
Abstract
Background:
The role of the laparoscopic approach to D2 gastrectomy for gastric cancer remains controversial. The aim of this study was to compare the operative and short-term oncologic outcomes of laparoscopic versus open resections.
Methods:
Patients who underwent potentially curative D2 gastrectomy between 2017 and 2019 were retrospectively reviewed. Patients were randomly matched on 1:1 basis for age and extent of surgery (total versus subtotal gastrectomy, and additional organ resection). Exclusions included emergency or palliative surgery. The learning curve for laparoscopic resections was included. Analysis was conducted on intention to treat basis. The outcomes were reported as median (range) or per cent as appropriate.
Results:
Among 78 patients who had undergone potentially curative gastrectomy 36 were matched. The groups were comparable for age, sex, American Society of Anesthesiologists (ASA) score, preoperative serum albumin and hemoglobin, body mass index, frequency of previous abdominal surgery, anatomic distribution of disease, extent of gastrectomy, need for additional resection, and disease stage. There was one conversion to open surgery. Although laparoscopic surgery required longer operating time (393 versus 218 minutes, P < .001), it was associated with less blood loss (100 versus 200 mL, P = .001) and shorter hospital stay (3.0 versus 7.5 days, P < .001). There were no significant differences in the rates of clinically significant complications, mortality, readmissions, reoperations, lymph node retrieval, and R1 resections.
Conclusions:
The laparoscopic approach to potentially curative D2 gastrectomy for gastric cancer is associated with less operative trauma and quicker recovery while offering an equivalent oncologic resection.
Introduction
While the incidence of gastric cancer is gradually declining, it is the fifth most common cancer worldwide and the third most common cause of cancer-related worldwide according to GLOBOCAN 2018 data. 1 The recent report of the Jordan Cancer Registry for 2016 shows gastric cancer to be the ninth most common among Jordanians. Despite the rising adoption of the laparoscopic approach to resection of advanced gastric cancer, particularly in the East where the incidence of this disease is high, 2 its potential benefits over open surgery remain uncertain. 3 The aims of this study were to establish whether the laparoscopic approach to D2 gastrectomy, in a setting where the introduction of laparoscopic techniques to gastric cancer resection is recent (learning curve included), offers advantages over open surgery in terms of postoperative recovery and to evaluate its operative and short-term oncologic safety.
Materials and Methods
Ethics
The Institutional Ethics Review Board approved this study.
Patients and procedures
All patients who underwent potentially curative D2 gastrectomy for gastric cancer at our Cancer Center between May 2017 and November 2019 were identified from the prospective cancer registry database, and their electronic medical notes were retrospectively reviewed. Patients were managed in a multidisciplinary setting.
The laparoscopic surgery was performed by 1 surgeon experienced in laparoscopic hepato-pancreato-biliary and bariatric surgery, and this reported experience included his learning curve with laparoscopic D2 gastrectomy for gastric cancer; he adopted a totally laparoscopic approach to resection in “all comers” with intracorporeal anastomosis and with extraction of the specimen through a Pfannenstiel incision. Two other surgeons experienced in open D2 gastrectomy (more than 100 procedures) performed open resections through a midline incision. The reconstruction technique of the gastrointestinal tract included either a retrocolic or antecolic Roux-en-Y or loop gastrojejunostomy after subtotal gastrectomy and a retrocolic or antecolic Roux-en-Y esophagojejunostomy after total gastrectomy according to each surgeon's discretion.
The laparoscopic surgeon adopted a more agile approach to enhanced recovery after surgery (ERAS); epidural catheters for analgesics delivery were not utilized, oral water was introduced the evening after surgery, the nasogastric tube (if it was not removed at the end of surgery) and the urinary catheter were removed on day 1 and free oral fluid intake allowed along with regular oral analgesia with discontinuation of patient-controlled opiate analgesia, a liquid diet established on day 2, and abdominal drain(s) removed on day 2 or 3 if drain amylase was not elevated more than three times that of serum amylase level.
Methods
Patients who underwent elective and potentially curative D2 gastrectomy for gastric cancer were included, while those who underwent emergency or palliative surgery or resection for indications other than gastric cancer were excluded. Patients who underwent laparoscopic resection were randomly matched to those who underwent open surgery on 1:1 basis for age (±5 years) and the extent of surgery (total versus subtotal gastrectomy, and additional organ resection). Data were extracted by two independent reviewers using a standardized collection Excel sheet.
The primary outcome of this study was the primary hospital stay, while secondary outcomes included operating time, intraoperative blood loss, frequency of prolonged hospital stay (>7 days), readmissions, total hospital stay (including duration of readmissions within 30 days of surgery), the rates of postoperative clinically significant 30-day complications (defined as Clavien–Dindo grades III or more), 4 30-day mortality, and R0 resections, as well as the count of lymph nodes retrieved.
Statistical analysis
Analysis was carried out on intention-to-treat basis, thus including conversions from laparoscopic to open surgery in the laparoscopic group. Data were analyzed using the software package SPSS 23 (Chicago, IL). Comparison between groups was performed using the Mann–Whitney U test and the χ 2 test and the results were expressed as medians and (range) or number (per cent) as appropriate. Significance was accepted at the 5% level.
Results
The study profile chart is shown in Figure 1. A total of 78 patients (Laparoscopic: 24 and Open: 54) were identified to have undergone a gastric resection. In the open surgery group, 5 patients were excluded for the following reasons: emergency surgery (n = 2), palliative resection (n = 2), and wedge resection (n = 1). In the laparoscopic surgery group, 5 patients were excluded for the following reasons: proximal gastrectomy for gastrointestinal stromal tumors (n = 2), palliative resection (n = 2), and completion gastrectomy (n = 1). The final random matching included 36 patients (Laparoscopic: 18 and Open: 18).
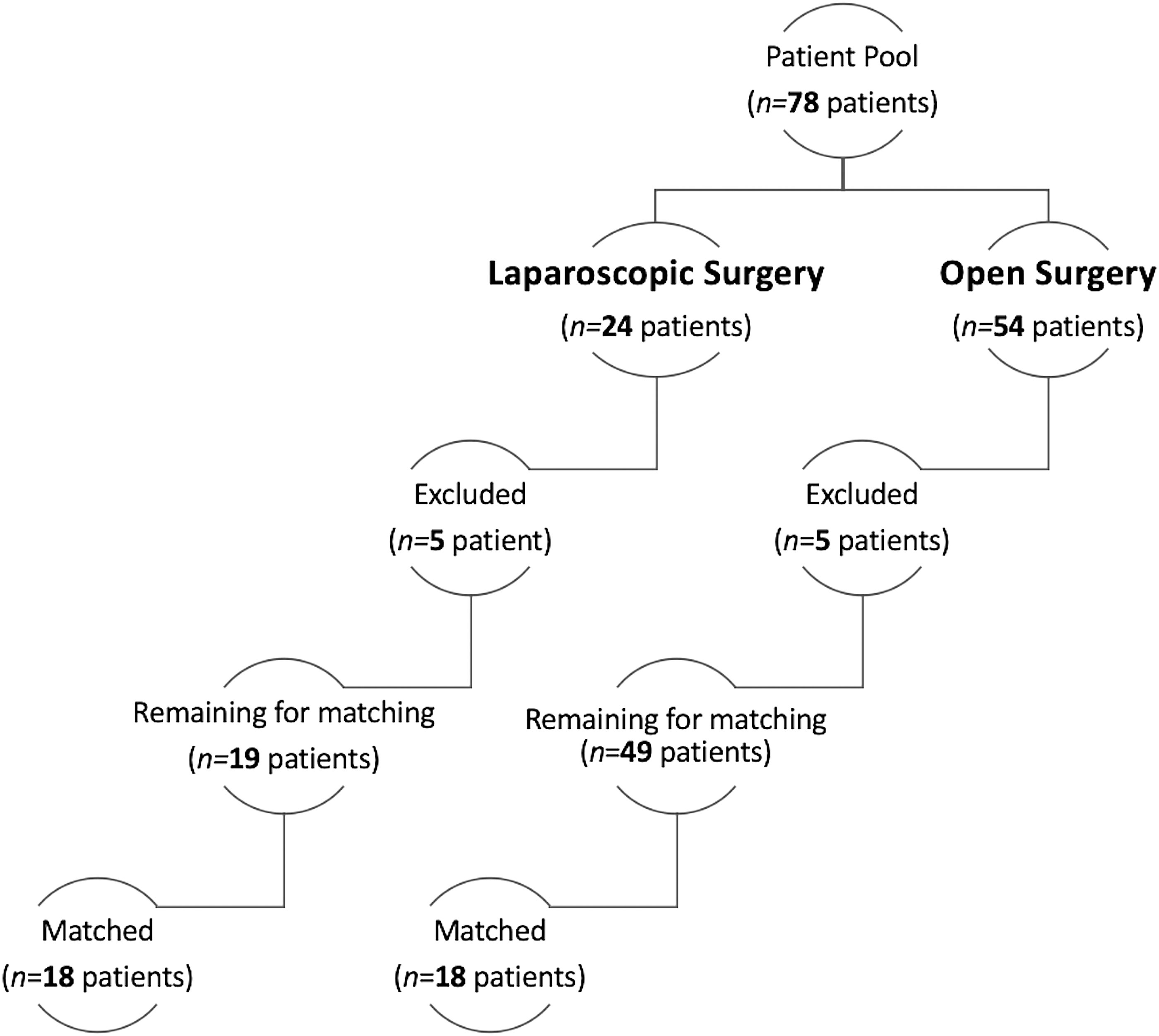
The study profile chart displaying the total number of patients considered for the study, the excluded patients and the final matched population of laparoscopic versus open D2 gastrectomy.
The groups were comparable for age, sex, American Society of Anesthesiologists (ASA) score, preoperative serum albumin and hemoglobin, body mass index (BMI; kg/m2), frequencies of subjects with obesity (BMI ≥30 kg/m2), underweight (BMI <18.5 kg/m2), previous abdominal surgery, the extent of gastrectomy (total or subtotal distal gastrectomy), whether additional organ resection was needed, the anatomic distribution of disease, and the American Joint Committee for Cancer (AJCC) disease stage (Table 1).
Details of Patients, Surgery, and Disease
Data shown represent median (range).
Preoperative clinical stage I.
ASA, American Society of Anesthesiologists; AJCC, American Joint Committee for Cancer 8th edition; BMI, body mass index.
The outcomes are summarized in Table 2. There was one conversion to the open surgery (5.6%) due to bleeding. Although the operating time for laparoscopic surgery was significantly longer, it was associated with significantly less blood loss, shorter primary hospital stay and total hospital stay (that included readmissions within 30 days of surgery), and less likelihood of prolonged hospital stay. There were no significant differences either in the need for blood transfusion, duration of intermediate/intensive care stay, rates of overall complications, clinically significant complications, readmissions, reoperations, mortality and R0 resections, or in the counts of lymph nodes retrieved. The postoperative complications are listed in Table 3. One patient in the laparoscopic surgery group, a 67-year-old woman, underwent relaparoscopy on day 2 and release of retrocolic Roux limb obstruction at the site of closure of the transverse mesocolic defect and was discharged 2 days later.
Operative and Early Oncologic Outcomes
Data shown represent median (range).
Postoperative Overall and Clinically Significanta Complications
Data shown represent number of patients (%).
Discussion
This matched comparative study demonstrated that the laparoscopic approach to elective D2 gastrectomy for gastric cancer offered advantages over open surgery in terms of reductions in intraoperative blood loss and primary and total hospital stay despite the longer operating time. Moreover, laparoscopic surgery offered a safe oncologic resection with equivalent R0 resections and lymph node retrieval rates.
Although a meta-analysis of 26 studies that included one randomized controlled trial (RCT) in the 2015 demonstrated some advantages to the laparoscopic surgery, including significant reductions in blood loss and hospital stay as well as faster recovery, 2 a recent meta-analysis 3 of five RCTs of laparoscopic versus open gastrectomy for advanced gastric cancer (n = 2157 patients) reported similar operative outcomes, including blood loss (103 versus 145 mL), 30-day clinically significant morbidity (2.7% in each group), type of complication, mortality (0% in both groups), and hospital stay (mean 9.6 versus 10.4 days). Despite this uncertainty as to whether the laparoscopic approach offers advantages over open gastrectomy for advanced gastric cancer in terms of postoperative recovery, it is not inferior to open surgery as far as the adequacy of oncologic resection. An equivalent lymph node retrieval rate was reported in both the case-matched comparative studies 2 and the RCTs (mean, 34.6 versus 33.9 nodes) 3 ; only one RCT reported on overall survival at a mean follow-up of 22 months with equivalent results. 5
Of note, the duration of the postoperative hospital stay reported in the RCTs after laparoscopic gastrectomy (mean, 9.6 days) 3 was considerably longer than that reported in our current study (median, 3 days). While this difference in hospital stay might be related to cultural differences, the laparoscopic-assisted approach adopted in all of these trials,5–9 whereby an ∼7–10 cm incision is made in the upper abdomen to reconstruct the gastrointestinal tract, might have contributed; this is in contrast to the total laparoscopic approach adopted in our study. Moreover, the active adoption of an agile ERAS by the laparoscopic surgeon in the current study might have played a role; a recent meta-analysis of randomized and nonrandomized trials found that the integration of ERAS in the perioperative care of gastric cancer surgery significantly shortened postoperative hospital stay (weighted mean difference of 2.5 days), compared with conventional care. 10 The concern that early discharge from hospital after laparoscopic surgery could result in higher readmission rates was not substantiated; like others,11–13 we observed no difference in readmission rates between the laparoscopic and open approaches to gastrectomy for gastric cancer (there was none in the laparoscopic group of the current study).
The only clinically significant postoperative complication encountered in the current study was that of a retrocolic Roux limb obstruction at the level of the transverse mesocolic defect after laparoscopic total gastrectomy that required a relaparoscopy. Nonetheless, the rates of severe postoperative complications and overall complications after laparoscopic D2 gastrectomy in the current study were comparable to those in the collective meta-analysis of five RCTs by Beyer et al. 3 (5.6% versus 2.8%, P = .407 and 16.7% versus 14.3%, P = .467).
The lymph node retrieval is a surrogate marker of adequacy of oncologic resection. In gastric cancer, a minimum of 15 lymph nodes in the resected specimen is considered essential for accurate staging and to avoid stage migration. 14 The adequacy of the oncologic resection in the current study is demonstrated by the high lymph node retrieval rate (median, 40.5 and 31.5 in the laparoscopic and open surgery groups respectively), the absence of inadequate lymphadenectomy (node counts <15) and the very low positive resection margin rates (0% and 11% in the laparoscopic and open surgery groups respectively). Lee and Kim 15 demonstrated that a surgeon experienced in open gastrectomy can achieve an adequate lymphadenectomy that is comparable to what is accomplished by open surgery even during the learning curve of laparoscopic D2 gastrectomy. In the current study, we have demonstrated that an adequate D2 lymphadenectomy can be accomplished during the learning curve of laparoscopic gastrectomy if the surgeon is experienced in laparoscopic lymphadenectomy for hepatobiliary cancers. Previous studies suggested that the learning curve for laparoscopic-assisted D2 distal gastrectomy, judged by the number of cases needed for the operating time to plateau, is ∼40 cases, potentially equaling that of open surgery by experienced surgeons.16–18 However, the learning curve for a totally laparoscopic D2 gastrectomy, such as that reported in the current study, can range from 20 cases for distal gastrectomy 19 to 100 cases for total gastrectomy. 20
Whether higher lymph node retrieval than the recommended minimum of 15 nodes could further improve gastric cancer staging and survival and where the point of diminishing could be are issues that remain controversial. In a Korean study of 575 patients with advanced gastric cancer, significantly better 5-year survival rates were observed with each group of higher lymph node retrieval (15–25 versus >25 nodes, and 15–39 versus ≥40 nodes). 21 A Japanese study of 1289 patients with resected gastric cancer suggested that retrieval of ≥25 lymph nodes was needed to avoid stage migration in patients with pathological stages II and III. 22 An analysis of 25,289 patients from an international joint database of the Surveillance, Epidemiology, and End Results (SEER) program (n = 13,932) and the Yonsei University Gastric Cancer (n = 11,358) reported a maximal survival advantage with a minimum of 29 lymph nodes retrieved during gastrectomy for gastric cancer. 23 While the survival advantage with higher lymph node yield might be more relevant to patients with node-positive gastric cancer, this concept seems to hold true in patients with node-negative advanced (T3/T4) gastric cancer; based on analyses of overall survival, one study recommended ≥19 node harvest 24 while another supported >15 nodes and found no survival advantage for lymphadenectomy of >25 nodes. 25
The limitations to the current study include its retrospective and nonrandomized nature, its relatively small sample size compared to studies arising from the East where gastric cancer is much more common, the study's single-center design, and the involvement of one laparoscopic surgeon experienced in laparoscopic hepato-pancreato-biliary cancer surgery. However, the well-matched, comparative, study design and inclusion of the laparoscopic surgeon's learning curve with this procedure in comparison to the well-established experience of surgeons performing open gastrectomy supports the study conclusions. Other markers of postoperative recovery such as time to first flatus, bowel motion, and oral diet could not be reliably retrieved retrospectively. Furthermore, the current study did not report long-term oncological outcomes due to the relatively short follow-up; however, the comparable pathology results such as those we reported might be expected to yield equivalent long-term oncologic outcomes.
In conclusion, the present case-matched analysis comparing the laparoscopic and open approaches to D2 gastrectomy for gastric cancer demonstrated benefits to laparoscopic surgery in terms of reduction in operative trauma despite longer operating time as well as reductions in primary and total hospital stay.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.