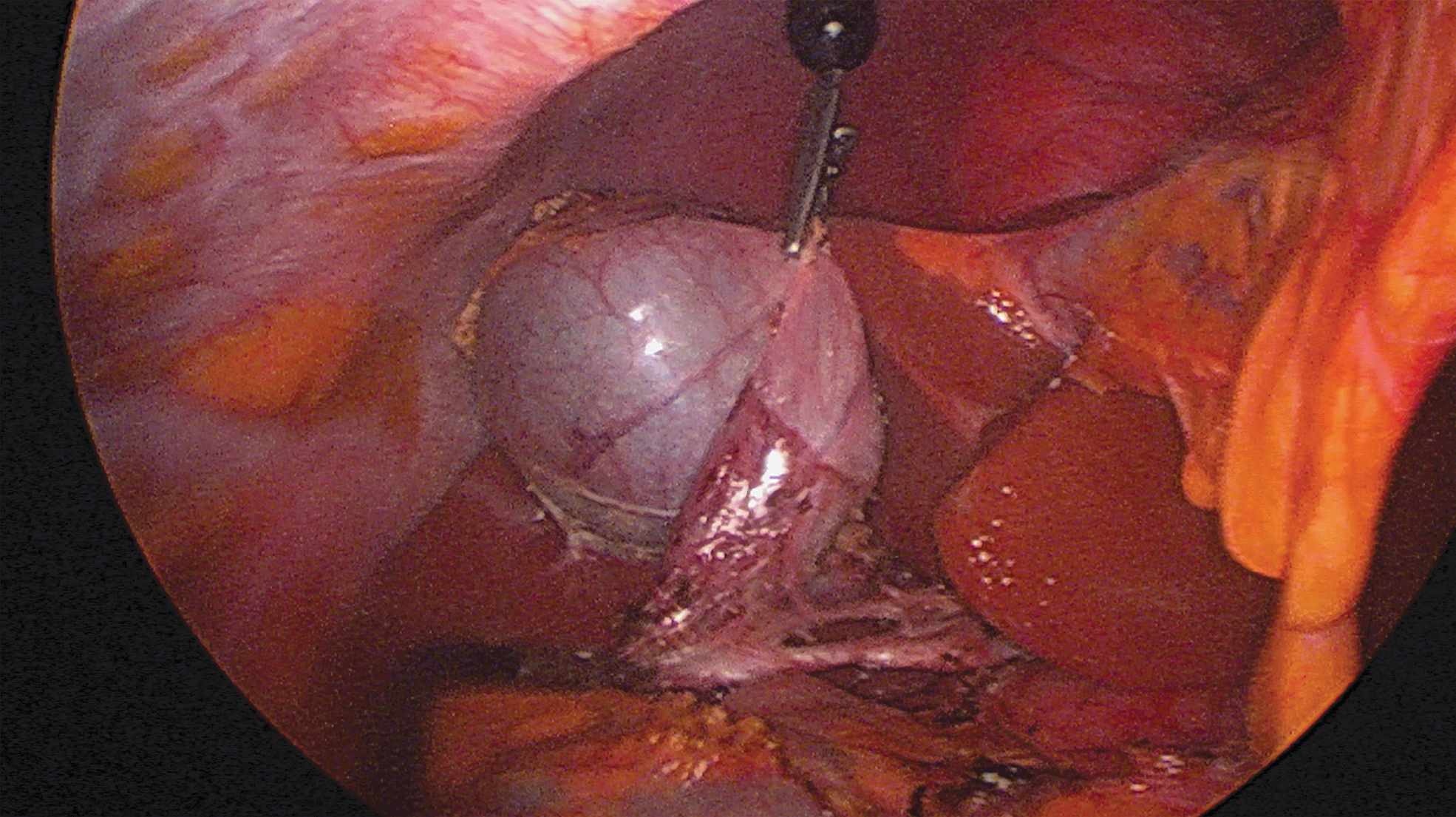
Laparoscopic view of Calot's triangle dissection.
Three different ways were used to extract the magnetic grasper:
The magnetic grasper was left grasping the fundus; then, both were introduced into the bag for extraction. The magnetic grasper was released from the fundus; extraction of the gallbladder and the magnetic grasper was done separately within a bag. The magnetic grasper was released, and removal was achieved through magnetism with laparoscopic forceps.
The latter description has been mostly used, because it is much easier and less time expensive.
The umbilicus was closed with polyglactin 910 with cross-stitch, and the skin was closed with 3-0 non-absorbable monofilament interrupted stitch.
The postoperative regimen included liquid diet after 12 hours with progression as tolerated; analgesia was maintained with a single intravenous nonsteroidal anti-inflammatory drug (NSAID; Ketoprofen). All patients were discharged at postoperative day 1.
Statistical analysis
Descriptive statistics were performed by using Software for Statistics and Data Science (v14.0; STATA, Lakeway, TX); p < 0.005 was considered significant. Variables with parametrical distribution were reported as mean and standard deviation (SD). The learning curve based on surgical time was calculated by piecewise regression analysis to obtain the CUSUM (cumulative sum) chart.
The CUSUM is a sequential analysis method that detects changes in an individual surgeon's performance; it is represented by a graphic that provides a rising line during the learning period, and a plateau as the performance stabilizes and the learning curve has been accomplished.
Results
There were 60 patients included; the mean age of the patients was 35.71 (SD: 4.48), mean weight was 61.6 (SD: 8.03), mean height was 1.55 m (SD: 0.038), and mean BMI was 25.34 kg/m2 (SD: 3.1). The proportion of the female population was 96.67%, and all patients presented an ASA I classification.
The mean operative time was 56.1 minutes (SD: 21.79). The operative bleeding was reported with gauze visual analogue; this scale measures the amount of blood in gauze. The mean operative bleeding was 6 mL (SD: 0), and this represents a 50% of saturation in a 10 × 10 cm gauze.
An additional port placement was required in 2 patients (3.33%). Conversion to conventional laparoscopic surgery was 0%.
Mean postoperative pain was 1.86 (SD: 0.44). Complications were presented in 3.33% of all Grade I Clavien–Dindo 6 at 30 days, both patients presented an umbilical seroma that was resolved after drainage, and no antibiotics were needed.
The mean aesthetic result was 9.93 (SD: 0.362) (Fig. 4). Two patients required an accessory port in the right upper quadrant, both patients had a BMI of 35 kg/m2, and the indication for port placement was an inadequate critical view of safety (Table 1).

Aesthetic perception of the abdominal wall after single-port magnetic-assisted cholecystectomy. Postoperative day 1.
Demographic Data of Patients Undergoing Single-Port Magnetic-Assisted Cholecystectomy
ASA SCORE, American Society of Anesthesiologist physical status classification system; BMI, body mass index; CVAS, cosmetic visual analogue scale; SD, standard deviation; VAS, visual analogue scale.
The fascial aggression in the umbilical region compared with single-port cholecystectomy is lower due to the use of a 12-mm trocar and a trans-fascial rigid grasper of 5 mm. After 12 months, the hernia incidence remained as 0%.
The CUSUM was initially designed for quality control, and it can be used in the surgical field to evaluate the behavior of a surgeon's performance in time. The objective is to determine the number of procedures that the surgeon requires to achieve a specific competence; this is reflected as a negative trend in the curve.
The CUSUM chart is made after determining the value of the mean operatory time (in our study was 50 minutes) and determining the lower and upper limit of the operatory time; these values correspond to H0 and H1 (−20 and +20, respectively). Operative time must be between these parameters; if the sum crosses the lower limit, (H0) reflects statistical significance and success. In our CUSUM chart, this was reached at the 22nd patient, proving that the learning curve has been reached (p < 0.005) (Fig. 5).
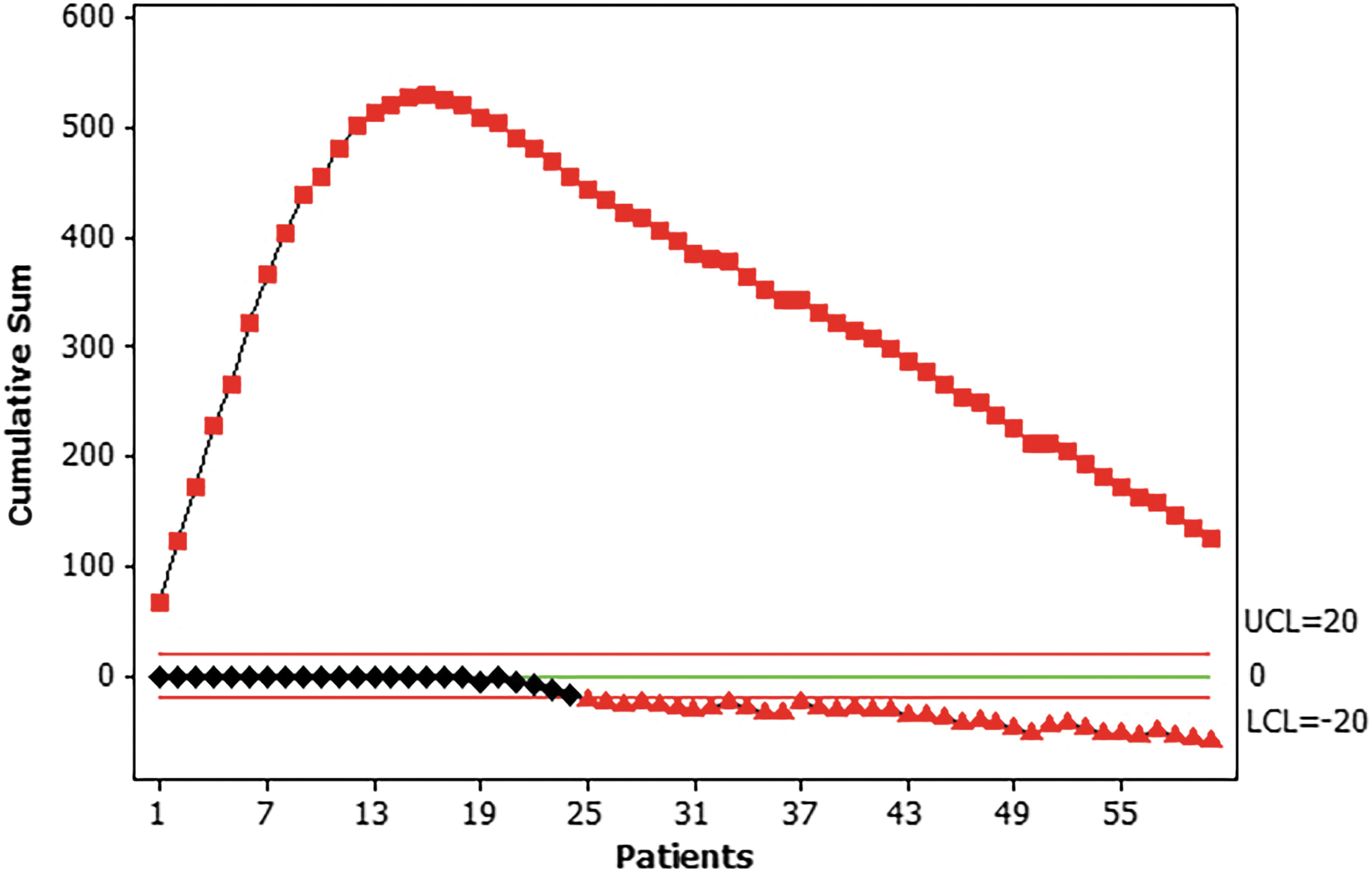
Learning curve cumulative sum chart, achievement in patient no. 22.
Discussion
Since minimally invasive surgery for cholecystectomy has emerged, it took 6 years to be called the “gold standard” due to the shorter hospital stay, with quicker recovery time compared with regular open surgery, fewer incisions that lead to a better aesthetic result and less discomfort. 7
Surgical tools have been created to allow the surgeon technical facilities for fewer invasiveness procedures and to reduce port surgery.
In 1997, SPLC emerged: Compared with standard LC, it has better cosmetic results, less postoperative pain, and faster recovery, but it is recognized that with SPLC basic principles of ergonomic cannot be achieved such as triangulation, which is perhaps the main reason for not complete technique adoption worldwide.8–10
After more than a decade, magnetic assistance was added to single-port cholecystectomy, as a surgical technique that uses magnetic properties to grasp the gallbladder fundus to expose Calot's triangle. The SPMAC differs from single-port cholecystectomy, because in all cases triangulation can be achieved.11–13
The first case of SPMAC was published in 2007 in Argentina by Domínguez et al., 10 with a subsequent report of a 40 patient series with a mean operative time of 93 minutes (95–130) and a 0% conversion rate; only 1 patient developed surgical site infection and was managed with antibiotics. 11 Studies in a pediatric population referred to SPMAC as a safety procedure. 13
Outcomes have evaluated this technique as feasible, with low complication rate and postoperative pain with excellent aesthetic results.
A meta-analysis of a single-port cholecystectomy reports biliary lesion incidence of 0.72% compared with 0.4–0.5% in standard LC. The biliary lesions are mostly associated with a reduced critical view of safety. 14 Currently, there are no biliary lesions reported for SPMAC.
In the setting of postoperative pain, a randomized controlled trial (RCT) that compares single-incision LC versus conventional LC reported lower extra-umbilical pain after 24 hours, more significant in a resting position in favor of a single port. 15 All the patients of our series were managed by one intravenous NSAID during the perioperative pain, and the mean postoperative pain was 1.85 (SD: 0.44) The 2 patients who referred 3 out of 10 VAS were those who required additional port placement. No patient presented considerable pain, and none required additional analgesia management.
Several meta-analyses report better aesthetic results when compared with conventional LC.16–20) The umbilicus is a natural embryological scar, and an incision through this area has good cosmetic results. Our mean of cosmetic visual analogue scale was 9.93 (SD: 0.36).
In 2016, The Levita™ Magnetic Surgical System (Levita Magnetics Corporation, San Mateo, CA) obtained the FDA approval for use in LC. 21
In 2017, the first American series of SPMAC using Magnetic Surgical System (Levita Magnetics Corporation) with 10 patients was published; the mean BMI was 27.6 kg/m2; the average operative time was 64.4 minutes; and 70% of patients were discharged home on the day of the surgical procedure and 30% on postoperative day 1.
Surgeons reported the use of the magnetic grasper as easygoing. This prospective series was performed by using three ports. 22
In 2018, Rivas et al. reported 50 cases using the Levita Magnetic Surgical System. The average BMI was 27 kg/m2 (20.4–34.1); the mean operative time was 63 minutes (SD: 19). The abdominal wall length was measured by ultrasound; the mean length was 2.6 cm. The surgeon's rate of surgical site exposure was excellent in 90% and sufficient in 10%. 21
In our series, 2 patients needed additional port placement, both of whom had a BMI of 35 kg/m2. It has been reported that with a more anteroposterior length of the abdominal wall, magnetic properties are reduced and with 6.95 cm the attraction forces are 0 grams/force. 23
Technical aspects and a learning curve have been reported after 10 cases for single-port cholecystectomy, but none has been reported for magnetic-assisted cholecystectomy. 24
As we currently know, the accurate determination of an LC is difficult to establish. The first step to create an LC is the selection of an appropriate outcome that indirectly reflects the ability of a surgeon to perform that particular task, on a temporal basis; this outcome will represent the clinical process and the task efficiency.
This study evaluates multiple indicators of task performance in the clinical process and also task efficacy, including operating time, blood loss, need for additional port placement, conversion rate, as well as intraoperative and postoperative complications.
There was no intraoperative complication and minimal intraoperative bleeding without any biliary lesion. The decrease in the operative time after patient 22 was attributed to technical understanding and systematization for magnetic grasper extraction. To our knowledge, this is the first prospective cohort that evaluates the learning curve in SPMAC.
The CUSUM methodology could be used in the training program of SPMAC.
Conclusions
Evolution demands continuous effort; surgical trauma must be reduced with proper cosmetic outcomes and complete safety of the surgical procedure without adding morbidity. Our series reflects that SPMAC is a safe and reproducible technique with a fast learning curve for a postgraduate surgeon.
This surgical technique differs from the traditional single-port surgery; utilizing neodymium magnets and working optic ports, there is no laparoscopic instrument collision. These properties allow obtaining the functional outcomes of a single port, including lower postoperative pain, better aesthetic results with the advantages of multiport surgery in triangulation, and ergonomic effects.
Results presented in this prospective study evaluated the safety and short-term outcomes after single-port magnetic-assisted cholecystectomy. Nowadays, SPMAC must be considered a technical armamentarium for the minimally invasive surgeon.
Footnotes
Acknowledgment
Juan Pablo Aparco: statistical analysis.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.