
Abstract
Background and Objective:
Endocrine insufficiency must be considered following distal pancreatectomy (DP), because diabetes mellitus can impose a long-term burden on patients. This systematic review and meta-analysis aimed to identify the incidence and severity of new-onset diabetes mellitus (NODM) after DP for benign and malignant tumors, and other indications.
Methods:
Articles reporting NODM after DP from PubMed, Embase, Cochrane Library, and Google Scholar were analyzed. The quality of the studies was assessed using the Newcastle–Ottawa Scale or MOGA scale. Inverse variance analysis calculated the overall NODM incidence, and 95% confidence intervals (CIs) and P values were determined. Subgroup analyses considered pre-existing pancreatic diseases.
Results:
The quantitative analysis involved 18 articles that described 2356 patients with pancreatic neoplasms or inflammatory lesions. The overall incidence of NODM after DP was 29% (95% CI 25–33). The NODM rates were 23% (95% CI 17–30) and 38% (95% CI 30–45) for patients with pancreatic neoplasms and chronic pancreatitis, respectively. Pre-existing chronic pancreatitis and being male were risks associated with NODM.
Conclusion:
NODM is fairly common after DP. Surgeons and patients should be aware of postoperative treatment-dependent endocrine dysfunction. Larger cohort studies are required to clarify the risk factors for NODM after DP.
Introduction
Distal pancreatectomy (DP) is the standard procedure for removing benign and malignant neoplasms from the pancreatic body or tail. DP is also conducted on patients with chronic pancreatitis when the lesions are located at the distal pancreatic duct in the pancreatic body or tail. The development of imaging techniques and heightened public awareness about disease prevention have led to the discovery of increasing numbers of asymptomatic pancreatic lesions, particularly those in the pancreatic body or tail, many of which have low malignancy potentials (e.g., intraductal papillary mucinous neoplasm, mucinous cystic neoplasms, and pancreatic neuroendocrine tumors). Given the relatively benign nature of the lesions and their lower impact on gastrointestinal physiology, DP has a low mortality rate and is associated with a longer life expectancy. 1 However, the morbidity associated with DP is considerable. 2 Postoperative new-onset diabetes mellitus (NODM) or the worsening of preoperative diabetes is not uncommon after DP. DP was believed to carry a higher risk of endocrine insufficiency than central pancreatectomy. 3 According to De Bruijn and Van Eijck in their systemic review published in 2015, 4 the incidence of NODM after DP was estimated to be >10% among patients with pancreatic tumors and up to ∼40% among patients with chronic pancreatitis. However, as years have passed and concepts of procedures in DP have been changing in terms of function preservation, more evidence of higher quality is needed. As NODM can impose a huge burden on patients and their families, as well as on medical resources, it is important to identify the frequency and severity of NODM and to clarify the effects of diabetes on patients' quality of life and whole life spans.
This systematic review and meta-analysis aimed to determine the incidence and degree of NODM after DP for neoplasms and chronic pancreatitis and to tentatively examine the risk factors for NODM after DP.
Methods
The study protocol was registered in PROSPERO (CRD42019130425). The Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines 5 were followed.
Study selection
PubMed, Embase, and Cochrane Library databases and Google Scholar were extensively searched in June 2019. The PubMed database was searched using medical subject headings and the Embase database was searched using Emtree subject headings. The search terms used were as follows: “distal pancreatectomy,” “left pancreatectomy,” “diabetes mellitus,” “pancreas insufficiency,” and “endocrine dysfunction.” The publication language was restricted to English; there were no restrictions regarding the year of publication.
All publications that reported postoperative pancreatic endocrine function in patients who underwent DP via laparotomy or laparoscopy with or without splenectomy were included in the primary screening. Studies that (1) included early postoperative complications only and had a follow-up duration of <3 months, (2) did not describe the preoperative diabetes incidence, (3) focused on surgical techniques, or (4) focused on other specific interventions (e.g., islet autotransplantation) were excluded from the analysis.
Quality assessment
Quality assessments were performed to determine the strength and quality of the evidence generated by the studies. All cohort studies were assessed using the Newcastle–Ottawa scale (NOS) 6 ; an NOS score ≥6 points indicated a high-quality study. All case series were assessed using the MOGA scale 7 ; a MOGA score ≥12 points was considered acceptable.
Data extraction
Two of the investigators (J.Y. and R.S.) independently screened the titles, abstracts, and complete articles. The following data were extracted: the patients' sex, mean/median ages, and body mass indexes (BMIs); the presence of preoperative diabetes; the presence of postoperative diabetes; the types of pre-existing pancreatic disease present, namely, a benign lesion, a malignant tumor, or chronic pancreatitis; the type of DP, namely, spleen-preserving or involving a splenectomy; the criteria used to diagnose diabetes, including a patient's self-report, the fasting blood glucose (FBG) or glycated hemoglobin (HbA1c) level, or an oral glucose tolerance test (OGTT); the treatment required, including exercise and diet, oral medication, or insulin; and the follow-up time.
Statistical analyses
Data were analyzed using Stata/MP version 14.0 (Stata Corporation LLC, College Station, TX). When the NODM rate was not given in a publication, it was calculated from the original statistics reported in the publication using the number of patients with NODM divided by the number of patients without preoperative diabetes. Intention-to-treat analyses were used in all studies. The overall incidence of NODM was calculated using the inverse variance method. The I2 statistic was calculated to measure the heterogeneity among the studies; when the I2 value was ≤40%, a fixed-effects model was used; otherwise, a random-effects model was used. Subgroup analyses were conducted on the groups of patients with benign tumors, malignant tumors, and chronic pancreatitis. The patients' baseline characteristics were compared using Student's t-test for the continuous variables and the chi-squared test for the categorical variables. A two-sided value of P ≤ .05 was considered statistically significant. The confidence intervals (CIs) are presented at the 95% level. Forest plots were used to summarize the individual studies and overall results, and funnel plots were used to assess the risk-of-publication bias.
Results
Literature search
A total of 876 articles were identified from the PubMed, Embase, and Cochrane Library databases and Google Scholar. After removing the duplicate articles, 776 articles remained. Abstracts describing animal experiments, individual case histories, reviews, the mechanism of diabetes, specific tumor pathologies, surgical techniques, other postoperative complications, and other interventions were excluded. The complete text of 205 articles was assessed, and 158 of these articles were excluded, because they described duplicate trials, did not discriminate among different surgical subgroups, did not describe the long-term postoperative complications, or described surgical techniques. Of the remaining 47 articles, 15 were excluded, because either they did not describe the patients' preoperative diabetes status or the numbers of study participants were insufficient. While 32 studies were included in the systematic review, 14 were excluded from the meta-analysis, because the study quality or the numbers of patients with the study outcome were unsatisfactory. Finally, 18 studies that involved a total of 2356 patients who underwent DP were included in the quantitative synthesis (Fig. 1).
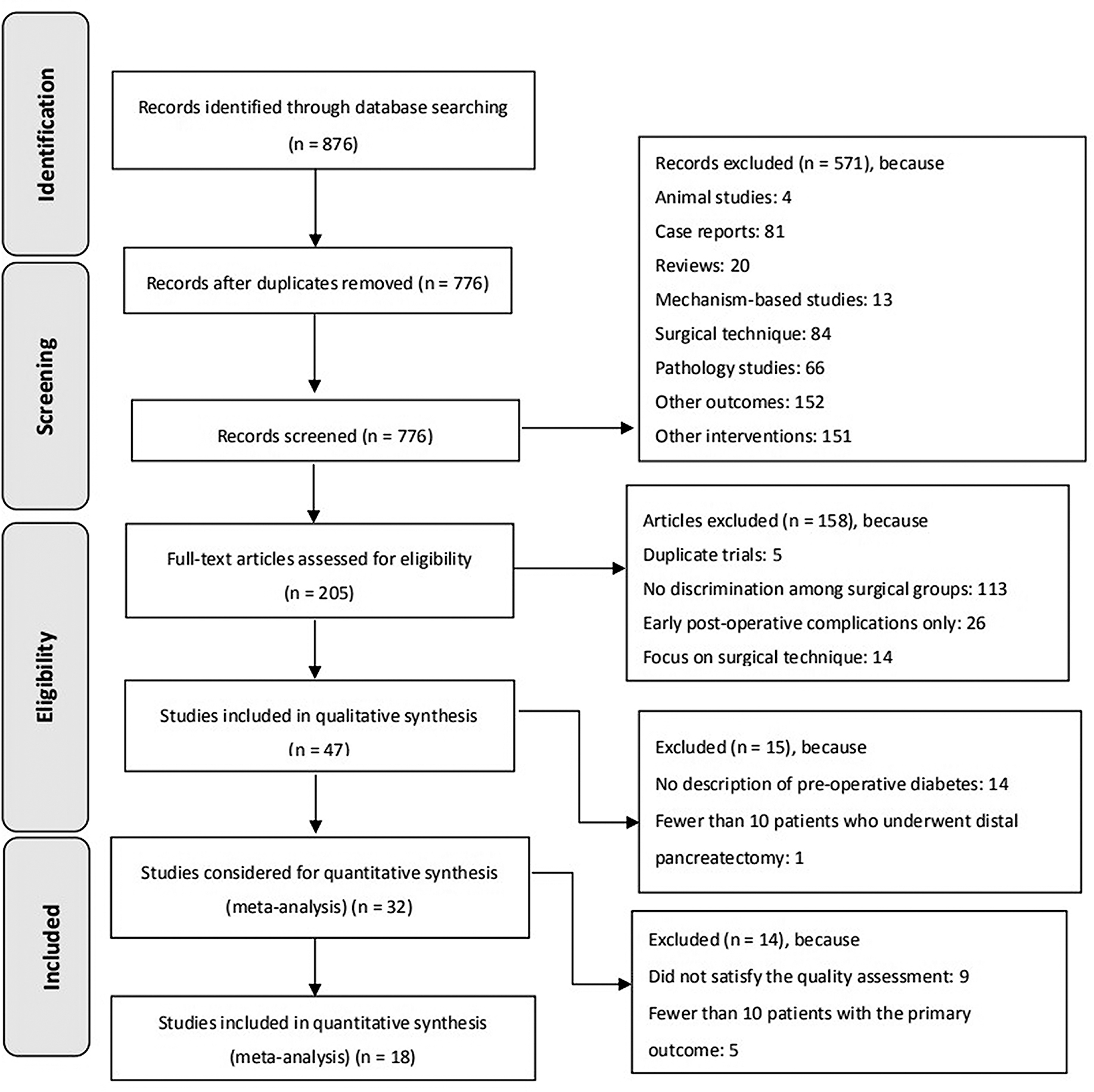
PRISMA flowchart of the studies selected for inclusion in the meta-analysis.
Study and patient characteristics
Table 1 summarizes the main characteristics of the studies and the patients included in the quantitative synthesis. A total of 2356 patients who had preoperative diagnoses of benign or malignant pancreatic neoplasms, chronic pancreatitis, or other pancreatic lesions were included in the quantitative synthesis. The mean ± standard deviation (SD) age of the patients was 51.6 ± 15.9 years, and the patients comprised 1139 males and 1217 females. Six studies involving 436 patients reported the mean ± SD BMI, which, for these patients, was 25.42 ± 7.70 kg/m2.
Endocrine Function After Distal Pancreatectomy: Summary of the Studies Included in the Meta-analysis
ADA, American Diabetes Association; BMI, body mass index; DM, diabetes mellitus; FBG, fasting blood glucose; HbA1c, glycated hemoglobin; NODM, new-onset diabetes mellitus; OGTT, oral glucose tolerance test; SD, standard deviation; WHO, World Health Organization.
The patients who underwent DP were divided into 3 subgroups according to the pre-existing pancreatic disease type. Subgroup 1 comprised 365 patients who had pancreatic neoplasms, Subgroup 2 consisted of 307 patients with chronic pancreatitis, and Subgroup 3 comprised 1684 patients who participated in studies that did not differentiate the pancreatic pathologies initially, thereby creating a heterogeneous group of patients with pancreatic neoplasms, chronic pancreatitis, or trauma. In terms of the patients' baseline characteristics, the differences between Subgroups 1 and 2 and Subgroups 2 and 3 in relation to the patients' mean ages were statistically significant (P < .001). No significant differences were evident between Subgroups 1 and 3 in relation to age or the BMI.
Meta-analysis of NODM
The meta-analysis involved 18 studies and 2356 patients whose preoperative endocrine function and postoperative pancreatic endocrine function were recorded in the publications. The I2 value was 64.0% (P < .001) for the 18 studies; consequently, a random-effects model was used to calculate the overall incidence of NODM, which was 29% (95% CI 25–33) for these patients, regardless of the presence of pre-existing pancreatic lesions (Fig. 2).
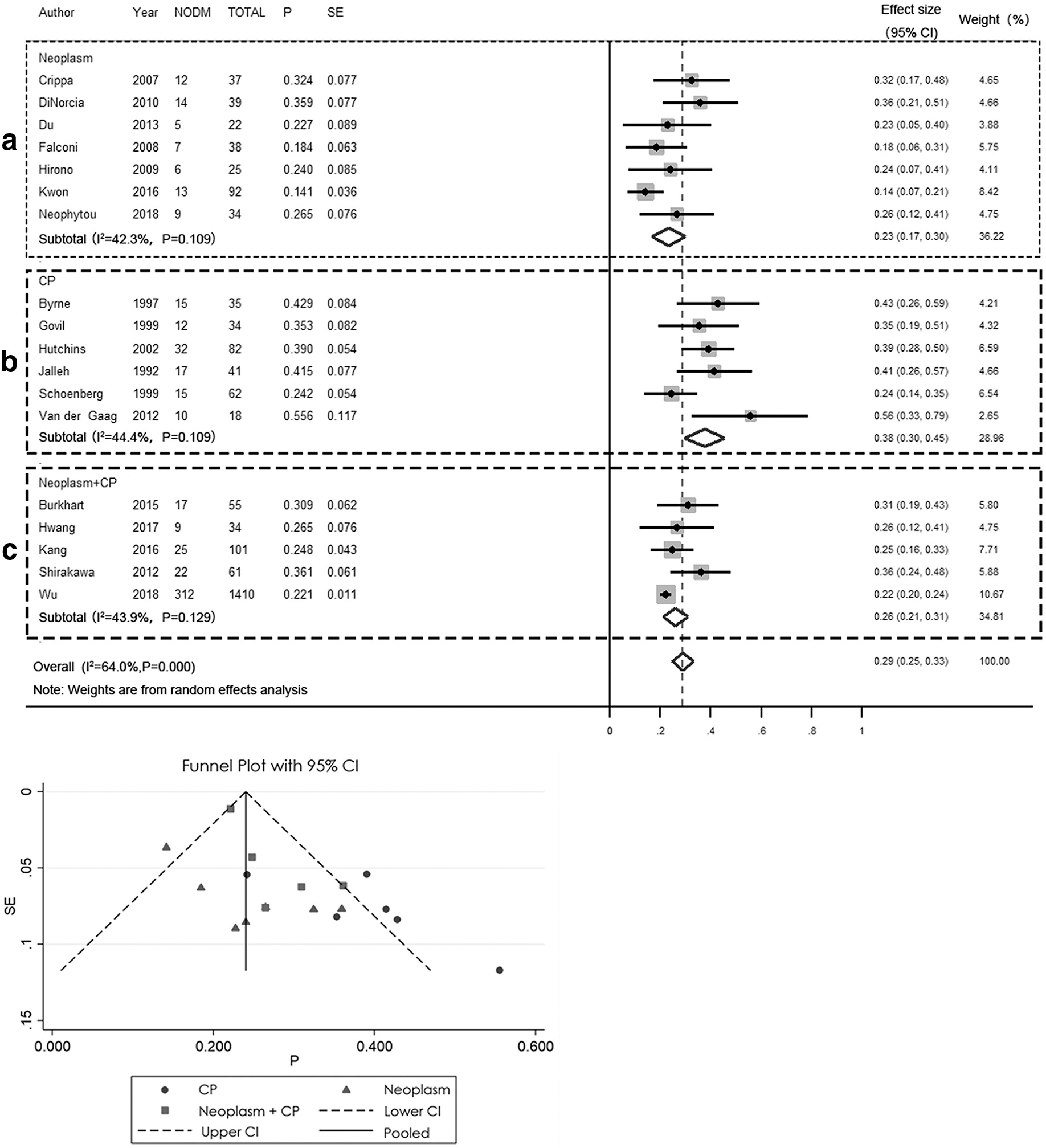
Incidence of NODM in the patients after distal pancreatectomy. P > 0.10 within each subgroup; P < 0.001 between
Since the heterogeneity among these studies was significant, we analyzed the studies in 3 subgroups according to the aforementioned types of pancreatic lesions reported.
Subgroup analyses
Subgroup 1: patients with pancreatic neoplasms
A total of 365 patients in 7 studies were included in Subgroup 18–14 for the quantitative synthesis of NODM after DP in patients with pancreatic neoplasms. The NODM incidence ranged from 13.6% to 35.9%. The mean ± SD age of the patients in Subgroup 1 was 54.09 ± 11.89 years, and Subgroup 1 comprised 115 males and 250 females. Only 3 studies reported the BMI, and the mean ± SD BMI of 196 patients was 24.18 ± 2.78 kg/m2. In this subgroup, 365 patients with pancreatic neoplasms underwent DP, of whom 326 (89.3%) were diagnosed with benign or borderline tumors and 39 (10.7%) were diagnosed with malignant tumors. Of the patients included in the quantitative synthesis, 60 (16.4%) were diagnosed with intraductal papillary mucinous tumors, 173 (47.4%) with cystic neoplasms, including serous cystic adenomas, serous pseudopapillary neoplasms, and mucinous cystic neoplasms, 52 (14.2%) with pancreatic neuroendocrine tumors, and 24 (6.6%) were diagnosed with other types of pancreatic lesions. The overall incidence of NODM was 23% (95% CI 17–30), the heterogeneity was moderate (I 2 = 42.3%; P = .109), and a random-effects model was used for the analysis (Fig. 2a). The aggravation of pre-existing diabetes was common after DP.
A variety of criteria were used to diagnose diabetes mellitus, including objective standards (e.g., the World Health Organization's criteria that are based on the FBG and HbA1c levels, and OGTT) and subjective reports (e.g., patients' medication requirements and diet control). Of note, preoperative diabetes mellitus was present in 16.8% of the patients in Subgroup 1; these patients were excluded from the analysis of the NODM rate.
The incidence of pancreatic fistula in Subgroup 1 ranged from 11% to 35%. All studies reported grade A–C postoperative pancreatic fistula cases based on the recommendations of the 2005 International Study Group on Pancreatic Fistula. 15
Subgroup 2: patients with chronic pancreatitis
Subgroup 216–21 consisted of 307 patients who underwent DP for chronic pancreatitis with unbearable complications. The mean ± SD age of the patients in Subgroup 2 was 44.64 ± 16.71 years, and Subgroup 2 consisted of 200 males and 107 females. None of the studies reported the patients' BMIs. The etiology of chronic pancreatitis was incompletely described within the reports. Thirty-five (11.4%) patients were diagnosed with diabetes mellitus before surgery; however, whether these patients experienced aggravations of their preoperative diabetes was not reported. The incidence of NODM ranged from 24.2% to 55.5% in Subgroup 2, and the overall NODM rate was 38% (95% CI 30–45). Heterogeneity within this subgroup was moderate (I 2 = 44.4%; P = .109), and a random-effects model was used for the analysis (Fig. 2b). After surgery, 44.3% of the patients became dependent on medication, including insulin.
Subgroup 3: patients with pancreatic neoplasms or pancreatitis
Subgroup 3 comprised a considerable number of studies22–26 that involved patients who underwent DP and whose pre-existing pancreatic diseases were not identified. This subgroup comprised 1684 patients with a mean ± SD age of 52.38 ± 16.20 years, and 49% of the patients were male. Three studies reported the patients' BMIs, and the mean ± SD BMI for 240 patients was 26.43 ± 9.96 kg/m2. Incidence of NODM ranged from 22.1% to 36.0% in this rather heterogeneous subgroup. The overall incidence of NODM was 26% (95% CI 21–31), and the I2 value was 43.9% (P = .129). In Subgroup 3, 6.73% of the patients had preoperative diabetes mellitus, and the overall postoperative incidence of diabetes was 21.25% (Fig. 2c).
Discussion
Among the patients in this meta-analysis who underwent DP, the overall incidence of NODM was 29%, irrespective of the type of pre-existing pancreatic lesion. The NODM rate was 23% among the patients with pancreatic neoplasms in Subgroup 1, which was significantly lower than that in Subgroup 2 (38%) that comprised patients who underwent DP for chronic pancreatitis. Overall, almost 30% of the patients who underwent DP might have experienced pancreatic endocrine function deficiencies, and this is a risk that cannot be overlooked. DP is performed with increasing frequency in clinical settings as consequences of progress in imaging techniques and the availability of more abundant resources for health care that facilitate the discovery and diagnosis of insidious pancreatic lesions, particularly those in the pancreatic body or tail.
When considering the emergence of diabetes mellitus and the insufficiency of pancreatic endocrine function, many more factors must be considered in addition to the pancreas. While the loss of insulin-producing beta cells through surgery is the fundamental cause of postoperative diabetes, sociodemographic, behavioral, and genetic factors also play important roles in diabetes.
Surprisingly, the patients with chronic pancreatitis in Subgroup 2 did not have a higher incidence of preoperative diabetes than those in the other subgroups. Nevertheless, they had a significantly higher incidence of postoperative diabetes, suggesting that the patients with chronic pancreatitis had reached the limits of their pancreatic functional reserve, contrary to that represented by the pancreatic function tests. The NODM rate was lower among the patients with pancreatic neoplasms because of the relatively higher volumes of functional pancreatic parenchymal tissue remaining after surgery. Whether different types of pancreatic lesion can influence the NODM incidence requires further investigation.
Subgroup 2 mainly comprised male patients, and the mean age of the patients in this subgroup was significantly lower than that of the patients in the other 2 subgroups. Hence, it was reasonable to consider that age and sex could be risk factors for NODM after DP. Patients' sociodemographic profiles and basic health indicators have been extensively investigated over the past few decades. Neophytou et al. 14 considered that a preoperative BMI >28 kg/m2 was a risk factor for the postoperative development of diabetes (hazard ratio [HR] 2.21; 95% CI 1.09–4.50; P = .0288) and that males had a greater risk for developing NODM (HR 1.43; 95% CI 1.22–1.87; P = .0191) than females; age, tobacco and alcohol usage, complications associated with hypertension, and liver dysfunction were not significantly associated with the postoperative development of NODM.
Concerning the surgical technique used, previous studies have investigated the impacts of the proportion of the pancreas resected and splenectomy on the incidence of NODM. Kwon et al. 13 reported that preserving the spleen during DP did not significantly impact upon the incidence of NODM. It is well established that saving more pancreatic parenchymal tissue during surgery preserves higher levels of the exocrine and endocrine functions. However, despite the importance of the relationship between the proportion of the pancreas resected and NODM, few studies have explored this topic thoroughly, because it is difficult to measure. Shirakawa et al. 25 found that a percent resected volume of the pancreas >44% was an independent risk factor for NODM (odds ratio [OR] 11.3; P = .004). While a standard DP procedure is preferred for removing malignancies from the pancreatic body or tail, the volume of pancreatic parenchymal tissue that should be resected during the removal of benign lesions remains debatable, especially for those in the pancreatic tail. For benign lesions in the pancreatic tail, a surgeon might have the option of dividing the pancreas at 2–3 cm proximal to the lesion to achieve a function-preserving DP. However, high-quality clinical research into the short-term and long-term complications and benefits of this modified approach is scarce; therefore, more clinical studies should be performed to validate this approach.
The incidence of NODM has been compared in relation to different types of pancreatic surgery. It was once believed that the rate of endocrine insufficiency would be higher after DP than after pancreatoduodenectomy, because functional beta cells are more prevalent near the pancreatic body and tail. 27 However, different clinical studies generated equivocal results. While some investigators considered that patients undergoing DP were at a higher risk of developing NODM (OR 2.222; P = .046) and some studies' findings showed a slightly higher incidence of NODM among patients who had undergone DP than among those who had undergone pancreatoduodenectomy, the difference was not significant. 28
Seven studies reported the incidence of postoperative infection; however, only one study by Hirono et al. 12 presented clear diagnostic criteria for postoperative infection: patients with positive culture, fever, and white blood cell count elevation. Other studies' description of infection was vague, only mentioning intra-abdominal abscess or other infections, including urinary tract infection, pneumonitis, subcutaneous infection, and catheter-related infection. Regarding pancreatic fistula, a relatively outdated definition and grading system was used, limiting its clinical significance in the current practice. Considering the limited report and nonstandardized reporting method, it was not clear whether perioperative complications, including pancreatic fistula and postoperative infection, would affect the development of endocrinal insufficiency. As these complications theoretically might influence patients' stress response and glucose regulation after surgery, it is important to incorporate a standard and up-to-date reporting system for postoperative complications in future studies to resolve this problem.
Time course of developing NODM has not been fully elucidated. In this review, studies with follow-up time less than 3 months were excluded, in consideration of possible insulin resistance under stress response in a short term after surgery. The mean follow-up time of included studies was 40 months. Several studies17–19 did report increased incidence of diabetes mellitus with time, suggesting a down-trending function of the remaining pancreatic parenchyma. Laboratory examinations, including insulin and C-peptide test, might be practical for more accurate and quantified clinical studies in the future to help us understand this.
This systematic review and meta-analysis involved a large number of patients and investigated the incidence of NODM after DP. The meta-analysis of the studies revealed NODM rates of 23% and 38% among the patients with pancreatic neoplasms and chronic pancreatitis, respectively. These findings were largely based on comprehensive information collected from 365 and 307 patients in Subgroups 1 and 2, respectively, and they were further supported by larger populations of patients that were included in the systematic review.
De Bruijn and Van Eijck provided a fundamental picture of NODM after DP in their 2015 review, 4 drawing attention to this clinically important issue. Five years later, we attempted to provide fresher clinical experience with our review of nine updated studies. The incidence of NODM in patients undergoing DP for pancreatic neoplasm was 23%, which was higher than the previous consideration (14%), 4 reinforcing the importance of this postoperative complication. We aimed to provide a clearer clinical picture of postoperative diabetes, describing the possible influencing factors, including pancreatic fistula and perioperative infections. Although we have seen the development of clinical guidelines and surgical techniques, there remain many problems with postoperative diabetes mellitus, and more high-quality clinical researches are required to elucidate this clinical concern.
The results from this meta-analysis should be interpreted in the context of its limitations. First, the criteria used to diagnose diabetes mellitus differed among the studies. Although some studies established the diagnoses using objective standards, including the FBG and HbA1c levels and the OGTT, a number of studies diagnosed diabetes based on patients' self-reports or their medication requirements, including insulin usage. Furthermore, other studies did not specify the criteria used to diagnose diabetes mellitus, and the investigators merely referred to previous medical records. Therefore, a bias may exist in relation to the postoperative diagnosis of diabetes, particularly among studies that used rigorous standards that may have led to underestimations of the NODM rates. Second, although all patients included in the meta-analysis underwent DP or left pancreatectomy, the volumes of the pancreas resected in routine clinical practice can greatly vary among institutions, surgeons, and patients. Given that the proportions of the pancreatic parenchymal tissue resected were not comprehensively recorded and discussed in each article, it was difficult to determine the effects of the volumes of the parenchymal tissue removed, which caused a high level of heterogeneity among the surgical approaches. Similar problems existed regarding other aspects of the surgery—for example, whether the surgery was performed via laparotomy or laparoscopy and whether or not the spleen was preserved in patients with different outcomes. With the quickly developing surgical approaches for the last 10 years, it would be beneficial if more recent clinical data could be reported for analyses. Third, the risk stratification of the pre-existing pancreatic diseases could not be fully elucidated, as well as bringing confounding factors, because it was based on the original designs of and reports from the included studies. Among the studies analyzed, most were retrospective case series, which meant that it was difficult to calculate the ORs and relative risks for each of the potentially associated factors.
Conclusion
This systematic review and meta-analysis should serve to remind surgeons that insufficiency of pancreatic endocrine function is a noteworthy long-term postoperative complication associated with DP. Pre-existing chronic pancreatitis, being male, and the volume of the pancreas resected might be risk factors for NODM. When informing patients of the surgical risks associated with DP, doctors should help patients understand that almost 1 in 4 patients is at risk for developing long-term diabetes, which may be medication- or, even, insulin-dependent. Given the patients' prognoses, surgeons should preserve as much of the pancreatic parenchymal tissue as possible. Cohort studies involving larger patient populations should be undertaken to clarify the risk factors associated with NODM after DP.
Footnotes
Acknowledgments
All data and analytic methods are available by e-mail request to the corresponding authors when required.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research is funded by the Fund for Excellent Youth in PUMCH (JQ201701).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.