
Abstract
Introduction:
Robotic distal gastrectomy (RDG) is now thought to be less invasive than conventional laparoscopic distal gastrectomy (LDG) for gastric cancer. Although the delta-shaped anastomosis is an established, widely performed procedure for intracorporeal Billroth-I (B-I) gastroduodenostomy after LDG, it has some difficulties and is performed in the ischemic region of the duodenum. We therefore developed a novel overlap B-I gastroduodenostomy after RDG.
Materials and Methods:
We started using the da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA) for RDG in May 2017. The robotic overlap B-I reconstruction was performed via side-to-side anastomosis, as follows: Two small incisions were made, one on the greater curvature of the remnant stomach, 5 cm from the edge of the remnant gastric stump, and one on the superior edge of the anterior wall of the duodenal stump. A 45-mm EndoWrist linear stapler device (EWLS) loaded with a blue cartridge was inserted through the incision. After the remnant stomach and duodenum were attached to the V-shaped form by the EWLS, the incisions were closed by the EWLS.
Results:
Seven patients underwent RDG followed by a robotic overlap B-I procedure up to March 2019. Short-term outcomes were determined from medical records and operative videos. No intraoperative complications or conversions to open or conventional laparoscopic surgery occurred. The mean time for the anastomosis was 37 (range 29–45 minutes) minutes. No postoperative complications occurred following the robotic overlap B-I procedure.
Discussion:
RDG followed by an overlap B-I gastroduodenostomy might be feasible and safe. However, long-term follow-up is required to identify additional benefits.
Introduction
Laparoscopic distal gastrectomy (LDG) for gastric cancer is an established minimally invasive procedure. Compared with open distal gastrectomy, it has several advantages, including less intraoperative blood loss, less postoperative pain, earlier postoperative recovery, and shorter hospital stay; and it provides an overall survival rate similar to the open approach.1–3 Robotic distal gastrectomy (RDG) is an emerging minimally invasive surgical option; and the technique has considerable short-term benefits, particularly with regard to reduction of local complications, including pancreatic fistula.4,5
The most common reconstruction methods performed after LDG is the Billroth-I (B-I) gastroduodenostomy. When the B-I is performed in totally LDG, the delta-shaped anastomosis (DSA), originally introduced by Kanaya et al. in 2002, 6 has been increasingly used, especially in Korea and Japan.6–8 Although the procedure for DSA is reportedly straightforward and has good long-term outcomes, this procedure involves several complicated procedures and pitfalls, such as a ventrodorsal direction for the duodenal transection, potential deterioration in the vascularization of the duodenum because of the need to create sufficient space around the duodenum, and difficulty in performing the common stub hole closure by endoscopic linear staples.9,10 Therefore, to overcome the difficulties of performing a DSA, we developed an overlap B-I procedure to perform after LDG, for which space around the posterior wall of the duodenum is no longer needed. 11 Although the technical aspects and outcomes of performing a DSA after RDG have been reported, 12 to the best of our knowledge, the overlap B-I procedure after RDG has never been reported.
Herein, we report our novel B-I procedure after RDG, which is performed using a 45-mm EndoWrist linear stapler (EWLS). 13
Materials and Methods
Patients
Starting in July 2017, robotic gastrectomy with B-I reconstruction was performed using an EWLS in 7 consecutive patients with gastric cancer at the Department of Gastrointestinal and Pediatric Surgery of Mie University Graduate School of Medicine. The diagnosis was based on preoperative examinations that included gastrointestinal endoscopy, an upper gastrointestinal series, and abdominal computed tomography. Tumor staging for each patient was based on the Japanese Classification of Gastric Carcinoma (15th edition). 14 In our institution, B-I reconstruction following RDG has been indicated for patients with clinical T1 or T2 gastric cancer in the lower or middle third of the stomach without duodenal invasion, and for whom at least one-third of the remnant stomach can be preserved.
Robotic distal gastrectomy
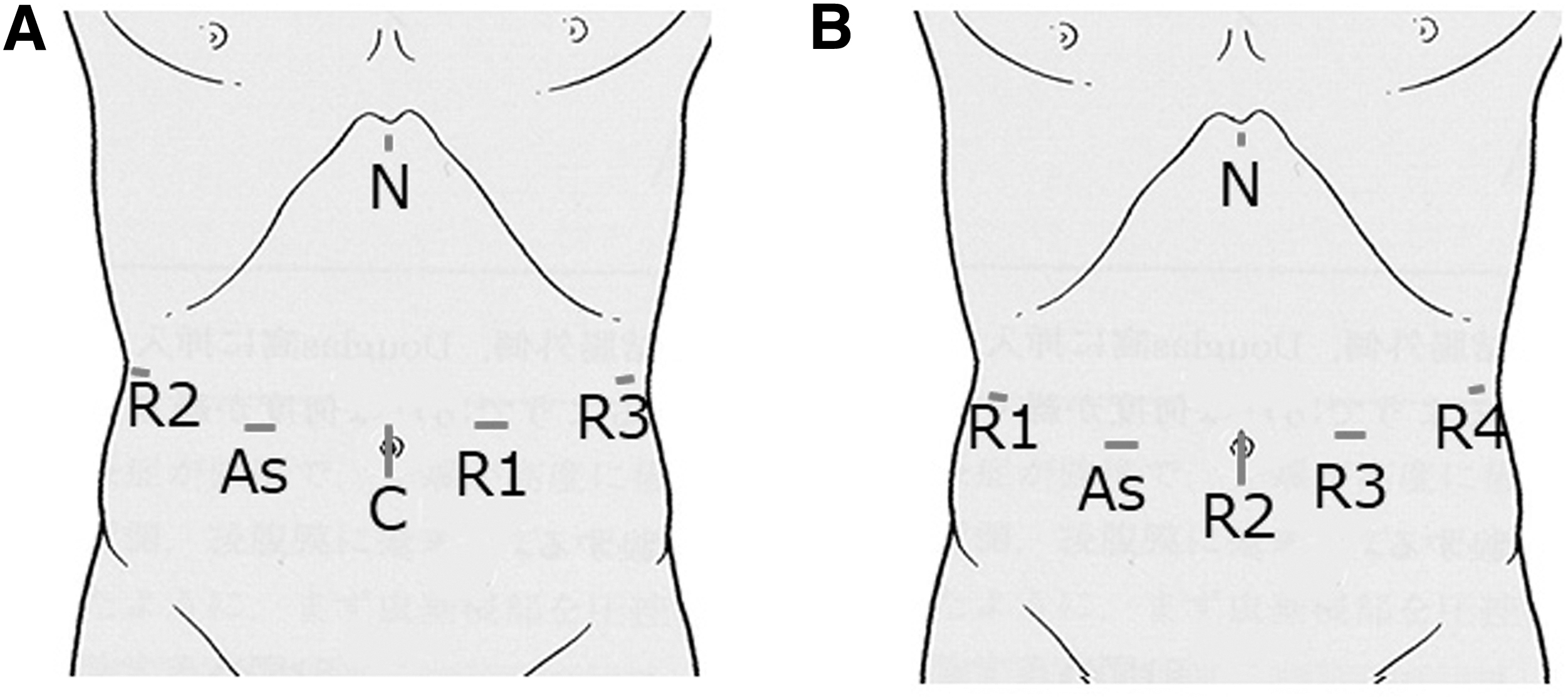
Each patient was placed in the supine position with the legs closed and a 15-degree head-up tilt. The details of the set up and procedures for RDG were previously reported. 15 We usually used the da Vinci Si or Xi Surgical System (Intuitive Surgical, Sunnyvale, CA) and a five-trocar system arranged on the upper abdomen. The correspondence of the trocars with the robotic arms differed between the Si setup and Xi setup, as shown in Figure 1A and B, respectively.
B-I procedure after RDG using the EWLS
The duodenal bulb was transected just below the pyloric ring from the posterior side toward the anterior side using EWLS after dissection of the infrapyloric lymph nodes (Supplementary Video S1 ). The B-I procedure was used as the primary option for alimentary tract reconstruction as long as the remnant stomach could be placed near the duodenal stump without excessive tension during the operation. When the B-I was infeasible because of too much tension between the remnant stomach and the duodenal stump, or presence of hiatal hernia, a Roux-en-Y anastomosis was performed.
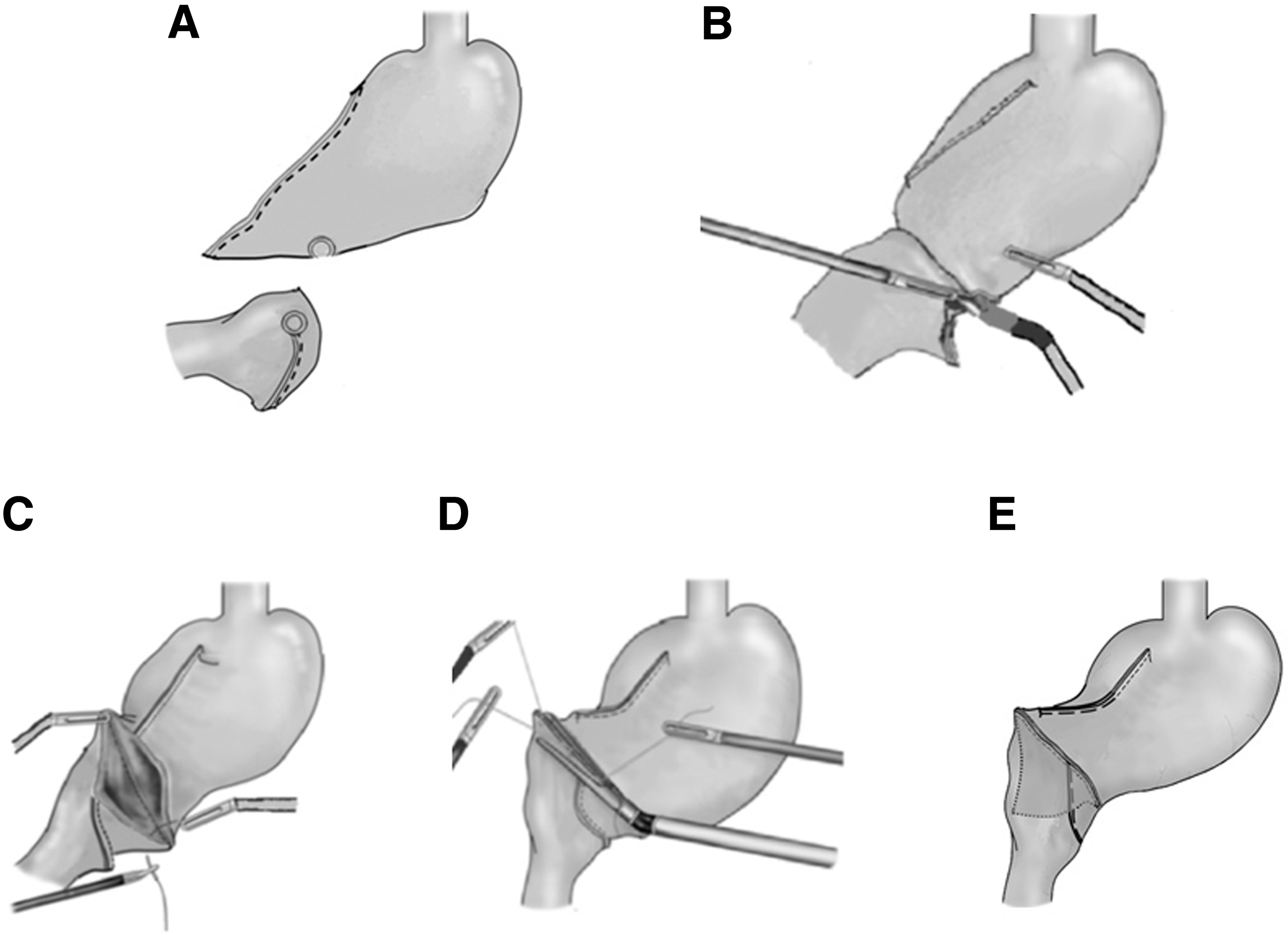
After the specimen was resected, small entry holes were made on the greater side 5 cm from the edge of the remnant gastric stump and at the superior edge of the anterior side of the duodenal stump (Fig. 2A). One suture was placed at each hole to prevent the mucosa and serosa from retracting. The EWLS was inserted through the left lower port. The forks were inserted into each created hole and were fired distally from each hole (Fig. 2B). The angulation and direction of the device could be freely adjusted with seven degrees of freedom and motion scaling. Thus, the remnant stomach and duodenum were attached in a V-shaped form at the base of the overlap B-I anastomosis (Fig. 2C). Finally, the common stab hole was closed with three stay sutures at the center and at both edges and was closed from the greater curvature side toward the lesser curvature side using the EWLS (Fig. 2D). By adjustment of the angulation and direction of the EWLS, uniform tension could be maintained and a wide-lumen stapled anastomosis could be formed (Fig. 2E).
(
Results
Patients' characteristics and surgical outcomes
Up until March 2019, 7 (2 males, 5 females) of 19 patients undergoing robotic gastrectomy underwent an RDG followed by robotic overlap B-I anastomosis. Patient characteristics and surgical outcomes are shown in Table 1. The mean patient age was 66 years (range, 52–78 years), and the mean body mass index was 23.8 kg/m2 (range, 21.7–28.8 kg/m2). All 7 patients were diagnosed with clinical T1 or T2 gastric cancer in the lower or middle-third of the stomach, without lymph node involvement. The mean total duration of surgery was 384 minutes (range, 324–470 minutes), and the mean duration of the anastomosis procedure was 37 minutes (range 29–48 minutes). The mean estimated blood loss was 47 g (range, 10–116 g). A mean number of 29 (range 19–51) lymph nodes were harvested. Histopathological types included differentiated adenocarcinoma (1 patient, 14%) and undifferentiated adenocarcinoma (6 patients, 86%). The pathological depths of tumor invasion included pT1 (6 patients, 86%) and pT2 (1 patient, 14%). None of the patients had histopathological evidence of lymph node metastasis. Intraoperative complications and cases of conversion to conventional laparoscopic or open surgery did not occur.
Patient and Surgical Characteristics (N = 7)
Postoperative examinations
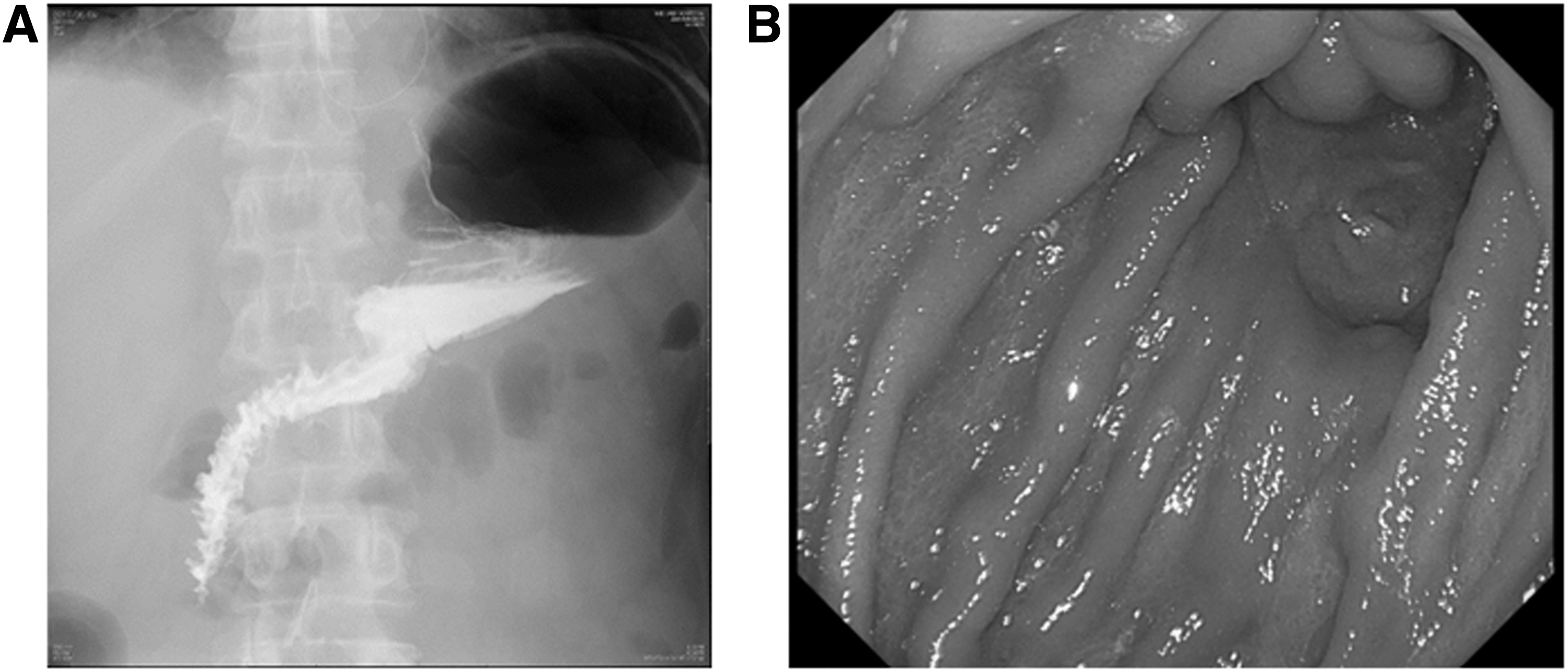
Figure 3A shows a contrast-enhanced radiographic image obtained 4 days after surgery. Passage of the contrast agent from the remnant stomach to the duodenum was very good, without leakage or stenosis. No postoperative complications, including anastomotic leakage, intraabdominal abscess, surgical site infection, remote infection, and delayed gastric emptying, were observed. The patients started drinking water on postoperative day 1 and started eating meals on postoperative day 4. The mean postoperative hospital stay was 12 days. Endoscopic examinations performed 6–12 months after surgery in 6 patients showed that the gastroscope had been smoothly inserted through the anastomosis (Fig. 3B). The median follow-up period was 22 months (range 10–31 months), and no late-phase complications, including stenosis, reflux, and dumping syndrome, were observed.
(
Discussion
Several procedures for intracorporeal B-I following LDG are known, including the DSA 6 and the modified triangulating stapling technique,16,17 which are essentially functional end-to-end anastomoses. The DSA requires further mobilization and rotation of the remnant stomach and duodenal stump. These actions might lead to deformation or torsion of the anastomosis, and insufficient rotation during anastomosis might leave ischemic tissue between the transection lines of the stumps and the anastomosis line, which might result in anastomotic complications. Although the modified triangulating stapling technique is an excellent method for preventing residual ischemic tissue, it also requires further mobilization of the duodenal stump to transect the entire line of the duodenal stump. Therefore, this might lead to further difficulties and enhanced complexity of this procedure.
Our novel overlap B-I procedure is characterized as a side-to-side overlap anastomosis between the greater curvature of the stomach and the anterior duodenal wall, with fixation using the EWLS. In this procedure, the vascular disposal of the duodenal posterior wall is unnecessary. Therefore, this reduces the possibility of damage to the surrounding structures and anastomotic ischemia. In addition, robotic surgery enables fine adjustment of the angulation and direction of the device because of 3-D magnified vision with high resolution, tremor filtering to prevent involuntary shaking of surgeons' hands, and seven degrees of freedom and motion scaling by the EWLS. 5 As a result, uniform tension and a wide anastomosis can be created, because angulation and direction of the EWLS are performed safely and easily, as needed by the surgeon. Furthermore, we believe that our procedure, which is essentially a side-to-side anastomosis, should result in decreased rates of anastomotic leakage and stenosis for the reason of absence of ischemic area in the anastomosis.
Considering that the entry hole on the side of the greater curvature must be located 5 cm from the stapler line, the remnant stomach for this anastomosis should probably be slightly longer on the side of the greater curvature than it would be with another anastomotic B-I method. However, this procedure is adopted for most cases with one-third remnant stomach. Besides, the Roux-en-Y reconstruction, an already established and widely accepted procedure, 18 can be adopted when the remnant stomach is small and the anastomosis is under too much tension on the greater curvature side. Rather, this procedure can be one of option for the case that a lot of stomach wall on the lesser curvature side was sacrificed.
We did not see any major complications during this study. However, there are study limitations, in that we only demonstrated a novel operative method of reconstruction following RDG on a small number of cases without sufficient follow-up time. Therefore, additional detailed clinical studies, including randomized control trials, are needed to validate the efficacy, safety, and benefits of this procedure.
In conclusion, our robotic procedure using the EWLS consists of a relatively simple and safe mechanical gastroduodenostomy, which results in reduced operative time. We suggest that this novel operation could be a feasible surgical procedure for RDG.
Ethical Statement
All procedures and subsequent analyses were performed with the approval of the Institutional Review Boards of Mie University Hospital in Japan (No. 2017–3203). The study was conducted in accordance with the guidelines of the 1975 Declaration of Helsinki.
Disclaimer
Written informed consent was obtained from all study participants.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.