
Abstract
Background:
Concomitant laparoscopic splenectomy and cholecystectomy (CLSC) is performed for concurrent pathologies of the spleen and gallbladder. This systematic review aimed to evaluate the available evidence on its indications, operative technique, and outcomes.
Materials and Methods:
The PubMed and Cochrane bibliographical databases were searched from the beginning of time (last search: December 6, 2019) for studies reporting on CLSC. The National Heart, Lung, and Blood Institute (NHLBI) quality assessment tool was utilized for the evaluation of eligible articles.
Results:
Eight studies met inclusion criteria and concerned collectively 108 patients (53 males and 55 females) with a mean age of 27.02 ± 20.48 years (mean, SD). The most common surgery indications were hereditary spherocytosis (38.9%) and sickle cell disease or β-thalassemia (32.4%). Laparoscopic cholecystectomy preceded splenectomy in the majority of cases (75%). A five-trocar approach was most frequently (89.8%) utilized. The mean operation duration was 170.18 ± 53.07 minutes (mean, SD). Resected spleen weight was 601.82 ± 386.02 g (mean, SD) and had a length of 18.74 ± 5.3 cm (mean, SD). The conversion rate was 2.7%, while 20.4% of included cases experienced postoperative complications. Most frequent ones included pulmonary infection (6.5%) and portal/splenic vein thrombosis (4.6%). No postoperative death was recorded. Mean hospitalization period was 5.43 ± 3.18 days (mean, SD).
Conclusions:
CLSC is a safe and feasible operation for simultaneous diseases of the spleen and gallbladder that require elective procedures. High-quality clinical trials are essential to further elucidate clinical evidence and standardize operative technique.
Introduction
Concomitant laparoscopic splenectomy and cholecystectomy (CLSC) was introduced in 1994 by Trias and Targarona 1 for the synchronous surgical management of coexisting pathologies of spleen and gallbladder. Despite advancements in laparoscopic surgery, no consensus has been reached regarding the technique and operative parameters of this procedure.2,3
Minimally invasive surgery is considered the gold standard for both spleen and gallbladder diseases. 3 Laparoscopic splenectomy (LS) was first reported in 1991 by Delaitre and Maignien 4 and currently is routinely implemented for spleen elective surgical procedures, especially concerning hematological disorders.5–7 On the contrary, laparoscopic cholecystectomy (LC), since its introduction in 1985, 8 is widely adopted as the optimal treatment approach for symptomatic cholelithiasis and cholecystitis. 9
Hematological diseases, such as hereditary spherocytosis, thalassemia, sickle cell disease, and idiopathic thrombocytopenic purpura, are often associated with symptomatic cholelithiasis, thus requiring frequently both splenectomy and cholecystectomy.10–12 They usually concern patients in childhood or early adulthood, and so, an improved cosmetic result is necessary and the wide abdominal incision of a conventional open approach should be avoided.13,14 In addition to minimal damage to the abdominal wall, CLSC is also reported to lead to less postoperative pain and faster recovery. 15
The objective of this study was to systematically review available literature regarding CLSC and to evaluate its indications, surgical technique, and outcomes.
Materials and Methods
Protocol and search strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines and in line with the protocol agreed by all authors. 16 Two investigators (I.K., E.K.) independently searched PubMed and Cochrane bibliographical databases (last search: December 6, 2019) using the following MeSH terms: “laparoscopic,” “cholecystectomy,” “splenectomy.” The title-abstract screening was performed using the Abstrackr tool. 17 A third investigator (D.S.) was consulted to settle any disagreements.
Inclusion and exclusion criteria
English-language literature published from the beginning of time that concerned concomitant LC and LS were included in this systematic review. Studies published in a language other than English, reviews, experimental studies, case reports and small case series with <5 patients, studies not presenting separate data for concomitant LC and LS, editorials, and letters to the editor were excluded from the present study.
Data extraction of eligible studies
A predefined data collection form was utilized for data extraction of all included studies. The number of patients, age, sex and surgical indication were recorded. Surgical technique characteristics (patient's position, trocar number and sites, part of operation performed first, structure mobilization, hilar vessel ligation, spleen removal method, and drains) were also collected. Furthermore, we gathered data concerning operation duration, intraoperative blood loss, need for transfusion, resected spleen weight and diameter, and conversion rate, where applicable. Data regarding the length of hospitalization, 30-day postoperative complications, and death rate were recorded.
Statistical analysis
Collected data were tabulated and analyzed using StataCorp 2015 (Stata Statistical Software: Release 14. College Station, TX: StataCorp LP). Continuous variables are presented as mean ± standard deviation, whereas categorical ones are summarized as valid percentages or frequencies. Pooled means and variances were calculated using aovsum STATA command. Formulas proposed by Hozo et al. 18 were utilized for the estimation of mean and variance of variables, where only median, range, and sample size were reported.
Quality assessment
Two researchers (I.K., E.K.) working independently evaluated the eligible studies using the quality assessment tool for case series studies developed by the National Heart, Lung, and Blood Institute (NHLBI) and Research Triangle Institute International. 19 The quality score ranges from 1 to 9; with 1–3 indicating poor quality, 4–6 fair quality, and 7–9 good quality. In the category assessing whether the follow-up period was long enough, the cutoff value was a priori set at 12 months following surgery.
Results
Literature search and eligible studies' characteristics
The literature search generated 253 studies. Eight studies met our inclusion criteria and were included in this systematic review.2,3,6,20–24 The detailed trial flow is shown in Figure 1. Eligible studies were published from 1999 to 2016 and 75% of them were published after 2007. Most studies originated from Italy (three studies, 37.5%), while one study came from each of the following countries: China, Japan, Greece, Saudi Arabia, and Turkey. Mean NHLBI quality assessment score was 7.13 ± 0.64 (mean, SD); 7 good-quality studies and 1 fair-quality study.
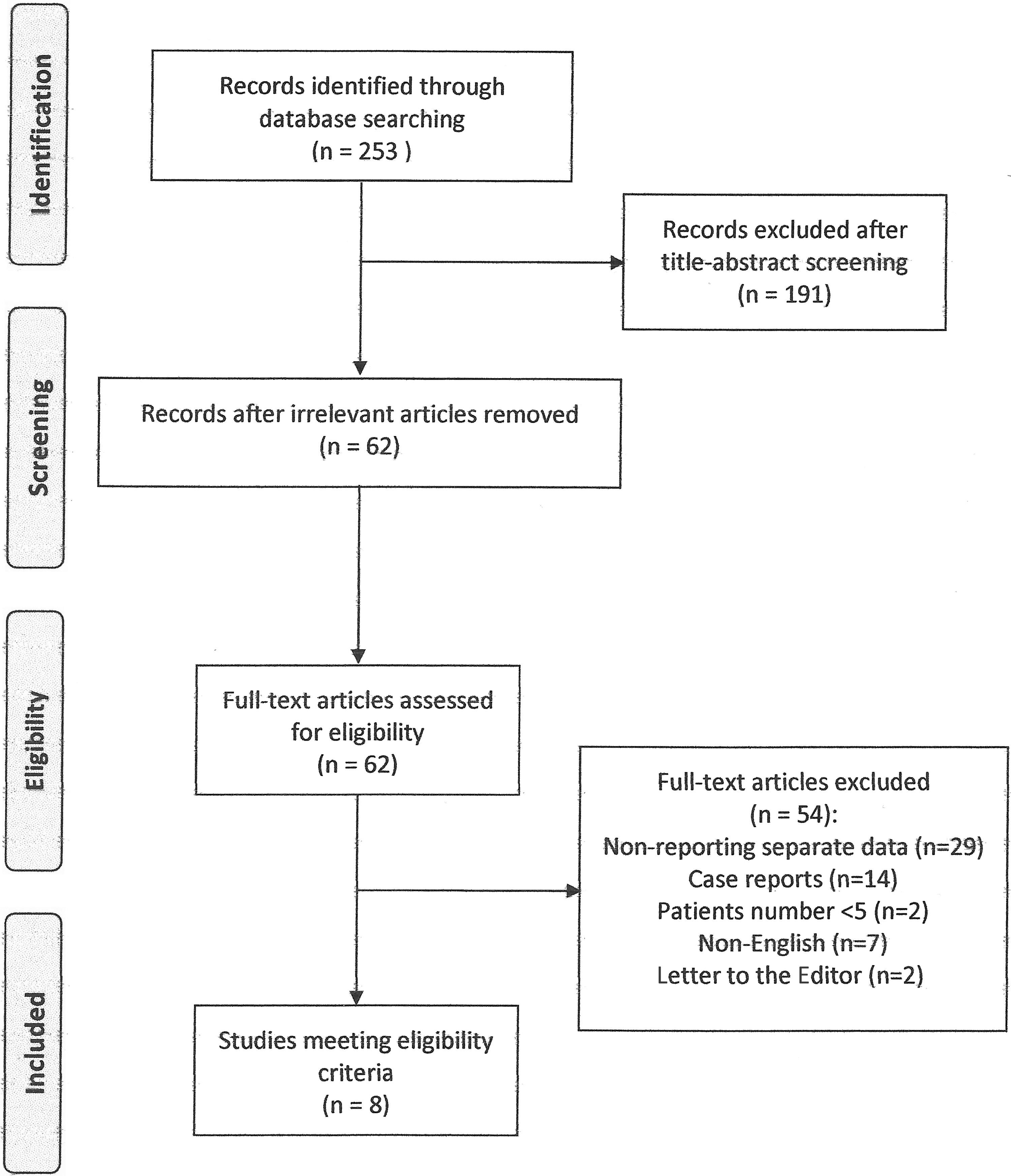
Trial flow diagram of this systematic review.
Patient characteristics
Included studies reported collectively on 108 patients, 53 males (49.1%) and 55 females (50.9%) with a mean age of 27.02 ± 20.48 years (mean, SD). The most frequent indications for operation were hereditary spherocytosis (38.9%) and sickle cell disease or β-thalassemia (32.4%). Other causes included liver cirrhosis complicated by hypersplenism and cholelithiasis (17.6%), idiopathic thrombocytopenic purpura (7.4%), autoimmune hemolytic anemia (1.9%), and 2 cases of combined cholelithiasis with splenic artery aneurysm (1.9%).
Surgical technique
In 75% of the studies, LC preceded LS, while in the remaining ones LS was performed first. In the majority of cases, the patient's initial position was right lateral or semilateral with left flank elevated at 30°–45°, while the operative table was tilted during surgery for the completion of both operative parts. Table 1 shows patient's position during each part of the operation for each included study. In the majority of cases (89.8%), a five-trocar approach was implemented, while a three-trocar and four-trocar approach was utilized at 5.6% and 4.6% of cases, respectively. Mobilization of the structures was performed using bipolar diathermy or ultrasonic scalpel, while hilar vessels were ligated utilizing the endostapler or electropolar sealing device. Detailed technical characteristics of eligible studies are presented in Table 2. In 96.2% of the available cases, the spleen was fragmented and a retrieval bag was used, while in 3.7% of cases, the spleen was removed intact. A drain was placed at the left subphrenic area in all the available cases, while a drain at the subhepatic space was utilized in 18.3% of available cases.
Patients' Position During Each Operative Part of Eligible Studies
LC, laparoscopic cholecystectomy; LS, laparoscopic splenectomy; N/A, not applicable.
Detailed Technical Characteristics of Each Study
N/A, not applicable.
Surgery outcomes
The mean duration of the operation was 170.18 ± 53.07 minutes (mean, SD). Resected spleen weighted 601.82 ± 386.02 g (mean, SD) and had a length of 18.74 ± 5.3 cm (mean, SD). An accessory spleen was found in 9 cases (8.3%). Mean blood loss was 118.68 ± 125.95 mL (mean, SD), and in 5 cases (4.6%) a transfusion was needed. In 3 cases (2.7%), a conversion to open surgery was decided due to excessive splenomegaly, lack of anatomical structure recognition, and bleeding from the splenic hilar vessels.2,20,23 In total, 22 patients (20.4%) experienced postoperative complications, with pulmonary infection (6.5%), portal/splenic vein thrombosis (4.6%), and postoperative bleeding (3.7%) being the most frequently encountered ones. Detailed postoperative complications of each included study are shown in Table 3. No postoperative death was reported. The mean hospitalization period was 5.43 ± 3.18 days (mean, SD).
Detailed Postoperative Complications per Eligible Study
N/A, not applicable.
Discussion
CLSC is indicated for the surgical management of diseases that affect both the spleen and the gallbladder. It was originally recommended 25 years ago and several techniques have been proposed through the years.3,25 To our knowledge, this is the most conclusive systematic review regarding CLSC, its indications, and the operative technique.
Several hematological diseases that lead to hemolytic anemia often affect both the spleen and the gallbladder. Benign disorders, such as hereditary spherocytosis, idiopathic thrombocytopenic purpura, and sickle cell disease, require splenectomy when conservative treatment fails, and a minimally invasive approach is the optimal alternative. 5 Furthermore, the resulting catabolic breakdown of heme leads to increased unconjugated bilirubin and the development of black pigment gallstones. 26 LC is indicated in patients with symptomatic gallstones, while the role of prophylactic surgery of asymptomatic patients remains a controversial issue. 10 About 8 of 10 of our included cases concerned such hematological disorders, with hereditary spherocytosis (38.9%) and sickle cell disease or β-thalassemia (32.4%) being the most frequent ones.
Liver cirrhosis complicated by portal hypertension results in hypersplenism and thus thrombocytopenia and leukopenia. 27 A splenectomy and devascularization or shunt surgery are essential for these patients to avoid the increased risk of variceal bleeding and bleeding tendency resulting from thrombocytopenia. 28 LS was contraindicated in such cases, but with recent advancements in minimally invasive procedures and instruments, LS is currently considered to be a feasible, safe, and effective procedure.29,30 Furthermore, Child–Pugh A and B patients suffering from symptomatic gallstones can safely undergo LC without any significant consequence in morbidity and mortality, whereas Child–Pugh C patients necessitate a careful preoperative evaluation.31–33 Wang et al. concluded that CLSC is a safe treatment approach for Child–Pugh A and B cirrhotic patients presenting with symptomatic gallstone disease and hypersplenism. 20
CLSC consists of two parts, LS and LC, performed consecutively. Wang et al. advocated that LC should be the initial one mainly due to its low conversion rate. 20 Our findings are in accordance with that, as 75% of the included studies performed LC first. Furthermore, the placement of the patient at a right lateral position with the left side elevated at 30°–45° is preferable and, during the operation, the table is tilted to set the patient at the optimal position for each part of the operation.2,3,6,23 The right lateral position gives an advantage for the excision of mildly enlarged spleens since it offers a better view of the splenic hilum and vessels.34,35
Most authors agree that a five-trocar approach is favorable for a better view of the operating field and improved recognition and exposure of the implicated anatomical structures.2,20–24 As far as the retrieval of the specimens is concerned, the gallbladder is typically extracted through the umbilical port, while the spleen can be placed in an endobag, fragmented, and then removed through the largest port. 23 In the case of advanced splenomegaly, a port incision can be extended and spleen removed through it. 3 Mobilization of the structures can be performed using bipolar diathermy or ultrasonic scalpel, while hilar vessels can be dissected with the endostapler or electropolar sealing device, on the condition that the pancreatic tail has been previously isolated.6,36 A drain at the left subphrenic area is essential at least for the 1st postoperative day.2,20
Operative time, as it was expected, is significantly prolonged compared with the one of each individual operation.5,37 As far as the spleen size is concerned, a laparoscopic approach is safe and comparable with that of a normal-sized spleen for a weight of <2000 g. 35 Mean blood loss and the need for transfusion rate of CLSC were comparable with those of LS. 20 The conversion rate of about 3% is considered to be mainly affected by LS rather than the LC part and is related to excessive splenomegaly, intraoperative bleeding, and difficult recognition of the anatomical structures.2,20,23 The mean hospitalization period was similar to the one of LS. 5
Approximately 1 of 5 patients experienced minor or major postoperative complications, whereas no postoperative death was recorded. Portal/splenic vein thrombosis is a severe complication, after LS, that could lead to devastating consequences. The longer operative time of CLSC and the consequent longer exposure to pneumoperitoneum could be a potential risk factor for its occurrence, as it reduces the blood flow in the portal system. 2 A routine postoperative screening is advocated by some researchers for the prompt diagnosis and treatment of this clinical entity. 38
In conclusion, CLSC is a safe and feasible operation for diseases that affect both the spleen and the gallbladder, while its complications and conversion rate are comparable with the ones of each operation. Further high-quality clinical trials are necessary to strengthen available evidence and lead to a standardization of the operative technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.