
Abstract
Background:
Some reports assert that there is a risk that laparoscopy might worsen the prognosis of incidental gallbladder carcinoma (IGBC) after laparoscopic cholecystectomy (LC) compared with open reoperation. The purpose of this study was to evaluate whether the surgical approach influences outcomes in patients with IGBC after LC.
Methods:
We retrospectively reviewed the medical records of 106 patients diagnosed with IGBC who had undergone LC for benign gallbladder disease such as cholecystolithiasis at our hospital between April 2010 and February 2018. We included patients with incidentally diagnosed GBC after routine pathology: 45 patients (16 men and 29 women; age: 45–76 years [mean: 62.6 years]) who underwent laparoscopic surgery and 61 patients (24 men and 37 women; age: 51–82 years [mean: 62.6 years]) who underwent open surgery. We evaluated outcomes in each group regarding tumor stage and operative time, time of reoperation after first operation, blood loss volume, number of lymph nodes in pathological specimens, hospital stay, and complication and survival rates.
Results:
Reoperation time after first operation, number of lymph nodes in pathological specimens, and operative time showed no statistical significance between laparoscopy and open reoperation. During follow-up, 3-year survival between laparoscopy (48.89%) and open reoperation (42.62%) showed no statistical significance, but laparoscopy had better 1-year survival (95.56% versus 86.89%, laparoscopy versus open, respectively; not significant [NS] <0.01) and 5-year survival (44.44% versus 29.51%, laparoscopy versus open, respectively; NS <0.05). However, comparing laparoscopy versus open surgery, respectively, blood -loss volume (100 ± 25.4 mL versus 200 ± 45.6 mL; NS <0.01), hospital stay (3.5 ± 1.9 days versus 5.6 ± 2.7 days, NS <0.01), and complication rates (6.7% versus 13.1%; NS <0.01) were lower, indicating better recovery and better patient experience.
Conclusions:
Laparoscopic radical reoperation for IGBC after LC is a feasible, effective, and safe procedure and is associated with less bleeding, low morbidity, and shorter hospital stay.
Introduction
Gallbladder carcinoma (GBC) is a fatal disease with poor outcomes. GBC is the most common cancer of biliary tract cancers and the fifth most common cancer in the gastrointestinal tract.1,2 Clinical symptoms and imaging findings for GBC are nonspecific and similar to chronic cholecystitis. By the time symptoms of GBC develop, the tumor would have invaded the major bile duct or liver parenchyma and possibly lymph nodes, and the disease has advanced. Although much progress has been made in treating many other gastrointestinal cancers, GBC prognosis and treatment have benefitted less at the same time.
Because of increased use of laparoscopy, a greater number of GBCs are diagnosed during or after cholecystectomy by pathological examination, and are defined as incidental GBC (IGBC). Most IGBCs are early stage, which is encouraging in that, if diagnosed early and tumor cells are found within the gallbladder mucosa, 5-year prognosis is ∼100% survival. 3 For cholecystitis and cholelithiasis, laparoscopic cholecystectomy (LC) has the advantages of shorter hospital stay, less pain, lower blood loss, shorter surgery time, and fewer complications versus open cholecystectomy. Several studies also suggest that laparoscopy does not adversely influence the prognosis of patients with IGBC versus open surgery after cholecystectomy.4–6
This study was established to evaluate whether laparoscopic surgery is safe and efficient compared with open surgery by analyzing intra- and postoperative factors and to evaluate whether laparoscopic surgery worsens the prognosis when IGBC is detected after LC.
Methods
We retrospectively reviewed the medical records of 106 patients diagnosed with IGBC after cholecystectomy for symptomatic cholelithiasis at our institution between April 2010 and February 2018. And all of 106 patients underwent LC before a secondary surgery. Of the 106 patients, 45 patients underwent laparoscopic surgery and 61 patients underwent open surgery. In both groups, a diagnosis of cholecystitis, cholelithiasis, or gallbladder adenomyosis was confirmed by imaging examination using ultrasonography or computed tomography (CT) before LC in all patients. We performed standard LC using a retrieval bag for gallbladder extraction in all patients. No included patients received adjunctive therapy (chemotherapy or radiotherapy).
All patients were followed for 3–6 months postoperatively with ultrasonography and enhanced CT when necessary, every 6 months. We defined disease recurrence as any tumor recurrence: distant metastasis, widespread or local peritoneal seeding, and port-site or scar recurrence. In the laparoscopic group, the median follow-up was 38 months (range: 3–84 months) versus 33 months (range: 6–72 months) in the open group. Statistical analysis were performed using statistical analysis procedures. And correlation between survival, operative time, bleeding, number of lymph nodes in pathological examinations, hospital stay, and complications (postoperative bleeding, incisional infection, bile leakage, and incisional hernia) were evaluated using the log-rank test. P-values <.05 were considered statistically significant. Statistical analyses were performed using SPSS (IBM, Armonk, NY).
Results
Laparoscopic patients included 16 men and 29 women with an average age of 62.6 years (range: 45–76 years), and open patients included 24 men and 37 women with an average age of 65.2 years (range: 51–82 years) (Table 1). No patients with GBC were diagnosed preoperatively. The indications for surgery were gallstones in 65 patients (28 laparoscopic versus 37 open), gallbladder polypus in 22 patients (10 laparoscopic versus 12 open), gallbladder adenomyosis in 9 patients (4 laparoscopic versus 5 open), and concurrent gallbladder polypus and gallstones in 10 patients (3 laparoscopic versus 7 open).
Patient Demographics for Patients of Incidental Gallbladder Carcinoma
LC, laparoscopic cholecystectomy.
Patients' tumor stage was based on the pathological tumor-node-metastasis staging system given in Table 1, 65 patients had pT1b adenocarcinoma (30 laparoscopic versus 35 open), 39 patients had pT2 adenocarcinoma (15 laparoscopic versus 24 open), and 2 patients had pT3 adenocarcinoma (both open patients). No significant differences in tumor stage were found in the two groups, and no patients had pT4 disease. Both groups underwent additional radical surgery 11.2 days (range, 7–16 days) (laparoscopic patients) and 11.6 days (range: 7–18 days) (open patients) after first operation. Additional procedure involved regional lymphadenectomy and excision of the liver bed.
No patients undergoing laparoscopy were converted to open surgery (Table 2). Operation time in the laparoscopic group was 115 ± 32.5 minutes versus 100 ± 20.4 minutes in the open group, and the difference was not statistically significant. Intraoperatively, the number of lymph nodes detected by the surgeon and confirmed pathologically was 19.8 ± 7.9 in the laparoscopic group and 17.3 ± 5.7 in the open group, with a nonsignificant difference. Figures 1 and 2 show the details of the laparoscopic lymph node dissection. Blood loss volume in the laparoscopic group was 100 ± 25.4 mL versus 200 ± 45.6 mL in the open group (P < .05). Hospital stay was 3.5 ± 1.9 days versus 5.6 ± 2.7 days, laparoscopic versus open, respectively (P < .01).
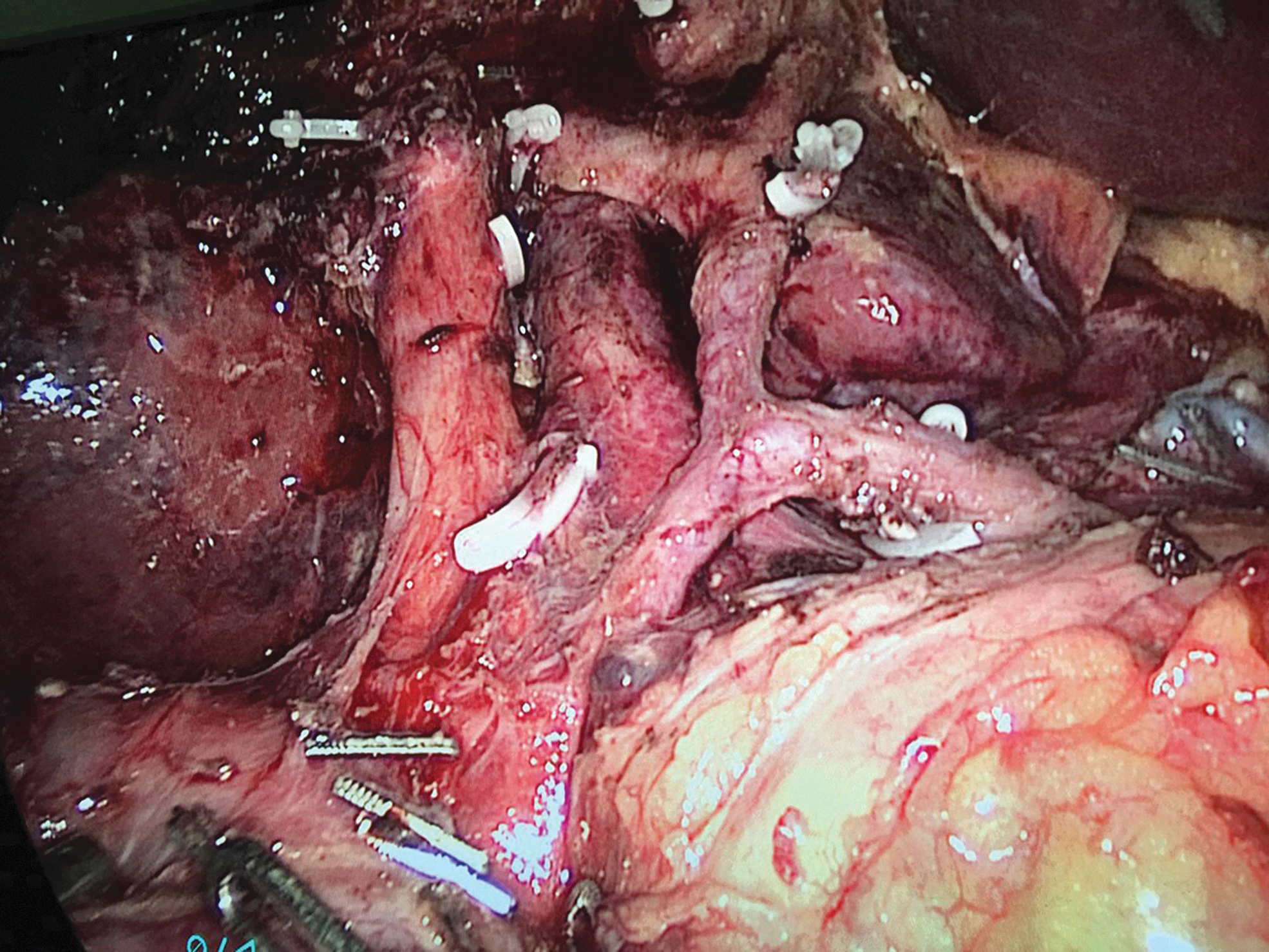
Vascular skeletonization in laparoscopic lymph node dissection.

Vascular anatomy. Red indicates an artery, blue indicates a vein, and yellow indicates a bile duct.
Perioperative Data
NS, not significant.
Complications after surgery for GBC include postoperative bleeding, incisional infection, bile leakage, and incisional hernia. No laparoscopic patients experienced postoperative bleeding versus 1 open patient. No incisional infection developed in laparoscopic patients versus 2 in open patients. One laparoscopic patient experienced bile leakage versus 2 open patients. No incisional hernias occurred in laparoscopic patients versus 1 in the open group. Four patients experienced other complications: 2 laparoscopic patients and 2 open patients, with a statistically significant difference (P < .05).
Median laparoscopic patient follow-up was 38 months (range: 3–84 months) versus 33 months for open patients (range: 6–72 months). GBC recurred 1 year postoperatively in 10 patients: 2 laparoscopic and 8 open (P < .01), and 3 years postoperatively in 58 patients: 23 laparoscopic versus 35 open (P > .05). The number of patients achieving 5-year survival in the laparoscopic versus open groups was 20 versus 18 patients, respectively, which was statistically significant (P < .05) (Table 2); no scar recurrences occurred postoperatively.
Discussion
GBC is a highly fatal and aggressive disease with a dismal prognosis. Also, early GBC has no specific symptoms. Once symptoms such as a palpable gallbladder mass, hard nodular liver, and malignant ascites secondary to carcinomatosis are detected by CT and magnetic resonance imaging, the disease is advanced.2,7,8 Currently, >90% of cholecystectomies are performed laparoscopically, and consequently, GBC is now often detected incidentally during or after LC.
IGBC is identified when GBC is found histopathologically after gallbladder removal for symptomatic benign gallbladder disease.9,10 GBC is suspected preoperatively in only 30% of patients11,12; the remaining 70% of patients with GBC are discovered incidentally by the pathologist. Because of the increased use of LC and difficulty diagnosing GBC preoperatively, IGBC discovered during and after LC has become more frequent, ranging from 0.2% to 2.9% of patients13–16 In this study, no patients were initially suspected of having GBC during LC, and all diagnoses were confirmed as IGBC after pathological examination.
Patients undergoing LC develop postoperative intraperitoneal adhesions, which complicates intraperitoneal anatomy and may increase difficulty during the secondary surgery in IGBC patients. Current surgical strategies for IGBC remain controversial.6,17 Both laparoscopic surgery and open surgery are widely used as the reoperation strategy after the first operation. The advantages of laparoscopic surgery are microinvasion, light pain, and quick rehabilitation; however, the advantages of open surgery are clear anatomical structure and wide operating space. To evaluate the difference of the two strategies, intraoperative blood loss volume, operative time, and the number of lymph nodes in pathological specimens all have been used to evaluate laparoscopic versus open approaches for IGBC. In this study, intraoperative blood loss volume in laparoscopic surgery was much lower than that in open surgery, which might be related to surgeons' experience with laparoscopy and coagulation. Also, compared with open surgical incisions, the smaller trocar holes reduce the amount of highly vascular skin and subcutaneous tissue to be incised.
Lymph node involvement is an important prognostic factor in patients with GBC, with significant differences in survival between nodal-negative disease and nodal-positive disease (5-year survival: 58%–77% versus 0%–45%, respectively).18,19 Many authors recommend lymph node dissection to improve survival of patients with GBC.19,20 With developments in laparoscopic lymphadenectomy, laparoscopic surgery for IGBC is becoming easier. Although laparoscopic lymphadenectomy requires more experience than for open lymphadenectomy because the laparoscopic approach requires complex vascular control and delicate dissection, in our study, the number of lymph nodes in pathological specimens in laparoscopic patients was slightly higher than for open patients; however, this difference was not statistically significant.
In general, laparoscopic surgery requires more time than open surgery, possibly because of lower surgeon experience with laparoscopy. In our analysis, we found no statistically significant difference for operative time for laparoscopic versus open surgery. As laparoscopic techniques and surgical skill develop, gaps between the two approaches will become insignificant.
In our study, no laparoscopic patients were converted to open surgery. However, the current major concern regarding laparoscopic surgery for patients with GBC is recurrence at scar or trocar holes and the spread of GBC cells when creating pneumoperitoneum.21–23 Implantation of GBC cells in the subcutis during tissue extraction may contribute to this concern. To prevent GBC cells from spreading, a retrieval bag is recommended in all patients undergoing laparoscopic surgery.24,25 Using a retrieval bag also prevents bacterial infection from bile leakage, which helps reduce the incidence of incisional infection. In many studies, retrieval bags are used only in surgeries in which the gallbladder is punctured. In our study, we used retrieval bags in every patient. Recent articles demonstrate that the incidence of abdominal wall implantation does not increase with laparoscopic surgery, and it is more likely a manifestation of the aggressive nature of GBC. 22 In our analysis, recurrence in the laparoscopic versus open groups was lower at 1 year. Although 10 patients in the current series had tumor recurrence within 1 year, and the difference was not significant at 3 years, the overall incidence of tumor recurrence was not high after surgery for patients with early stage GBC and might have resulted from the aggressive nature of carcinoma. Unlike some previous reports, in our study, repeat laparoscopic surgery compared with repeat open surgery did not increase peritoneal dissemination and port-site recurrence. This may have resulted from caution for facilitating tumor-free manipulation during surgery, our surgeons having experience and skill, and standardized use of retrieval bags.
In our study, overall 5-year survival after laparoscopic surgery was higher than that for open surgery, and, compared with open surgery, laparoscopic surgery improved the prognosis of IGBC patients rather than worsening it. And the results of this study support the hypothesis. Although the difference between two groups of recurrence after 3 years is not significant, recurrence after 1-year and 5-year survival of laparoscopic surgery is better in this study. Complications after laparoscopic surgery in our study were also much lower than that after open surgery; only 1 patient developed bile leakage, and 2 experienced other complications. Open postoperative complications included two bile leakage, one postoperative bleeding, two incisional infections, one incisional hernia, and two other complications. Using laparoscopy, surgeons may have a clearer view of the anatomy and complete surgery with less invasion.
Laparoscopic surgery for IGBC has a better prognosis, lesser bleeding during the procedure, fewer complications, shorter length of hospital stay and shorter recovery from disease compared with open surgery, because laparoscopic surgery has fewer complications and minimal invasion.
Conclusions
In our study, patients diagnosed with IGBC who underwent laparoscopic surgery had better survival and fewer complications than patients undergoing open surgery. This is likely because of the advanced laparoscopic technique and lesser invasion. Laparoscopic radical reoperation for IGBC after LC is a feasible, effective, and safe procedure and is associated with less bleeding, low morbidity, and a short hospital stay.
Our study has certain limitations. One of those is sample size is not so large, which is because morbidity of GBC is low and all the cases are collected in a single institution. Another important limitation is that follow-up time is not long enough. As for the limitations of follow-up time and small sample size, further study is needed to define the definite results.
Footnotes
Acknowledgment
We thank Jane Charbonneau, DVM, from Liwen Bianji, Edanz Group China, for editing the English text of a draft of this article.
Disclosure Statement
All the authors declare that this research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors, thus disclosing any conflict of interests regarding such work.
Funding Information
No funding was received.