
Abstract
Background:
The standard treatment for esophageal carcinoma is extensive resection of the tumor and esophagogastric anastomosis despite the high incidence of related anastomotic complications, such as stricture and leakage. Thus, the choice of the cervical esophagogastric anastomotic method—triangulating stapling (TS) versus circular stapling (CS)—is a critical decision for the surgeon.
Aim:
To compare the incidence of major adverse outcomes between TS and CS in patients with resectable thoracic esophageal cancer.
Methods:
For this meta-analysis, PubMed, Embase, Wiley Online Library, Google Scholar, Wanfang, and China National Knowledge Infrastructure databases were searched for subject-relevant studies by using a rigorous study protocol established according to the recommendations of the Cochrane Handbook. Anastomotic leakage, anastomotic stricture, and postoperative pulmonary complications were the primary endpoints used for comparison. Relative risk (RR) with 95% confidence intervals (CI) were calculated to assess the strength of association.
Results:
Six studies were selected by our inclusion/exclusion criteria and represented a total of 739 patients in our meta-analysis of TS (n = 376) versus CS (n = 363). The TS group showed a lower incidence of anastomotic stricture (RR: 0.23 [95% CI: 0.08–0.63]; P = .004) and pulmonary complications (RR: 0.57 [95% CI: 0.37–0.87]; P = .01). However, the incidence of anastomotic leakage was similar for the two groups (RR: 0.66 [95% CI: 0.41–1.09]; P = .1). Subgroup analysis of four studies in which the surgical methods were minimally invasive demonstrated the TS group to have a lower incidence of lung complications (RR: 0.55 [95% CI: 0.35–0.87]; P = .01), anastomotic leakage (RR: 0.36 [95% CI: 0.18–0.74]; P = .005), and anastomotic stricture (RR: 0.23 [95% CI: 0.05–0.98]; P = .05).
Conclusion:
The TS method for cervical esophagogastric anastomosis after esophagectomy had a lower incidence of anastomotic stricture and postoperative lung complications.
Introduction
Esophageal carcinoma is the eighth most common cancer and sixth most common cause of death worldwide. At present, extensive resection of the tumorous tissue followed by esophagogastric anastomosis is the standard treatment. 1 However, even cases of the treated disease continue to have poor prognosis and low quality of life due to the limitations associated with the surgery itself. Some of the major postsurgical complications are related to the anastomosis, the most prevalent being anastomotic stricture and leakage. 2 Thus, the choice of cervical esophagogastric anastomotic method—triangulating stapling (TS) versus circular stapling (CS)—is a critical decision for the surgeon, as one may produce a lower incidence of common complications.
Currently, use of a gastric tube for cervical reconstruction in esophagogastric anastomosis is widely accepted and the CS method is preferred by many for its convenience. In previous analyses, we found that CS can reduce the incidence of leakage but carries a high incidence of stricture, ranging from 40% to 50%.3,4 The stricture itself remains a prominent problem in these patients, as they are already suffering from dysphagia, malnutrition, and low quality of life.
The more recently introduced method of triangular anastomosis (TS), conducted by means of a linear stapler, has an advantage over CS by producing less suture failure and stenosis. 5 Many surgeons, especially those from China and Japan, have incorporated the TS method into their surgical practice of cervical esophagogastric anastomosis after esophagectomy in patients with thoracic esophageal cancer. Nevertheless, its effectiveness is still controversial.6,7 Therefore, the present meta-analysis was designed as the first to compare TS and CS cervical esophagogastric anastomotic methods for treatment of resectable esophageal cancer with regard to postsurgical complications. The results of our study will aid surgical decision making and design of effective and safe treatment strategies.
Materials and Methods
Data sources and search strategy
We carried out systematic searches of PubMed, Embase, Wiley Online Library, Google Scholar, Wanfang, and China National Knowledge Infrastructure databases by using the terms “triangulating stapling,” “circular stapling,” “esophagogastric anastomosis,” “triangular anastomosis,” “circular anastomosis,” and “esophagectomy” combined with the Boolean operators AND or OR (date until August 2019). References from articles identified at this step were checked for additional suitable studies, which were then obtained as well.
Selection of studies
Inclusion and exclusion criteria
Literature included in the present meta-analysis was required to meet the following criteria: (1) The study must have been a randomized controlled trial or a nonrandomized comparison trial with parallel controls, (2) the study must have carried out a comparison between triangular and circular anastomosis, and (3) the publication must provide sufficient data for calculating relative risk (RR)/odds ratio and a 95% confidence interval (CI). When there were multiple studies using the same population, only the most up-to-date research was included. Studies were excluded when the design was not a controlled study, if it was a case report, or if the study data were incomplete.
Data extraction
Two investigators (S.-Y.D. and X.-Y.H.), working independently, extracted the data, including, but not limited to, first author, country, publication year, numbers of cases, and outcomes. Doubled data were included. The Cochrane Collaboration's tool for assessing risk of bias was applied to each selected study, with the following seven yes/no/unclear queries: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective reporting, and (7) other bias.
Definition of outcomes
Anastomotic stricture
An endoscope with an ∼9-mm diameter could not pass or dilation was required.
Anastomotic leakage
Signs of clinical fistula and/or presence of extraluminal contrast by imaging examination.
Postoperative lung complications
Mainly including pneumonia, pneumothorax, and respiratory failure.
Statistical analysis
All extracted data were entered into Review Manager 5.1 software by 2 investigators (S.-Y.D. and X.-Y.H.) working in parallel. The RR was calculated by using 95% CIs. The χ 2 statistic was used to assess heterogeneity, and the Higgins I2 statistic was used to determine the percentage of total variations across studies caused by heterogeneity. If the I2 statistic was less than 50%, the fixed-effects model was used; otherwise, the random-effects model was used. Forest and funnel plots were used to estimate the heterogeneity and publication bias.
Results
Study characteristics
Six studies consisting of 739 total patients (376 who received TS and 363 who received CS) were included in our meta-analysis.6–11 Figure 1 presents the flow chart of our literature search, carried out according to the PRISMA statement. Patient clinical data from each study are presented in Table 1.
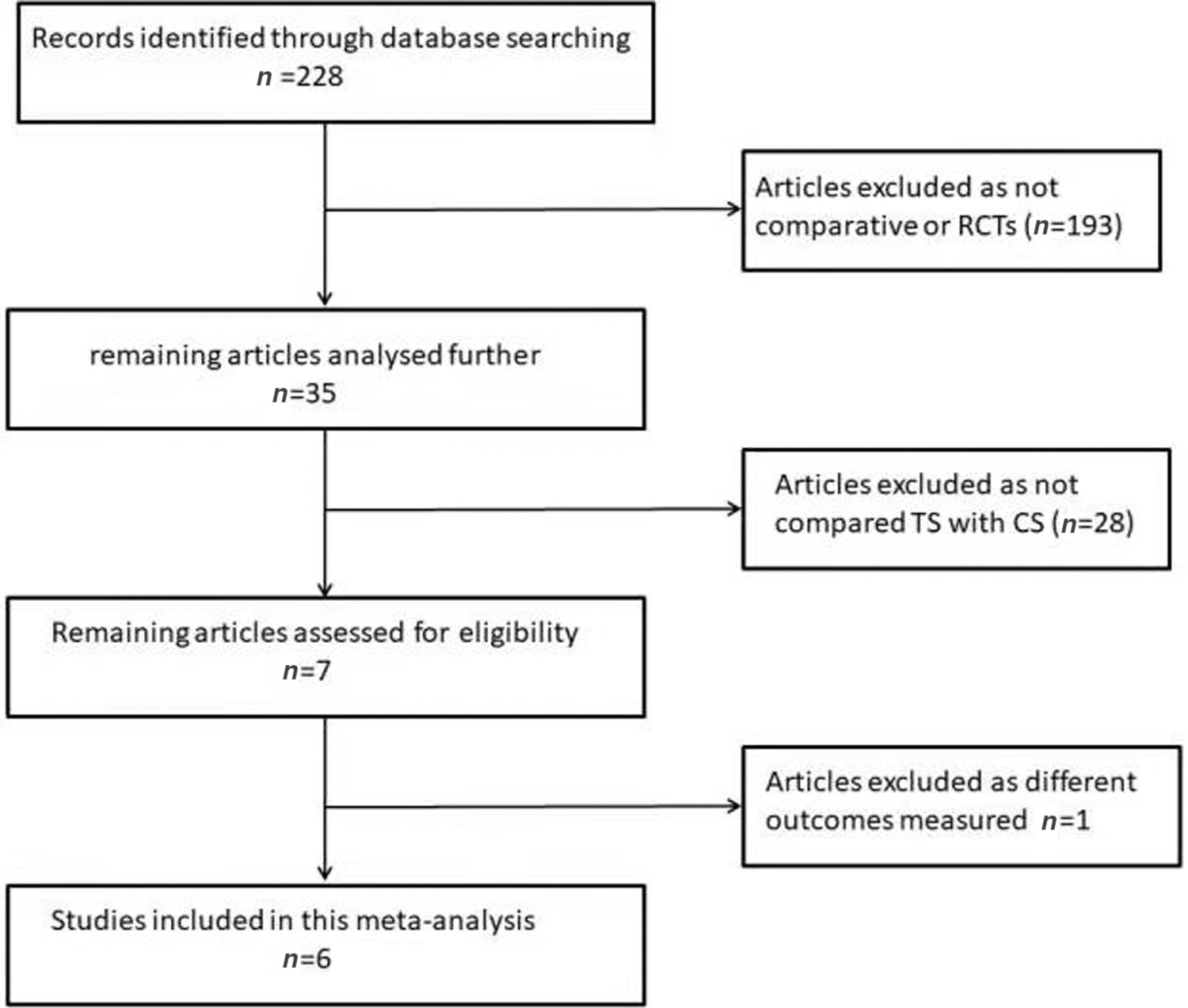
Flow chart of the literature search according to the PRISMA statement. CS, circular stapling; RCT, randomized controlled trial; TS, triangulating stapling.
Six Studies Included in This Meta-Analysis
Data are presented as average or average ± standard deviation.
CS, circular stapling; RCT, randomized controlled trial; TS, triangulating stapling.
Esophagogastric anastomotic stricture
All six studies investigated the incidence of anastomotic stricture after TS versus CS. The TS method showed less incidence of anastomotic stricture compared with the CS method (RR: 0.23 [95% CI: 0.08–0.63]; P = .004; Fig. 2A). For this analysis, statistical heterogeneity was found to be significant (I 2 = 60%, χ 2 = 12.52 [degrees of freedom, df = 5]; P = .03).
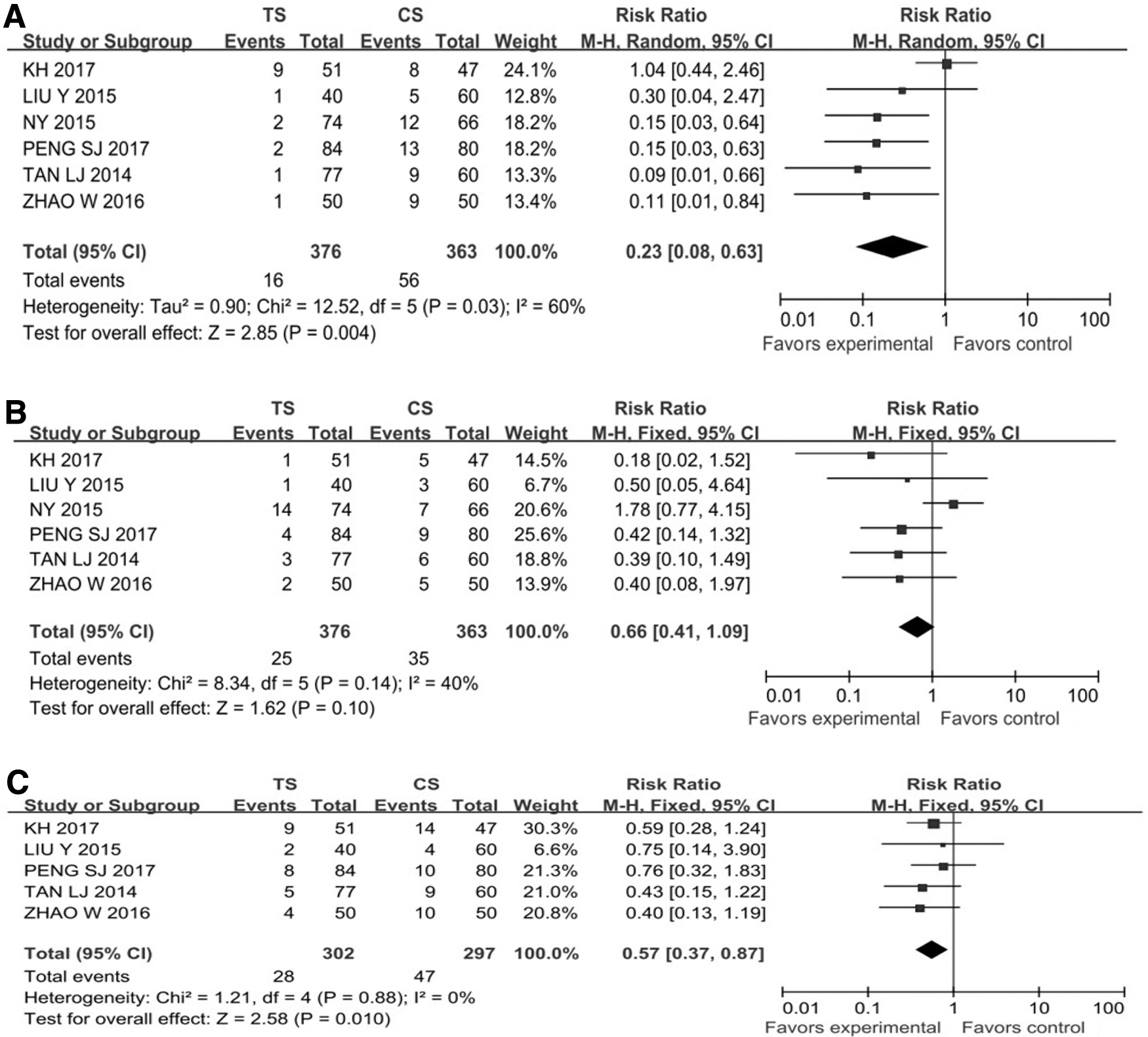
Forest plots to estimate the heterogeneity and publication bias for three outcomes of interest for TS and CS.
Esophagogastric anastomotic leakage
All six studies reported the incidence of anastomotic leakage after TS versus CS. The two groups showed a statistically similar incidence of anastomotic leakage (RR: 0.66 [95% CI: 0.41–1.09]; P = .1; Fig. 2B). For this analysis, mild heterogeneity was found (I 2 = 40%, χ 2 = 8.34 [df = 5], P = .14).
Postoperative lung complications
The postoperative morbidity rates of lung complications were 9.3% for the TS group and 15.8% for the CS group from the five studies that reported on them. The rate was significantly different between the two groups (RR: 0.57 [95% CI: 0.37–0.87]; P = .01), indicating that the application of TS may reduce the postoperative morbidity rates of lung complications (Fig. 2C). For this analysis, no statistical heterogeneity was found (I 2 = 0%, χ 2 = 1.21 [df = 4]; P = .88).
Subgroup analysis
We performed a subgroup analysis of studies in which the surgical methods were minimally invasive. The TS group showed a significantly lower incidence of lung complications (RR: 0.55 [95% CI: 0.35–0.87]; P = .01), anastomotic leakage (RR: 0.36 [95% CI: 0.18–0.74]; P = .005), and anastomotic stricture (RR: 0.23 [95% CI: 0.05–0.98]; P = .05) compared with the CS group (Fig. 3).
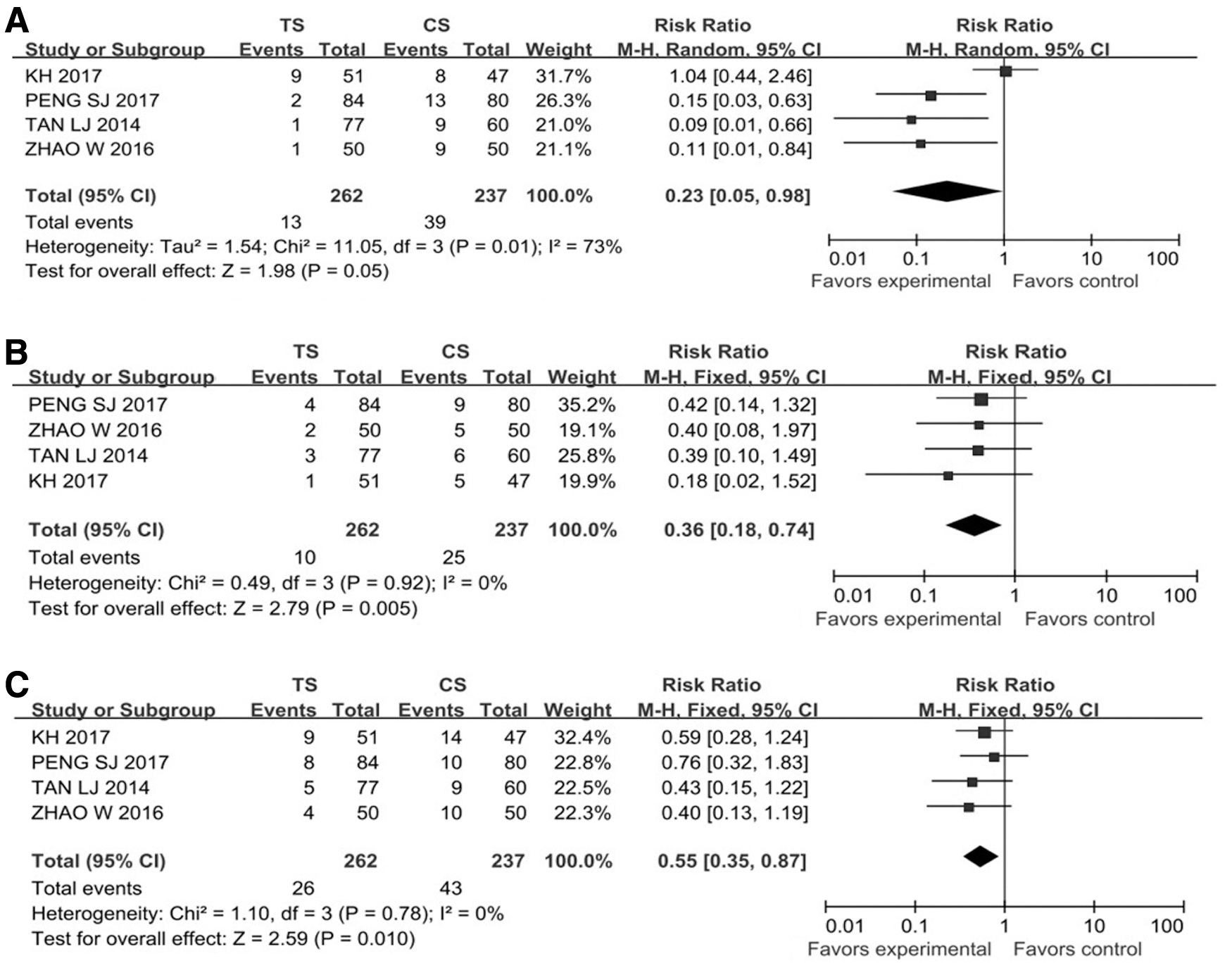
Forest plots to estimate the heterogeneity and publication bias for the three outcomes of interest for minimally invasive surgeries with TS or CS.
Sensitivity analysis and publication bias
We conducted a sensitivity analysis of the three main outcomes (anastomotic stricture, anastomotic leakage, and postoperative lung complications) by excluding any single study and re-testing the heterogeneity. For anastomotic stricture and leakage, the heterogeneity was found to come mainly from Hayata et al. 6 and Yoshida et al., 7 respectively. According to our funnel plot analysis, there was significant heterogeneity in the publications for anastomotic stricture and mild heterogeneity in those for anastomotic leakage (Fig. 4).
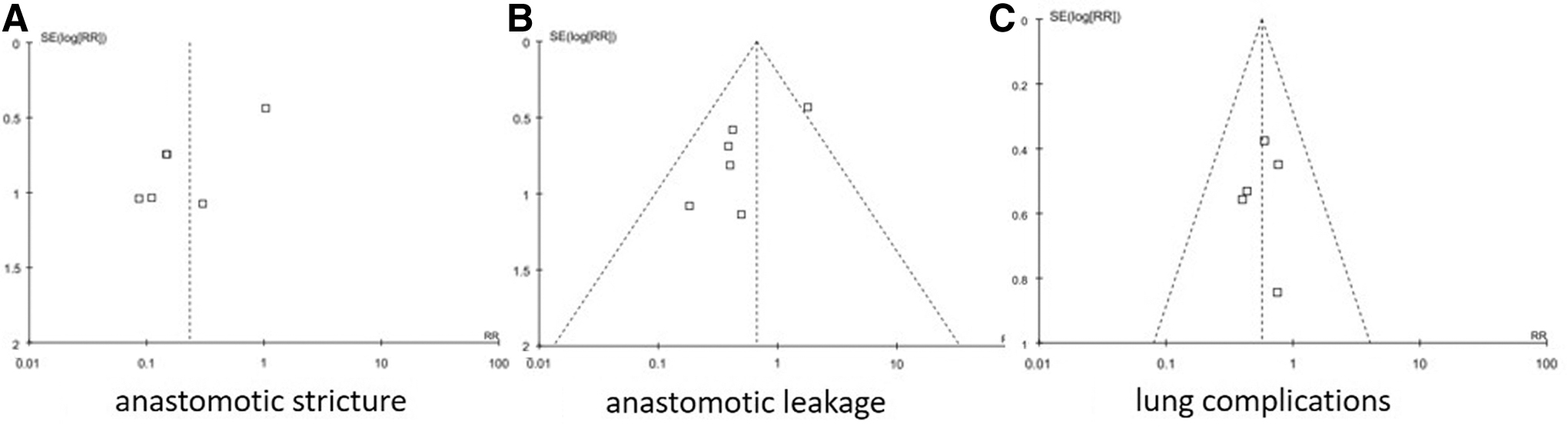
Funnel plots for the three outcomes.
Discussion
Gastroesophageal reconstruction remains a challenge to surgeons who follow the standard treatment of esophageal cancer (i.e., resection). Addressing the risk factors of the related anastomotic complications that plague this treatment will ultimately bolster patient postoperative quality of life. 12 The known factors are age, body weight, cardiovascular disease, pulmonary disease, chemoradiotherapy, and suturing technique; for suturing, the anastomotic technique is one of the most important concerns facing the esophageal surgeon.13–15
Triangular anastomosis was originally used for colon cancer surgery. 16 However, gratifying results have been achieved since Japanese scholars adapted it to esophageal cancer surgery. 5 The TS method is an end-to-end anastomosis using a linear stapler. The method involves first suturing the posterior wall of the residual esophagus and the gastric tube in an inverted fashion, followed by application of another two linear staples for the anterior wall of the anastomosis in an everted fashion.
The traditional CS method is an end-to-side anastomosis involving suturing of the residual esophagus and posterior wall of the gastric conduit. Compared with the hand-sewn method, CS greatly improves the stenosis rate and decreases the incidence of anastomotic fistula.17,18 Further, a study comparing CS with the linear stapling method for side-to-side esophagogastric anastomosis showed that the latter produces a lower incidence of stenosis. 19 An important limitation to this finding is the fact that linear stapling is only suitable for lower or junctional esophageal cancer, which allows for retainment of a sufficient length of esophageal and gastric stumps for reconstruction.
Our meta-analysis showed a significantly lower rate of anastomotic stricture and a lowered trend of anastomotic leakage in patients who received TS compared with those who received CS. There are at least four reasons for the beneficial effects of TS on stricture that are possible. First, end-to-end anastomosis can ensure maximal blood supply at both sides of the anastomosis, benefiting anastomotic healing. 20 Second, the TS method itself achieves an inverted posterior and everted anterior mucosal wall, maximizing mucosal contact, and thereby decreasing the incidence of stricture and leakage. Third, the triangle-shaped anastomosis is wider than the circular type, and the tension is also lower because the TS method does not need to involve as much of the stomach tissue. Fourth, in the narrow anatomical space of the neck, it is more convenient to suture by using a smaller linear stapling device.
It is noteworthy that the TS group in our meta-analysis showed a significantly lower rate of lung complications than the CS group. This is likely due to the TS method having a lower risk of aspiration caused by postoperative gastroesophageal reflux, which is also a common postoperative complication influenced by the anastomotic technique, among other factors. 21 Subgroup analysis of the four studies in our meta-analysis that investigated minimally invasive surgical techniques showed the TS group to have a significantly lower incidence of lung complications, anastomotic leakage, and anastomotic stricture compared with the CS group.
Our study is limited by the overall small sample size, not only in the number of trials but also in the number of patients. The fact that five out of the six studies included were not randomized controlled trials may raise the risk of bias. Moreover, there was significant heterogeneity in the anastomotic stricture analysis and mild heterogeneity in the anastomotic leakage analysis. On one hand, the study by Hayata et al. 6 employed a longer follow-up time (12 months instead of 1–4 months for the other studies). Since anastomotic stenosis after resection of esophageal cancer is a long-term complication, the length of follow-up will affect our accurate determination of its incidence. Because the majority of data for our included outcomes were obtained in short-term follow-up periods, we cannot say how close our findings reflect long-term incidences in this patient population. On the other hand, in the study by Yoshida et al., 7 the proportion of patients in the TS group who received preoperative chemotherapy or radiotherapy was much higher than that of patients in the CS group (67.6% versus 19.7% as reported). Preoperative radiotherapy and chemotherapy may increase the incidence of esophageal cancer anastomotic fistula; therefore, we recommend more prospective, multicenter, randomized controlled trials and long-term comprehensive follow-up.
In conclusion, this meta-analysis showed that application of the TS method for cervical esophagogastric anastomosis after esophagectomy produced a statistically significant smaller incidence of anastomotic stricture and lung complications as well as a lower rate of anastomotic leakage. Therefore, our meta-analysis suggests that the TS method could be an appropriate option for creating a cervical esophagogastric anastomosis in patients with thoracic esophageal cancer.
Footnotes
Acknowledgment
The authors gratefully acknowledge the contribution of S.-Y.D. in data extraction and software input.
Authors' Contributions
S.G.Z. designed the article; X.-Y.H. and S.-Y.D. collected the patient's clinical data; and S.G.Z. and X.-Y.H. analyzed the data and wrote the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from the Natural Science Foundation of China (No. 81201890) and Research Foundation of Education Bureau of Liaoning Province, China (No. LK201614).