
Abstract
Background:
Management of refractory esophageal strictures in children is challenging and mostly involves frequent and prolonged dilatations that are associated with significant physical and psychological complications. Biodegradable stents (BDS) have recently been used and it is particularly attractive in children as stent removal is avoided due to their dissolution.
Report of Cases:
We report our experience with BDS use in 3 children with severe refractory esophageal strictures. Two of the patients had strictures as a result of caustic ingestion and 1 after long-gap esophageal atresia repair. Median number of dilatations prestent is 5 per year. Custom-made uncovered BDS were inserted under general anesthesia. Median follow-up period was 23 months.
Results:
Minor postprocedure complications occurred in 1 patient. Stent insertion led to temporary improvement in swallowing in all cases. However, all of the patients developed recurrent symptoms as severe as before stenting and need for dilatations remained unchanged. They also experienced mucosal hyperplasia that contributed to their recurrent symptoms.
Conclusion:
All of the cases in our series did not have a favorable outcome with BDS use. BDS is yet to be proven as an effective management option for refractory esophageal strictures in children from our experience as well as most other published reports.
Introduction
Esophageal strictures in children occur commonly as a result of corrosive ingestion, anastomotic scarring after esophageal atresia repair and gastroesophageal reflux. 1 Most strictures can be successfully managed with dilatations. However, up to 30% of anastomotic strictures after esophageal atresia repair are refractory to conventional treatment.2,3 A refractory stricture is defined as one where age-appropriate feeding is not obtained after up to five dilatations each performed at 4-week intervals maximally. 4 They are usually managed with prolonged and frequent dilatations, which are, in turn, associated with significant physical and psychological complications. 3
Esophageal stents have been used in the past couple of decades to manage refractory strictures in children with the aim of achieving resolution of symptoms or reduction in the need for dilatations.5,6 Commonly used plastic and metallic stents have been associated with complications, including migration, chest pain, and respiratory compromise from tracheal compression. Esophageal injury, including perforation from these stents and insertion/removal process, has also been reported.6,7
More recently, biodegradable stents (BDS) have been developed. These stents are made of bioresorbable suture material, therefore avoiding the need for subsequent removal. This is particularly attractive for use in children. Data about the efficacy of BDS use in managing strictures in children are minimal. We report our experience with BDS use in 3 children with severe intractable esophageal strictures.
Case Series
Patients
Three pediatric patients with severe refractory esophageal strictures requiring frequent dilatations were managed with BDS at our hospital. Two patients (cases 1 and 2) had esophageal stricture as a result of caustic ingestion at age 16 and 18 months, respectively. BDS insertion was performed 7 and 11 years after caustic ingestion, respectively. They both had normal neurocognitive and medical background. Case 2 previously had a removable stent inserted, which was removed after migration into the stomach. The third patient (case 3) had congenital long-gap esophageal atresia (LGEA) corrected with Foker's technique. A stricture requiring dilatation developed 3 months after esophageal anastomosis; BDS insertion was performed 17 months after anastomosis. Median follow-up period was 23 (range 18–28) months.
All of the patients had severe proximal esophageal strictures requiring frequent dilatations under general anesthesia. Median number of dilatations before BDS insertion was 5 per year (range 5–10). The 2 cases with caustic ingestion each had >30 total dilatations before stenting, whereas the case of post-LGEA correction had 16 dilatations prestenting (Table 1).
Patient Characteristics and Outcomes
BDS, biodegradable stents; LGEA, long-gap esophageal atresia.
Procedure
BDS insertion followed a multidisciplinary discussion involving patients, family, pediatric surgeons, and interventional radiologist with the aim of achieving long-term symptom relief. Custom-made uncovered BDS (ELLA-CS, Hradec Kralove, Czech Republic) was used in all cases (Fig. 1). The stents were made of polydioxanone material that usually disintegrates in ∼12 weeks. 9 The stents were sized according to normal esophagus from previous dilatation. Sizes 14/12, 16/14, and 16/14 mm diameter and 40–50 mm length BDS were used. The procedure was performed under general anesthesia in the interventional radiology suite by an interventional radiologist. The esophagus was catheterized through the mouth using BMC catheter (Cook) and Sensor guide wire (Boston Scientific) under fluoroscopic guidance. An initial water-soluble contrast study was performed to assess stricture site, length, and severity. Balloon dilatation was then undertaken; the size of the balloon was chosen based on the diameter of the normal esophagus when distended with contrast. The BDS was mounted on delivery catheter, inserted, and deployed across the stricture. Check contrast study was performed at the end of the procedure to check the position and effect of the stent, and ensure no evidence of perforation (Fig. 2). A check X-ray was obtained 1 week after BDS insertion followed by contrast study at 3 weeks and endoscopy at 4–6 weeks postprocedure.
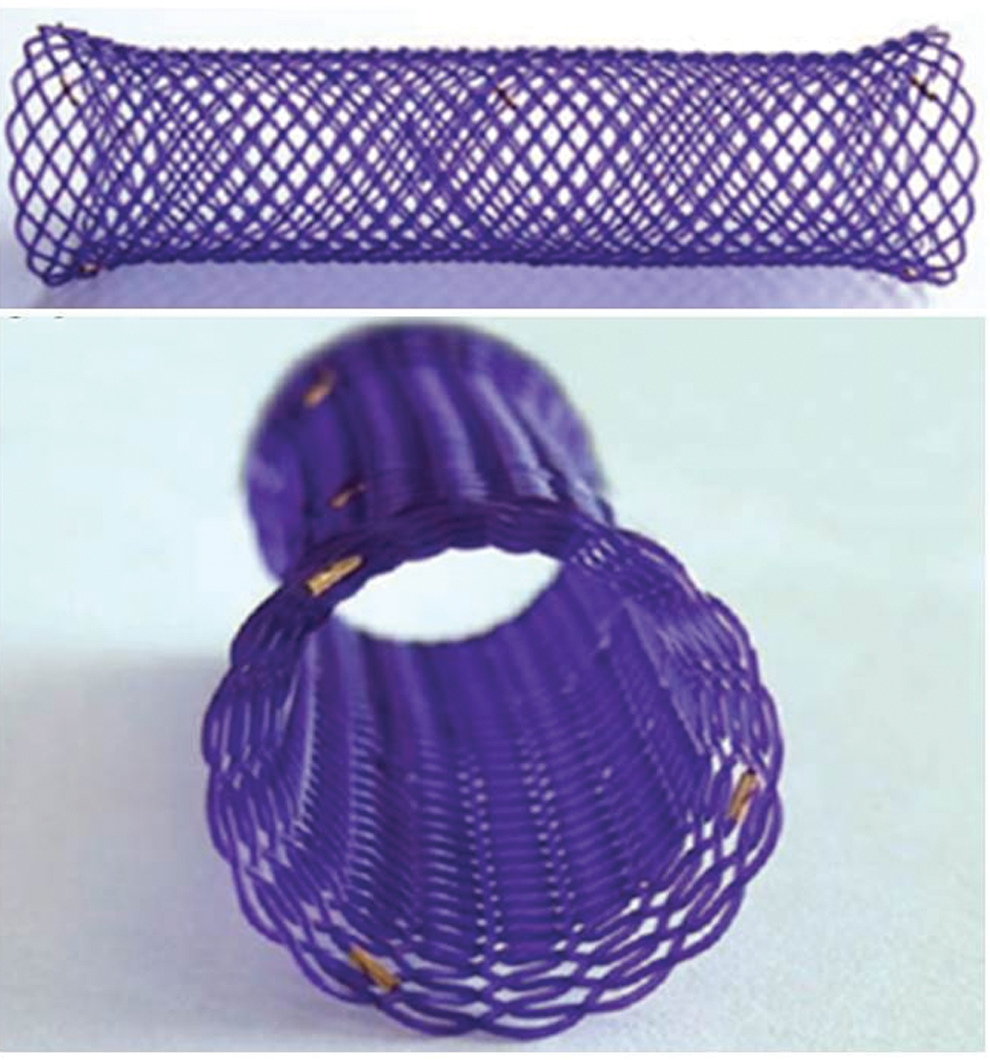
Biodegradable esophageal stent. 8
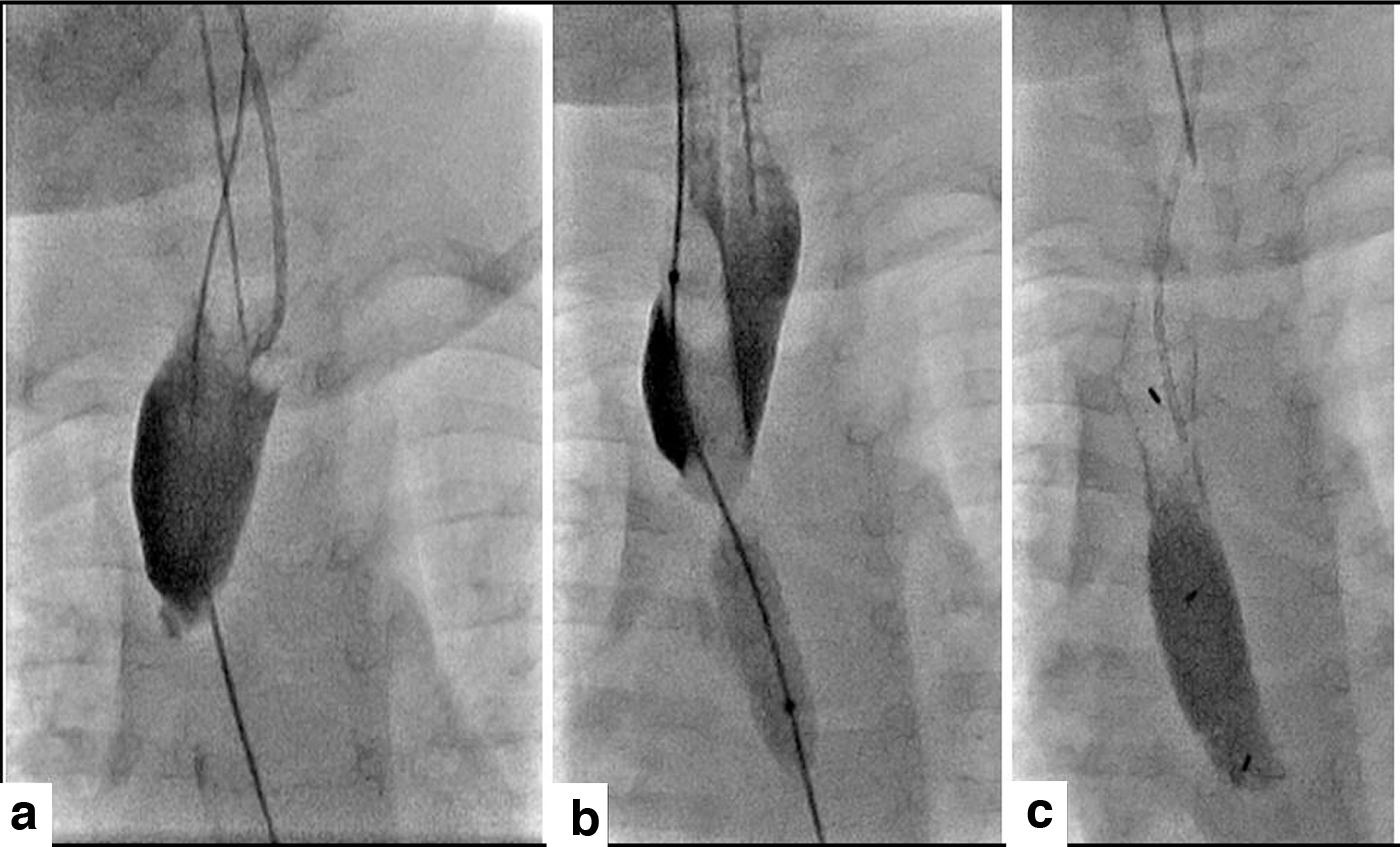
BDS insertion procedure:
Outcomes
Case 1 had minor complications with small-volume hematemesis and chest pain after procedure that required overnight admission for observation only. There was also early migration of the stent in case 1, requiring a second stent insertion 4 weeks later. The other two cases had no postoperative complication and were discharged home the same day. Stents were generally well tolerated without any long-term pain or reflux symptoms.
Stent insertion led to significant improvement in swallowing and they were able to tolerate normal diet immediately after. However, the symptom improvement was temporary, lasting 1–3 months in each case. Complete stent degradation occurred between 4 and 6 months. Case 3 had a second stent insertion 10 months after the first due to severe recurrence, but there was further stricture recurrence (Fig. 3).

Poor outcome observed in case 3:
Recurrent symptoms were as severe as prestent insertion in all of the cases. Need for dilatations remained unchanged after BDS. None had complete resolution of stricture/symptoms. In addition, all cases developed mucosal hyperplasia around the edges of BDS, which resulted in narrowing of the esophageal lumen and this itself contributed to their recurrent symptoms. The mucosal reactions eventually resolved with continued dilatations; however, the original stricture recurred.
Discussion
Although the advantage of avoiding the need for stent removal is attractive especially in pediatric practice, our experience with BDS use in managing children with refractory esophageal strictures is not favorable. All of the patients developed significant mucosal hyperplasia that contributed to the early recurrence of symptoms. In addition, the stent did not prevent the development of recurrent strictures long after the stent had completely degraded. They eventually needed as much and, in some cases, more general anesthesia and frequency of dilatations as they did before stenting.
Only four publications in English language reporting experience of BDS use for managing esophageal strictures in children were found based on our literature search. Two were case reports and two case series. Vandenplas et al. 10 reported their experience with BDS insertion in a 10-year-old, 6 weeks after caustic ingestion. Symptoms resolved completely after four poststent dilatations. BDS was used as the primary treatment option for a newly diagnosed stricture. This differs to the cases in our series, which were refractory strictures.
Karakan et al. 11 reported outcomes of BDS use in a series, including 2 children (ages 5 and 14 years) and 7 adults, with severe refractory esophageal strictures after caustic ingestion. Similar to our experience, both of the pediatric cases developed mucosal hyperplasia causing severe feeding difficulties. This, however, seem not to be as common compared with adults as only 1 out of the 5 adults had the complication. They suggested that this could be due to the size of the BDS as same stent diameter was used for their pediatric and adult cases. The patients in our series, however, had bespoke BDS made for them based on the diameter of their normal esophagus and they all developed mucosal hyperplasia. We suspect that this could be more to do with tissue reaction with the stent material rather than stent size. One of the 2 children in the series had persistent symptom as could only swallow semisolids at the end of the 2 year follow-up period.
Okata et al. 12 managed a child with severe esophageal stricture after LGEA repair using BDS. They also reported tissue reaction and severe stricture recurrence despite a total of four BDS insertions. Their patient eventually underwent stricture resection and end-to-end anastomosis. Alberca-de-las-Parras et al. reported BDS use in conjunction with mitomycin injection in 4 children with severe esophageal strictures (1 after caustic ingestion and 3 postesophageal atresia repair). 13 Two had associated bronchoesophageal fistula. Strictures reoccurred in 3 cases and 1 patient had complete stricture resolution but had persistent fistula requiring surgery. All four required further mitomycin treatment and/or surgery.
Conclusion
Recurrent severe strictures needing frequent dilatations or further interventions occurred in all the cases in our series and most of other published reports in children. Based on these early results, BDS is yet to be proven as an effective management option for refractory esophageal strictures in children.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.