
Abstract
Purpose:
The significant reduction in childhood cancer mortality has allowed for greater emphasis on survivorship issues, including infertility. This study evaluated the participation of pediatric surgery training programs in fertility preservation (FP) and exposure of fellows to adnexal cases.
Materials and Methods:
A survey was distributed to pediatric surgery fellowship program directors in the United States and Canada through email. Questions focused on FP participation, operative cases, FP program limitations, and fellow completion of adnexal cases.
Results:
Survey participation was 49% (28/57). Overall, 43% (12/28) of training programs report participation in FP initiatives. Of those who participated, the most common procedures performed were testicular tissue biopsy (58%) and testicular sperm extraction (42%) in males, and surgical transposition of the ovaries (83%) and laparoscopic oophorectomy (67%) in females. The greatest cited limitations on participation were that FP was another department's responsibility (50%) and lack of multidisciplinary team (31%). Notably, lack of operative experience in benign ovarian and testicular procedures (0%) was not a limitation. All programs, regardless of participation in FP, noted that their fellows performed benign and malignant adnexal cases.
Conclusion:
Less than half of pediatric surgery training programs participate in FP initiatives, despite adequate advanced minimally invasive training of fellows to perform these procedures.
Introduction
The overall survival for childhood cancer has now reached over 80%. 1 This increase in survival has allowed for a shift in focus toward long-term quality-of-life issues, including treatment effects on future fertility, which has been shown to be a priority for patients and their families.2,3 Unfortunately, many benign and malignant conditions require gonadotoxic treatments that may threaten a child's future fertility.4–7 Currently, the only pretreatment fertility preservation (FP) options for prepubertal children are testicular tissue cryopreservation (TTC) and ovarian tissue cryopreservation (OTC). Both procedures involve the surgical removal of gonadal tissue.8,9 OTC and TTC can be performed without intraoperative complications and little to no postoperative morbidity, and patients are able to resume their cancer therapy without delay.10,11 Although TTC is considered experimental, the American Society for Reproductive Medicine (ASRM) has deemed OTC nonexperimental. 12
Multiple societies recommend discussion about the effect of treatment on fertility. Specifically, ASRM and American Association of Pediatrics and American Society for Clinical Oncology recommend discussions as early as possible so that the most amount of options are available to the patient and family.13–15 The Children's Oncology Group endorses the recommendations of American Society for Clinical Oncology. In addition, the National Comprehensive Cancer Network recommends that adolescents and young adults who are interested in FP be given a referral to an FP clinic within 24 hours. 16 Given that the best chance of future successful utilization of cryopreserved ovarian or testicular tissue may be when it is frozen before treatment begins, pediatric surgeons are often involved early in a child's comprehensive cancer care. This study sought to evaluate the participation of pediatric surgery training programs in FP and the exposure of pediatric surgery fellows to operative adnexal and testicular cases.
Materials and Methods
Lurie Children's Hospital's Institutional Review Board approval (IRB# 2016-599) was obtained before survey distribution. An electronic survey was distributed to pediatric surgery fellowship program directors in the United States and Canada through email correspondence with the assistance of REDCap from 2016 to 2018. Program directors were chosen for distribution of this survey with the assumption that their focus on fellow education and training would lead them to be aware of various programs in their department. Also, program directors have access to their fellows' case logs. Questions were related to participation in FP initiatives, FP operations (e.g., ovarian transposition, oophorectomy, testicular sperm extraction [TESE], and testicular tissue biopsy), collaboration with other departments, limitations to department participation, and the involvement of fellows in adnexal surgery during training (Supplementary Data). The number of prompted questions varied depending on question-specific responses, between 12 and 15 in total. Questions related to participation in FP surgery and department limitations were formatted as “choose all that apply” and were not limited to single responses. The remainder of the questions were single-answer responses. Given the small amount of total training programs, there were no demographic questions asked that could link specific departments to their answers. Therefore, all survey answers were kept anonymous.
REDCap was utilized for data collection and export. Descriptive statistics were calculated using proportions. Data merging and statistical analysis were performed with IBM SPSS Statistics for Windows, version 19.
Results
The survey was distributed to 57 pediatric surgery fellowship training program directors with a 49% (28/57) response rate. Of respondents, 43% (12/28) of training programs report participation in FP initiatives. The most common collaborating departments include pediatric oncology (92%, 11/12), pediatric and adolescent gynecology (50%, 6/12), and adult endocrinology (33%, 4/12).
Of training programs with FP initiatives, the most common procedures performed for males were testicular tissue biopsy (58%, 7/12) and TESE (42%, 5/12) (Table 1). However, only 50% (6/12) of departments reported performing at least 1 FP procedure for males in the last year (33% [4/12] 1–5 procedures, 17% [2/12] 6–10 procedures, 0% greater than 10 procedures).
Procedures Performed for Fertility Preservation in Males at Participating Programs
FP, fertility preservation.
For female FP, the most common procedures performed were surgical transposition of the ovaries (83%, 10/12) and laparoscopic oophorectomy (67%, 8/12) (Table 2). Over the last year, 75% (9/12) of training programs performed at least 1 procedure for female FP (58% [7/12] 1–5 procedures, 0% 6–10 procedures, 17% [2/12] greater than 10 procedures).
Procedures Performed for Fertility Preservation in Females at Participating Programs
FP, fertility preservation.
Of training programs without FP initiatives (57%, 16/28), the most common other departments who do participate are pediatric hematology and oncology (38%, 6/16) and pediatric and adolescent gynecology (31%, 5/16). The most commonly cited limitations were that FP was another department's responsibility (50%, 8/16) and the lack of a multidisciplinary team (31%, 5/16). In addition, one department cited lack of funding. Notably, unfamiliarity with technical aspects of cryopreservation (6%, 1/16) and lack of operative experience with benign ovarian and testicular procedures (0%, 0/16) were not considered limitations to involvement in FP (Fig. 1)

Department limitations to fertility preservation participation.
All departments (28/28) responded that their fellows perform benign and malignant adnexal cases, regardless of participation in FP. During fellowship, most trainees logged greater than 10 adnexal cases (39% performed 11–20 cases and 25% performed 21–30 cases) (Fig. 2)
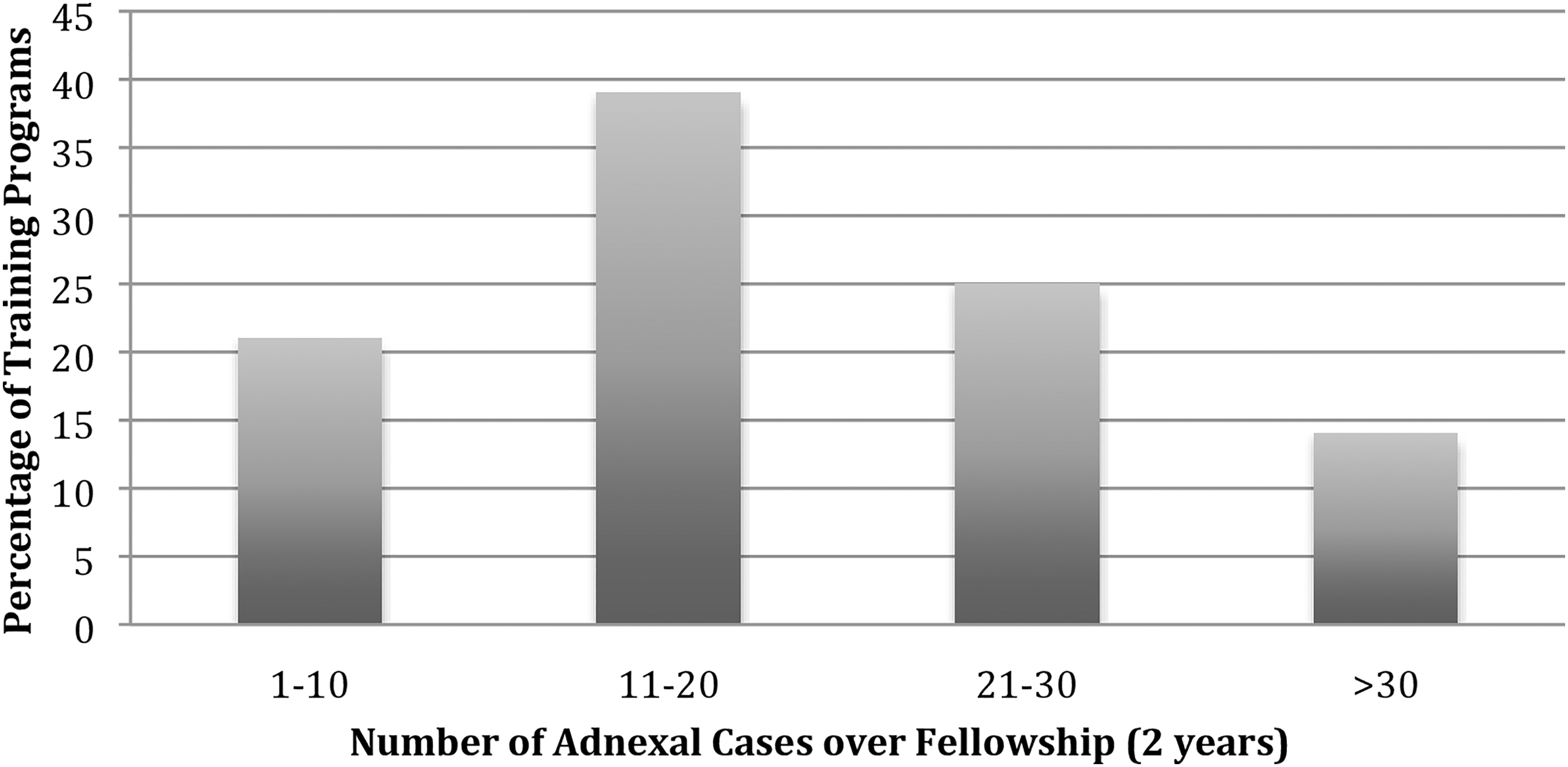
Number of adnexal cases for pediatric surgery fellows over fellowship (2 years).
Discussion
Our study suggests that less than 50% of pediatric surgery departments with fellowship training programs participate in FP initiatives. The most common procedures performed are testicular tissue biopsy, transposition of the ovaries, and laparoscopic oophorectomy. For programs that do not participate in FP, the most cited reasons were that FP was the responsibility of another department and lack of a multidisciplinary team. Importantly, there were no programs that cited lack of tissue handling or cryopreservation laboratory techniques or training in ovarian and testicular procedures as limitations. Furthermore, over 80% of fellows perform more than 10 adnexal cases during their training, where ∼40% perform greater than 20 cases. Currently, the Accreditation Council for Graduate Medical Education (ACGME) requires a minimum of five adnexal cases during fellowship. 17 Although most training programs do not participate in FP, pediatric surgeons commonly perform oophorectomy and testis biopsy for other indications in infants, children, and adolescents.
A fundamental aspect of pediatric surgery training is the acquisition of advanced minimally invasive surgery skills for a variety of abdominal and pelvic conditions in pediatric patients. 17 Also, there is particular emphasis paid to delicate tissue handling during training. It is for these reasons that the American Academy of Pediatrics recommends a pediatric surgeon, or pediatric surgical subspecialist, be responsible for the surgical care of any child younger than 5 years and younger than 12 years, who is receiving a minimally invasive procedure. 18 Proficiency in advanced minimally invasive surgical techniques is applicable to FP surgery because the gonadal tissue is uniquely procured for future fertility and hormone restoration and treated as tissue for transplant. 19 Poor handling of the tissue may have implications on future restoration outcomes. In a single-institution study of OTC, 92% were performed laparoscopically. Of the remaining cases that were performed with an open approach, a concurrent tumor resection was planned. 11 As FP initiatives continue to develop, pediatric surgeons may find themselves asked to perform FP procedures since they are trained in advanced minimally invasive surgery and equipped with the technical skills to operate on small children.
Beyond the purely technical aspects of FP surgery, it is important to recognize the therapeutic relationship developed between pediatric surgeons and the oncology patients whom they treat, in particular, those children diagnosed with solid tumors. For patients who eventually will require surgical resection, pediatric surgeons are a key part of the multidisciplinary oncology team and have the opportunity to establish rapport with patients and their families to broach sensitive topics such as FP in the face of other oncologic treatments. In addition, pediatric surgeons have the capability and training to perform necessary ancillary procedures that are essential to comprehensive oncology care, including central venous catheter placements, gastrostomy tube placements, lymph node dissections, and tumor resections. Recent studies have demonstrated that over 70% of OTC and TTC patients undergo an additional procedure during the same anesthetic as their FP surgery.10,11 Because of the multifaceted skills of a pediatric surgeon, it is sensible to consider them an integral part of FP initiatives.
The implication of these data may be that pediatric surgery departments have organizational limitations to forming an FP program, but not a technical limitation. Similar to our study, a recent Dutch study, evaluating barriers to FP in a system where insurance universally covers these procedures, demonstrated that at an organizational level, there is disagreement about which department is responsible for fertility discussions. 20 While it is true that forming a, FP program requires more than just technical expertise, 21 it can be done with proper support and adequate resources as highlighted in a recent, well-organized article from the Pediatric Initiative Network (PIN) of the Oncofertility Consortium. The article specifically highlights the need for a highly motivated multidisciplinary team, identification of target populations, and establishment of experimental ovarian and TTC protocols under IRB approval. 22
It is not possible, however, for all pediatric surgery departments with training programs to establish an FP program. Nonetheless, it is important for their fellows to be adequately educated and trained in performing FP procedures. At the time of the survey, there were no published resources in pediatric surgery literature for FP and this survey did not address FP didactic education; however, this could represent an important subsequent study to evaluate utilization of present resources. Resources have become available through the American Pediatric Surgical Association, such as the Fertility Preservation NaT chapter, 23 which can be combined with various oncology-based didactic lectures.
Simulation-based training modules have been useful for other operations, including common bile duct exploration, 24 thoracoscopic esophageal atresia with tracheoesophageal fistula repair, thoracoscopic pulmonary lobectomy, laparoscopic duodenal atresia repair, 25 and laparoscopic pyloromyotomy. 26 This technique could also be developed by leaders in the field for laparoscopic oophorectomy specifically for FP and used in conjunction with workshops at international conferences. There is need for collaboration between programs of different sizes and capabilities. Any fellow, or established surgeon, with interest in incorporating FP into their practice should seek out training and additional experience with established programs.
We acknowledge several limitations to the generalizability of this study. First, we received a survey response rate of 49%, so it may be difficult to draw major conclusions. It is feasible that we missed training programs that do have FP programs, which would have increased our overall FP participation rate. In addition, respondents might have been discouraged to complete the survey if they were unsure as to whether their department had an FP program. We intentionally did not include program identifiers, given the small number of pediatric training programs, but this omission did limit our ability to characterize departments for which there are FP programs. Although not specifically asked in this study, surgical oncologists have been shown to lack awareness of FP, which is a major barrier of starting an FP program. 20 Additional studies are needed to assess surgeon-specific knowledge of FP.
Regardless of these limitations, we have identified an area for improvement in current pediatric surgical training. As pediatric FP becomes integrated into a child's comprehensive cancer care, there will likely be an increase in the number of pediatric patients who are candidates for OTC and TTC. The next generation of pediatric surgeons should actively participate in FP by being aware of FP options for these patients and by safely performing OTC and TTC when they are indicated.
Conclusion
Ovarian and TTC are the only pretreatment FP options for prepubertal patients and both procedures require surgical removal of gonadal tissue for cryopreservation. Our survey indicates that less than half of pediatric surgery training programs surveyed may be involved in FP, despite adequate advanced minimally invasive training of fellows to perform these procedures. There is opportunity for research in video- and simulation-based education, as well as multicenter collaboration for ongoing translational and outcome research.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.