
Abstract
Background:
Pancreaticoduodenectomy (PD) involves complicated surgical procedures and is associated with high postoperative mortality. PD can be performed using laparoscopy; however, there is a lack of evidence on laparoscopic PD (LPD) outcomes in elderly patients. Therefore, this study aimed to compare LPD outcomes in elderly patients with those in patients aged <65 years and assess elderly outcomes according to the LPD surgical learning curve.
Materials and Methods:
In this retrospective study, medical records of 75 elderly patients (Group A) and 225 patients aged <65 years (Group B) were reviewed. Preoperative and postoperative data, as well as oncologic outcomes, were collected. To assess the effect of the surgical learning curve on outcomes of elderly patients, patients were equally divided into four phases, based on the number of surgeries performed at the study site.
Results:
The mean preoperative physical status score was significantly higher in Group A than in Group B (z = 5.222, P < .001), indicating higher disease severity. There were no significant differences in operative time, intraoperative blood loss, vascular reconstruction rate, or intensive care unit (ICU) stay between the groups. The blood transfusion rate (χ2 = 4.301, P = .038) and length of postoperative hospital stay (z = 2.386, P = .017) were significantly higher in Group A than in Group B. The surgical resection margins and the number of lymph nodes harvested did not differ between the two groups; however, a significant difference was observed in pathological results. In assessing the surgical learning curve, the pairwise comparison of means showed that the operation times in phases 3 and 4 were shorter than that in phase 1 (P < .05) and differences in nasogastric tube removal time between the four groups were statistically significant (H = 15.390, P = .002).
Conclusions:
Advanced age alone should not be a contraindication for LPD, since outcomes for elderly patients who have undergone LPD are similar to those for younger patients.
Introduction
Pancreaticoduodenectomy (PD) is the only radical surgery for tumors of the ampulla and its surrounding area and has been widely used in clinical settings. Many studies have shown that in surgical groups with rich experience in PD, elderly patients without obvious surgical contraindications have similar safety and efficacy rates compared with nonelderly patients. 1 In addition, studies have shown that compared with laparotomy, laparoscopic PD (LPD) has the same safety and effectiveness with certain advantages, such as reduced recovery time and less scarring. 2 LPD was one of the first surgeries to use the laparoscopic technique, first reported by Gagner and Pomp 3 in 1994. However, due to limitations in surgical training and instruments, LPD was not used widely after its introduction. Currently, with the rapid development of technology and training, laparoscopy has transformed many surgeries, and almost all abdominal surgeries can now be performed routinely using this technique.4,5
However, LPD still involves complicated surgical procedures and is associated with high postoperative mortality. Therefore, surgeons make conservative treatment decisions with elderly patients who need PD. In addition, because of the complexity of LPD, only a few experienced surgeons perform it routinely. Meanwhile, few studies have assessed the safety and effectiveness of LPD in elderly patients. This study aimed to evaluate the safety, feasibility, and oncologic outcomes of LPD in elderly patients and compare them to those in younger patients. A secondary aim of the study was to assess outcomes of elderly patients according to the LPD surgical learning curve.
Materials and Methods
This retrospective study included 300 consecutive patients who underwent LPD with complete data between April 2015 and March 2019. Of these patients, 75 were elderly patients (Group A, age ≥65 years), and 225 were nonelderly patients (Group B, age <65 years). Written informed consent was obtained from all patients before the operation. All procedures were performed by an experienced hepatopancreatic and biliary surgeon (Y.L.) at a single institution. The study was approved by the Ethics Committee of the First Hospital of Jilin University.
Surgical procedures
The patients adopted a supine position with legs separated. A 12 mm trocar was selected to establish pneumoperitoneum 3 cm below the umbilicus, which was used as an observation port for surgery. The pressure of carbon dioxide pneumoperitoneum was maintained at 12–14 mmHg. The surgeon stood on the right side of the patient, the assistant stood on the left side, and the laparoscope holder stood between the legs of the patient. The operation was performed using the posterior colonic approach. Reconstruction was performed using pancreaticojejunal, bilioenteric, and mechanical gastrojejunal anastomoses.
Postoperative management
All patients were transferred to the ICU for monitoring and treatment after surgery. Patients were transferred to general wards within 1–2 days when all indices stabilized. All patients received prophylactic empirical antibiotics. According to the protocol for fast-track surgery, all patients had their nasogastric tubes removed on the first day after surgery, and liquid food was administered once anal exhaust was restored. The drainage volume was closely observed after surgery, and if the drainage volume was <50 mL/d and the amylase level in the ascitic fluid was <3000 IU/L, the nasogastric tube was removed on the third day after surgery.
Variable definitions
The American Society of Anesthesiologist (ASA) physical status classification score was assessed preoperatively. Operative time was calculated as the time from trocar placement to entire skin closure. The estimated blood loss was recorded carefully through a vacuum system. Length of stay was defined as days from admission to discharge. According to the 2017 International Study Group of Pancreatic Surgery (ISGPS) criteria, 6 the pancreatic fistula was classified as a biochemical leak, grade B, or C, and only grade B and C were considered clinically significant. Similarly, we defined delayed gastric emptying (DGE) 7 and postpancreatectomy hemorrhage 8 according to the ISGPS definitions. Biliary leakage was defined as an elevated bilirubin level in the abdominal drainage fluid. Gastrointestinal anastomotic hemorrhage was identified based on gastric tube drainage accompanied by hemoglobin blood drop. Ascites was defined based on postoperative abdominal imaging examinations, such as ultrasound or CT scan. Studies show that the occurrence of postoperative ascites was related to surgical trauma, local inflammatory response, and the production of endotoxin by microorganisms. 9
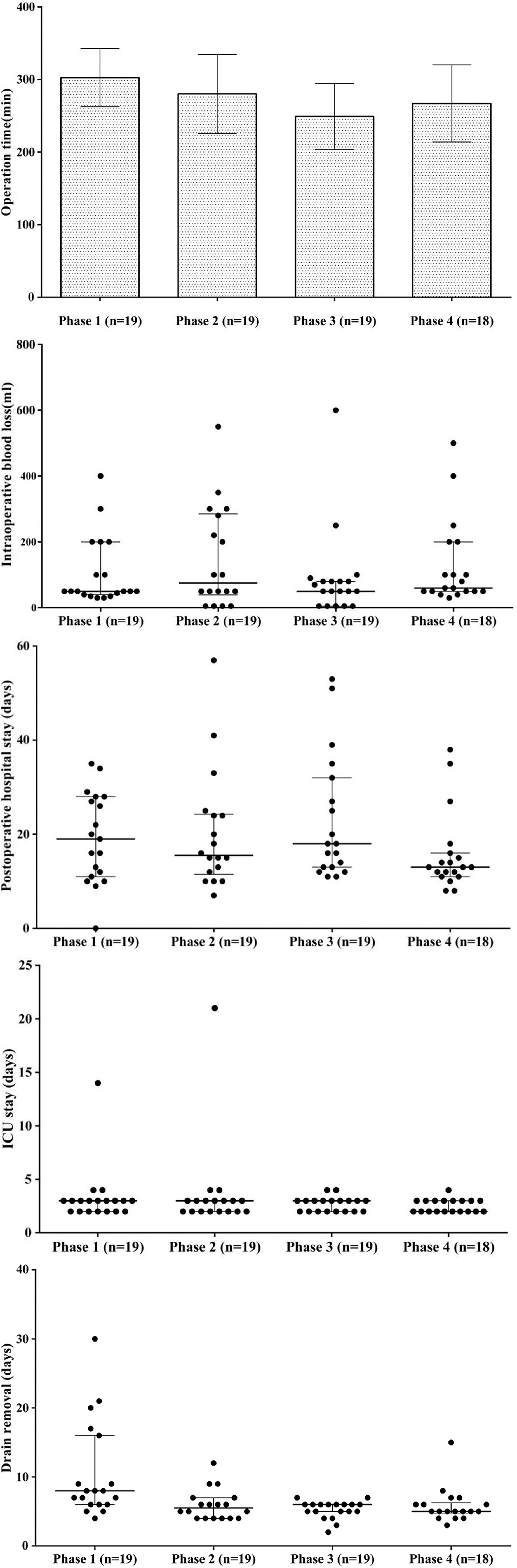
To assess elderly outcomes according to the surgical learning curve, the elderly patients were equally divided resulting in four consecutive phases within the study period. Phase 1 included the first 19 patients from April 2015 to September 2017; phase 2 included the next 19 patients from October 2017 to August 2018; phase 3 included 19 patients from September 2018 to January 2019, and phase 4 included the remaining 18 patients from February 2019 to March 2019.
Statistical methods
Data were collated using Excel 2007 (Microsoft Corp., Redmond, WA) and analyzed statistically using SPSS 22.0 software (SPSS, Chicago, IL). Measurement data are expressed as mean (percentages). For pairwise comparison of measurement data, t-tests were used for data with normal distribution, and Wilcoxon signed rank-sum tests were used for data with nonnormal distribution. Enumeration data were expressed as frequency or rate, and comparisons were performed using chi-squared tests. The Fisher exact probability method was used when the theoretical frequency was <1. A P-value <.05 indicated statistical significance for all tests.
Results
Preoperative general condition
Preoperative general conditions of patients in Group A and Group B are shown in Table 1. The proportion of male patients in Group A was 60%, and that in Group B was 53%, indicating no statistically significant difference in gender composition between the two groups (χ 2 = 1.010, P = .315). There was no statistically significant difference in body mass index between the two groups (t = 0.964, P = .336). The comparison of ASA scores between the two groups showed that Group A scores were higher than those in Group B, and the difference was statistically significant (z = 5.222, P < .001). Comparison of other preoperative general conditions of patients in the two groups showed no statistically significant differences (P > .05).
Comparison of the Patient General Preoperative Condition
Fisher exact probability method results.
ASA, American Society of Anesthesiologists; BMI, body mass index.
Assessment of the surgical learning curve using elderly outcomes
The operation time, intraoperative blood loss, postoperative hospitalization stay, ICU stay, and time of drain removal for each phase are shown in Figures 1A–E. Analyses showed that the operation times between the four phases were significantly different (F = 4.064, P = .010). Pairwise comparisons showed that the operation times in phases 3 and 4 were shorter than those in phase 1 (P < .05). Similarly, differences in drain removal times between the four groups were statistically significant (H = 15.390, P = .002). The binomial comparisons showed that the drain removal times in phases 2, 3, and 4 were shorter than those in phase 1, with statistically significant differences (P < .05). There were no statistically significant differences in other operation variables, postoperative hospital stays, or complications between the four phase (P > .05), as shown in Table 2.
Assessment of the Surgical Learning Curve Based on Perioperative Results in the Elderly
Results from Fisher exact probability method.
DGE, delayed gastric emptying; ICU, intensive care unit; ISGPF, International Study Group of Pancreatic Fistula.
Discussion
In this study, we aimed to compare pre-, intra-, and postoperative variables in elderly and nonelderly patients who underwent LPD to assess differences in outcomes. According to the preoperative ASA scores, the disease severity in the elderly patients was significantly higher than in nonelderly patients. Despite this, our results show that LPD outcomes in elderly patients were similar to those in nonelderly patients.
According to the World Health Organization, age >65 years is defined as old age. Studies have shown that >60% of patients who undergo general surgery are aged >65 years. 10 Moreover, age is one of the most important independent risk factors affecting the prognosis of all diseases. With the increase of age, age-related diseases such as pneumonia, coronary heart disease, hypertension, diabetes, cerebrovascular disease, and hyperproteinemia are more prevalent, which increases the risk of mortality after surgery.11,12 For example, one study showed that the risk of cardiovascular complications was three times higher and the risk of pulmonary complications was two times higher in patients aged ≥70 than in patients aged <70 years. 13 Meanwhile, the risk of pancreatic head and surrounding tumors in elderly patients is more than 50 times higher than that in younger patients,14,15 leading to a higher proportion of elderly patients requiring PD. In recent years, surgical technique and technology have advanced rapidly; however, one study showed a 40% prevalence in pancreaticoduodenal resection complications after abdominal surgery.16,17 Because of these risks, clinicians may choose more conservative palliative care or other treatments that may not be as effective as LPD.
Some studies show that the average operation time of LPD surgery is 301 minutes, 18 while the average operation times of the two groups of patients in this study were 274.85 minutes in the elderly and 271.52 minutes in the nonelderly patients. A shorter operation time is associated with a lower incidence of postoperative complications. The intraoperative blood loss was the same in the both groups, but the transfusion rate was statistically different. This is most likely due to the poor tolerance of elderly patients to ischemia. Therefore, regarding postoperative recovery, although the intraoperative blood loss is similar, the transfusion rate is expected to be higher in the elderly group.
Studies show that the incidence of postoperative complications associated with LPD can be as high as 30%. 18 Among the complications, studies show that pancreatic fistula is the most common complication, reaching as high as 35% 19 ; the second-most common complication is DGE, reported to be as high as 14%–61%. 20 In this study (Table 3), the incidence of the two most common complications was not significantly different between groups. Even though the incidence of complications tended to be higher in the elderly group, it was still lower than what has been reported in the literature. In terms of postoperative hospital stay, the elderly group stayed longer, indicating that although the outcomes were similar, the recovery rate of the elderly patients was slower than that of the nonelderly patients, which is to be expected. Based on our results, LPD is equally safe in elderly and nonelderly patients and age alone is not a contraindication for LPD, but elderly patients need more hospital time for recovery.
Comparison of Surgical and Postoperative Conditions
DGE, delayed gastric emptying; ICU, intensive care unit; ISGPF, International Study Group of Pancreatic Fistula.
According to postoperative pathological aspects (Table 4), the tumor size, lymph node number, and number of positive lymph nodes were not different between groups, but there were differences in pathological results. The elderly group had more pancreatic ductal adenocarcinoma and bile duct carcinoma, while the nonelderly group had higher rates of ampulla carcinoma and bile duct carcinoma, which shows that age may be associated with different tumor susceptibility.
Comparison of Postoperative Pathology Between Elderly and Nonelderly Patients
IPMN, intraductal papillary mucinous neoplasm.
Fisher exact probability method results.
There is a learning curve in the development of any technique. Studies have shown that after the initial 10 cases of LPD, operation time and blood loss significantly decrease, and the decreasing trend continues up to 50 cases. 21 Results from the present study show that the operation times between the four phases were statistically significant. Results showed that phases 3 and 4 had operation times shorter than those of phase 1. In addition, the nasogastric tube removal times of the four phases were statistically different. Timing of the nasogastric tube removal in phases 2, 3, and 4 was shorter than that in phase 1, showing a clear downward trend. Shorter operation time and earlier removal of nasogastric tube feeding are associated with faster recovery. Although the operation time, postoperative hospital stays, and complications were not statistically different between the four phases, there was a decreasing trend. The statistical results may be limited due to the small sample size, but it suggests that the risk of postoperative complications may be reduced with accumulated LPD experience.
This study had some limitations to consider. First, the number of cases was small, and all patients came from a single center within a short time. In addition, there was no long-term follow-up due to the recent introduction of LPD. Therefore, the results need to be confirmed further by a multicenter, large-scale, randomized clinical study.
Conclusion
LPD in elderly patients has similar outcomes compared with those in nonelderly patients. The learning curve for LPD shows a downward trend in indicators associated with postoperative complications. Therefore, LPD is an effective treatment in the elderly population.
Footnotes
Acknowledgment
The authors thank Editage for English language editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.