
Abstract
Background:
Laparoscopic cholecystectomy is the main treatment of acute cholecystitis. Although considered relatively safe, it carries 6%–9% risk of major complications and 0.1%–1% risk of mortality. There is no consensus regarding the evaluation of the preoperative risks, and the management of patients with acute cholecystitis is usually guided by surgeon's personal preferences. We assessed the best method to identify patients with acute cholecystitis who are at high risk of complications and mortality.
Methods:
We performed a systematic review of studies that reported the preoperative prediction of outcomes in people with acute cholecystitis. We searched the Cochrane Library, MEDLINE, EMBASE, WHO ICTRP, ClinicalTrials.gov, and Science Citation Index Expanded until April 27, 2019. We performed a meta-analysis when possible.
Results:
Six thousand eight hundred twenty-seven people were included in one or more analyses in 12 studies. Tokyo guidelines 2013 (TG13) predicted mortality (two studies; Grade 3 versus Grade 1: odds ratio [OR] 5.08, 95% confidence interval [CI] 2.79–9.26). Gender predicted conversion to open cholecystectomy (two studies; OR 1.59, 95% CI 1.06–2.39). None of the factors reported in at least two studies had significant predictive ability of major or minor complications.
Conclusion:
There is significant uncertainty in the ability of prognostic factors and risk prediction models in predicting outcomes in people with acute calculous cholecystitis. Based on studies of high risk of bias, TG13 Grade 3 severity may be associated with greater mortality than Grade 1. Early referral of such patients to high-volume specialist centers should be considered. Further well-designed prospective studies are necessary.
Introduction
Acute cholecystitis is an acute inflammatory disease of the gallbladder. In the United States, there were about 213,000 hospital admissions related to acute cholecystitis in 2012. 1 The costs related to the management of these patients were about U.S. $43,000 per patient. 1 Acute cholecystitis costs U.S. $9.3 billion annually, accounting for 1.5% of total health care costs in the United States. 1 Approximately 85% of acute cholecystitis is due to gallstones. 2 Approximately 0.3%–0.4% of people with gallstones develop acute cholecystitis annually. 3
Laparoscopic cholecystectomy during the index admission is generally recommended in people with acute calculous cholecystitis, if they are fit to undergo surgery.3,4 However, laparoscopic cholecystectomy is a major surgical procedure and, although considered relatively safe, it is associated with about 0.1%–1% mortality rate,5–7 ∼0.2%–1.5% risk of bile duct injury,6–8 and about 6%–9% risk of major complications, such as myocardial infarction, heart failure, acute stroke, renal failure, pulmonary embolism, lung failure, or postoperative shock. 5
Conservative management with fluids, analgesia, and antibiotics is an alternative option for people with mildly symptomatic acute cholecystitis (i.e., in people without peritonitis or those who have worsening clinical condition). In a small randomized-controlled trial (RCT) with high risk of bias including 64 participants, about 30% of people treated conservatively (33 participants) developed recurrent gallstone-related complications over a median follow-up of 14 years, and 60% of people had undergone cholecystectomy subsequently.9,10 Furthermore, the mean age of the participants in the trial of surgery versus conservative management in mildly symptomatic acute cholecystitis was about 55 years and the study excluded patients older than 80 years or those with severe comorbidities. 10 Therefore, the trial does not address the issue of whether surgery or conservative treatment is better in elderly people or those with severe comorbidities. Therefore, until new high-quality evidence becomes available, laparoscopic cholecystectomy can be considered the recommended treatment for people who are fit to undergo surgery.
Identification of patients with acute cholecystitis at high risk of complications and mortality can help in optimizing these patients before surgery or referral to high-volume specialist centers, which may decrease the complications.11,12 This can also help in making informed decisions about surgery versus conservative management. However, there is no current consensus on how to measure the operative risk. 4
There are currently no systematic reviews of prognostic factors or risk prediction models in patients with acute calculous cholecystitis and the management of those patients is usually not evidence based.
The aim of our study is to assess the best method to predict the risk of death, complications, health-related quality of life, and conversion to open cholecystectomy in patients with acute cholecystitis, regardless of whether they underwent cholecystectomy.
Materials and Methods
The protocol was registered with PROSPERO database registration number: CRD42019136890. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidance was followed.13,14
Criteria for considering studies for this review
Types of studies
We included prospective and retrospective studies that reported the prediction of outcomes in people with acute cholecystitis. There were no restrictions by publication status or language. We excluded studies in which the people received different treatments based on the prognostic characteristics or those that compared different treatments or timing of treatments.
Types of participants
We included studies where all participants had acute calculous cholecystitis or if prognostic information was available separately for participants who had acute calculous cholecystitis.
Type of interventions and outcomes
We included only studies in which any patient-related or disease-related prognostic factors or risk prediction models could be applied preoperatively to predict the short-term mortality, adverse events, conversion to open surgery (in people who underwent surgery), and health-related quality of life using a validated scale. For adverse events, we accepted the adverse events as defined by the authors and considered them serious if they caused deaths, or were life-threatening, required inpatient hospitalization, resulted in a persistent or significant disability, or any important medical event that might have jeopardized the patient or required intervention to prevent it. 15 We also accepted Grade III or above in the Clavien–Dindo complication classification system as serious adverse events.16,17
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library, MEDLINE, EMBASE, WHO ICTRP, ClinicalTrials.gov, and Science Citation Index Expanded (including Conference Proceedings Citation Index) until April 27, 2019. We used the McMaster Health Information Research Unit search filters for MEDLINE and EMBASE databases.18,19 The detailed search strategy for each database is available in Supplementary Table S1.
Searching other resources
We also searched the references of the identified studies to identify further relevant studies.
Data collection and analysis
Two authors independently identified studies and extracted data from included studies in a prepiloted data extraction form created using Microsoft Excel.
Selection of studies
We identified the studies for inclusion by screening the titles and abstracts of the studies retrieved during the searches and retrieved the full texts of any articles identified by at least one of the review authors as being potentially eligible for inclusion. We selected studies for inclusion based on the assessment of the full-text articles (after translation, if required) and resolved any discrepancies arising regarding inclusion/exclusion through discussion.
Data extraction and management
Two authors independently extracted the following data.
Year and language of publication.
Country in which the participants were recruited.
Details of the settings such as primary care, secondary care, or tertiary care.
Year(s) in which the trial was conducted.
Inclusion and exclusion criteria.
Population characteristics such as age, sex, severity of acute cholecystitis.
Outcomes (mentioned in ‘Type of interventions and outcomes’).
Risk of bias (described below).
Details of the prognostic factor(s) or risk prediction model(s) (including the threshold, the details of the variables included in the risk prediction model, and whether this was a development study or a validation study: if the same study reported a development cohort and validation cohort, we considered these as two different cohorts).
We sought clarification of any unclear or missing information by contacting the authors of the individual trials. We resolved any differences in opinion through discussion.
Assessment of risk of bias in included studies
We independently assessed the risk of bias in the trials without masking the trial names. We used the prediction model risk of bias assessment tool (PROBAST) to assess the risk of bias. 20 The PROBAST tool has been mainly developed for risk prediction model. It includes the most relevant items from the quality in prognostic studies tool (developed for prognostic factor studies). 21 The schema that we used to assess the risk of bias is available in Supplementary Appendix SA1. We considered studies to have a low risk of bias if we assessed all the risk of bias domains as being at low risk of bias. In all other cases, the studies were considered to have unclear or high risk of bias.
Data synthesis
We calculated the summary C-statistic with 95% confidence interval (CI) along with odds ratio (OR) and its 95% CI and planned to calculate the summary observed versus expected events ratio with 95% CI and prediction intervals to determine the ability of each scoring system to predict the outcomes. However, none of the studies reported observed versus expected events; therefore, we performed only the meta-analyses of C-statistic and OR. We performed a meta-analysis only when this was meaningful (e.g., we combined only studies with identical thresholds used to define high and low levels of the prognostic score) using Stata 15. For meta-analysis of the C-statistic, we used the logit transformation; for OR, we used log transformation. We used the random-effects model as default because of anticipated clinical heterogeneity among studies. We did not compare different thresholds of a specific prognostic scoring system against one another as planned because of the sparse data and the high risk of bias in the studies.
Subgroup analysis
We did not perform the planned subgroup analyses on elderly versus young patients because of the sparse data.
Reporting bias
We did not perform the planned exploration of reporting bias by funnel plots because of the few studies included for each prognostic factor or prognostic model. In some of the studies, the outcomes such as mortality and complications were not reported, although it is likely that they were measured. This indicates that there is possibility of reporting biases.
Results
Results of the search
We identified a total of 4697 references through electronic searches of The Cochrane Hepato-Biliary Group Controlled Trials Register and the Cochrane CENTRAL in The Cochrane Library (n = 72), MEDLINE (n = 595), EMBASE (n = 3269), and Science Citation Index Expanded (n = 740), ClinicalTrials.gov (n = 14), and WHO trial register (n = 7). We excluded 500 duplicates and 4167 clearly irrelevant references through reading abstracts. The remaining 30 references were retrieved as full text for further assessment. No references were identified through scanning reference lists of the identified studies. We excluded 18 references for the reasons listed under the “Characteristics of excluded studies.” In total, 12 studies fulfilled the inclusion criteria and provided data for the systematic review. The reference flow is shown in Figure 1.
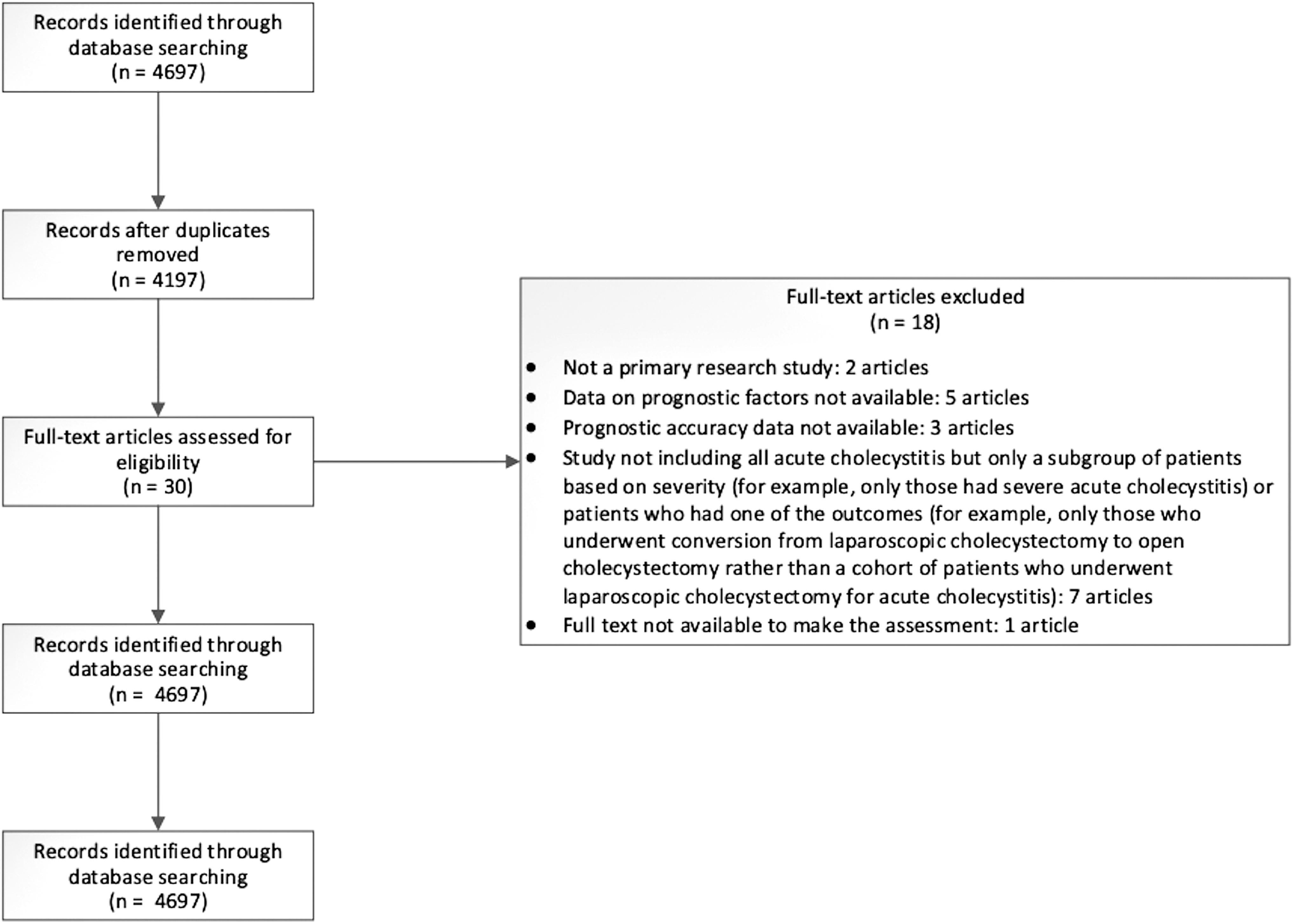
Study flow diagram. The figure shows the reference flow.
Characteristics of included studies
Of the 12 included studies, only 1 study was a prospective study 22 ; 9 studies were retrospective studies23–31 ; it was not clear whether the remaining 2 studies were prospective or retrospective studies.32,33
A total of 7978 people were eligible for this review in the 12 studies and 6827 people were included in one or more analyses in the 12 studies.22–33 A total of 1151 participants (14.4%) were excluded from the analysis by the authors due to missing data or because they did not undergo surgery. Eleven studies included only patients who underwent cholecystectomy.22–30,32,33 In the remaining study, 76.3% of people underwent cholecystectomy and the remaining patients were treated conservatively. Seven studies included only people who underwent laparoscopic cholecystectomy.22,23,25,29,30,32,33 In the remaining five studies, cholecystectomy was started as open procedure in 4.4%–45.9% of patients.24,26–28,31 The proportion of people who required conversion from laparoscopic to open procedure was 5.4%–23.8% in the 11 studies that reported this information.22–26,28–33 In seven studies, the cholecystectomy was performed early22,23,27,28,30,32,33; in two studies, the timing of cholecystectomy was not stated.26,31 The timing of surgery in the remaining 3 studies is as follows: in one study, 240 participants (89%) had early surgery 24 ; in a second study, 41 participants (77.4%) had surgery within 72 hours of admission 29 ; and in the last study, the median time to cholecystectomy was 7 days. 25
Eleven studies included adults of different age groups,22–26,28–33 while 1 study included only elderly patients (>65 years). 27 All studies included patients with and without comorbidities. It was difficult to estimate the proportion of patients with comorbidities in the studies as the comorbidities were defined in different ways in different studies.
The prognostic factors studied included individual prognostic factors such as age, gender, presence of diabetes, previous abdominal surgery, existing risk prediction scores such as The American Society of Anesthesiologists (ASA), Charlson Comorbidity Index, P-Possum, and Frailty index, and new predictive models based on regression, discriminant analysis, and artificial neural network.
The outcomes reported in the studies included all-cause mortality, major complications, minor complications, all complications, and conversion to open cholecystectomy. All the outcomes were reported until discharge or until 30 days of surgery. None of the studies reported predictors of health-related quality of life.
The characteristics of included studies are summarized in Supplementary Table S2. The prognostic factors or predictive models and the outcomes reported in each study are summarized in Table 1.
Prognostic Factors or Risk Prediction Models and Outcomes in Included Studies
ALT, alanine transaminase; ASA, The American Society of Anesthesiologists; AST, aspartate transaminase; BMI, body mass index; CRP, C-reactive protein; SAPS-II, Simplified Acute Physiology Score II; TG13, Tokyo Guidelines 2013; WBC, white blood count.
Characteristics of excluded studies
Eighteen studies were excluded for the following reasons: not a primary research study,34,35 data on prognostic factors not available,36–40 prognostic accuracy data not available,41–43 study not including all acute cholecystitis but only a subgroup of patients based on severity (e.g., only those had severe acute cholecystitis) or patients who had one of the outcomes (e.g., only those who underwent conversion from laparoscopic cholecystectomy to open cholecystectomy rather than a cohort of patients who underwent laparoscopic cholecystectomy for acute cholecystitis),44–50 and full text not available to make a sufficient assessment. 51
Risk of bias and applicability concerns
The risk of bias and applicability concerns in the studies are summarized in Supplementary Table S3. All the studies were at high risk of bias for one or more domains. The major reasons were that most studies were retrospective studies, the predictor or outcome measurements were not defined clearly for most predictors and outcomes, and blinding of predictor or outcome measurement was not reported. The number of participants with outcomes was <100 or the threshold was determined by optimal threshold for all the outcomes.
There were no concerns about whether the included participants were different from the usual type of patients with acute cholecystitis. However, it was not clear whether predictors or outcomes were measured in the same way as they would be measured in clinical practice, for example, it was not clear whether the predictors were measured on arrival or just after admission into the hospital or the complications included all the complications that would be routinely measured in clinical practice.
Discrimination results
A summary of the results from each study is presented in Supplementary Tables S4 and S5. The OR and the 95% CI are presented as forest plots in Figures 2–4 when there were at least two studies reporting the prognostic factor or predictive model, and in Supplementary Figures S1, S2, S3, S4 for other factors or predictive models with only one study.

Ordinal predictors. Meta-analysis showing the odds ratio and 95% confidence intervals for ordinal prognostic factors with at least two studies reporting the outcome. TG13 grading was the only ordinal prognostic factor that had at least two studies. TG13 Grade 3 increased the risk of all-cause mortality compared with Grade 1. There was no evidence of significant discriminatory ability for TG13 Grade 2 versus Grade 1 for either all-cause mortality or conversion to open cholecystectomy or for TG13 Grade 2 versus Grade 1 for all-cause mortality. TG13, Tokyo Guidelines 2013.
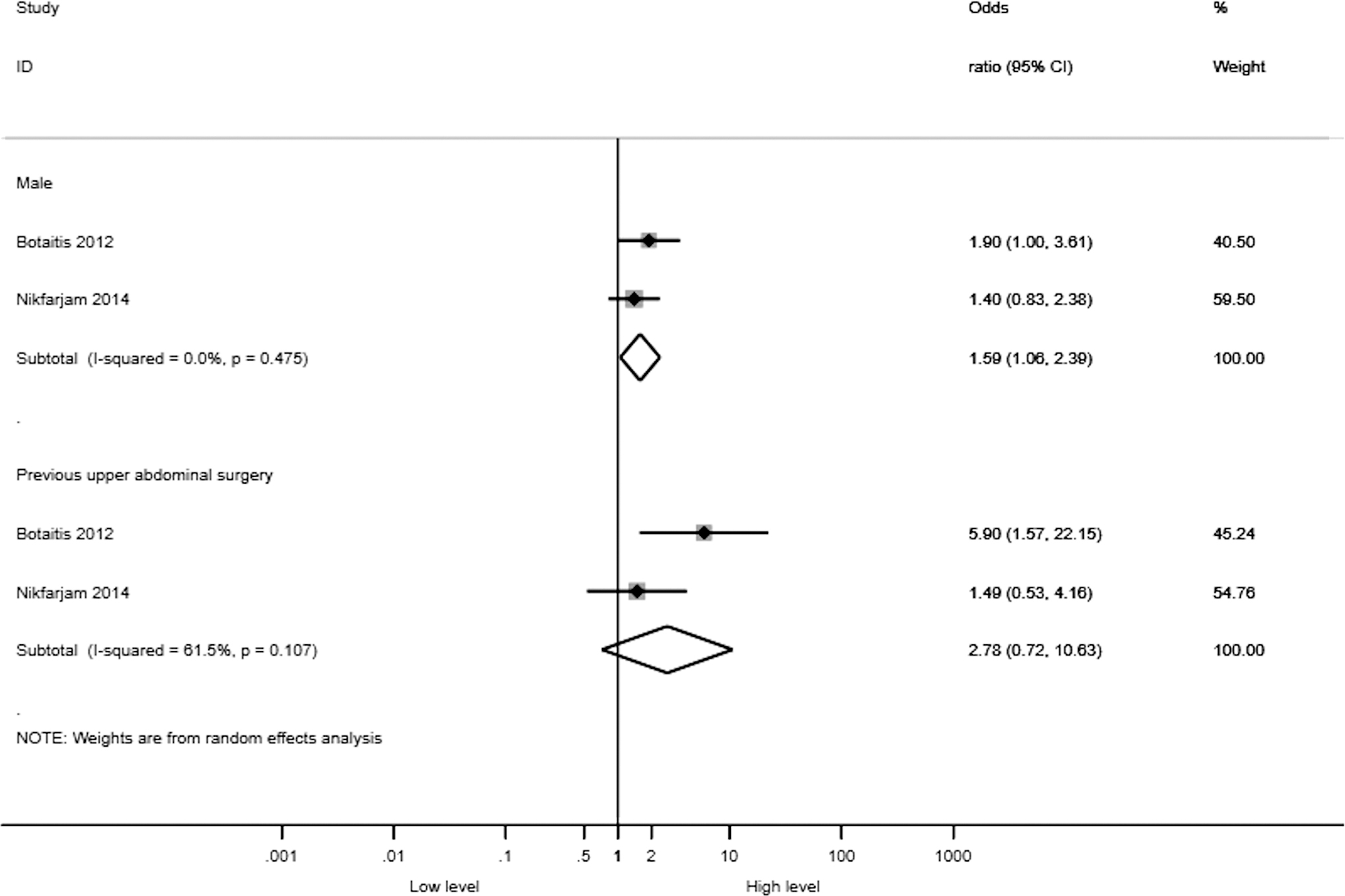
All complications (binary predictors). Meta-analysis of all complications showing the odds ratio and 95% confidence intervals for binary prognostic factors with at least two studies reporting the outcome. Male gender had good discriminatory ability to predict “all complications,” but there was no evidence of significant discriminatory ability for previous upper abdominal surgery to predict “all complications.”
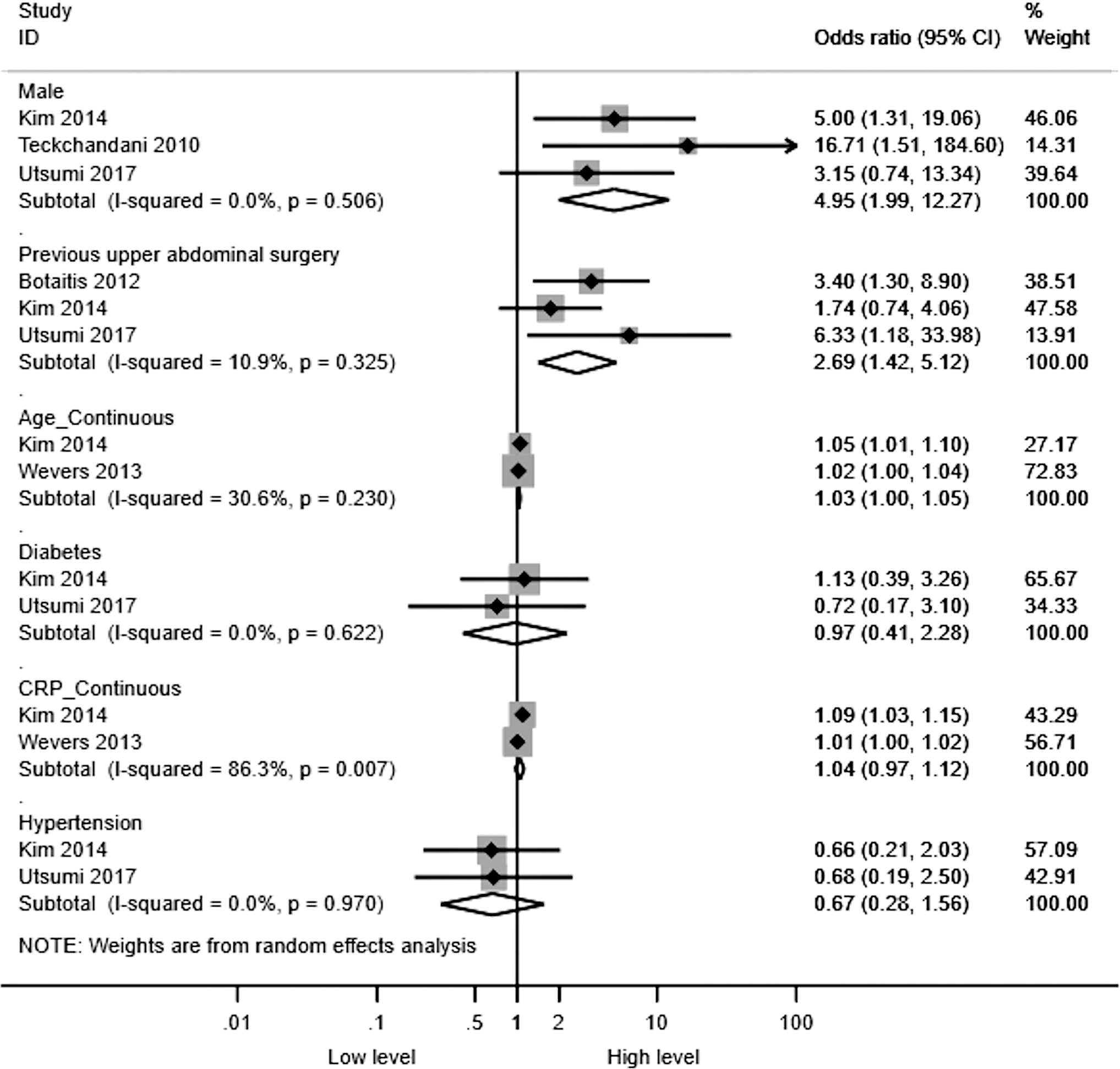
Conversion to open cholecystectomy (binary and continuous predictors). Meta-analysis of conversion to open cholecystectomy showing the odds ratio and 95% confidence intervals for binary and continuous prognostic factors with at least two studies reporting the outcome. Male gender, previous upper abdominal surgery, and age had good discriminatory ability to predict conversion, but there was no evidence of significant discriminatory ability for diabetes or hypertension to predict conversion.
All-cause mortality
Five studies (5655 participants) reported the ability of 5 prognostic factors or models (age, Charlson Comorbidity Index, Tokyo guidelines 2013 [TG13], number of dysfunctioning organs, and body mass index [BMI]) in predicting all-cause mortality.23,24,26,28,31 The median (interquartile range [IQR]) risk of all-cause mortality was 1.3% (0.8%–1.5%). TG13: Grade 3 (severe acute cholecystitis) versus Grade 1 (mild acute cholecystitis) was reported in two studies and had significant predictive ability (OR 5.08, 95% CI 2.79–9.26). The remaining factors were reported either in only one study or did not have significant predictive ability.
Major complications
Three studies (884 participants) reported the predictive ability of 3 prognostic factors or predictive models (Charlson Comorbidity Index, TG13, and BMI) in predicting major complications.23,24,26 One study reported major complications such as organ failure, bleeding, bile duct injury, and bile leak 23 ; another study reported major complications such as intrahepatic abscess, bleeding, bile leakage, biliary tract injury, and postoperative pancreatitis 24 ; and the last study reported major complications such as Clavien–Dindo Grades III or IV. 26 The median (IQR) risk of major complications was 3.3% (2.0%–3.9%). None of the factors reported in at least two studies had significant predictive ability.
Minor complications
Two studies (735 participants) reported the predictive ability of 2 prognostic factors or predictive models (Charlson Comorbidity Index, and BMI) in predicting minor complications.24,26 The median (IQR) risk of minor complications was 6.1% (5.4%–6.7%). None of the factors reported in at least two studies had significant predictive ability.
All complications
Six studies (1807 participants)24,26–28,30,32 reported the predictive ability of 24 prognostic factors or predictive models (male, previous upper abdominal surgery, age, albumin, alanine transaminase [ALT], aspartate transaminase [AST], bilirubin, Charlson Comorbidity Index, chronic liver disease, chronic obstructive airway disease, chronic renal failure, diabetes, glucocorticosteroid use, hemoglobin, hypotension, ischemic heart disease, platelets, P-Possum physiology score, previous biliary colic, Simplified Acute Physiology Score II [SAPS-II], temperature, white blood count [WBC], frailty score, and BMI) in predicting all complications. The median (IQR) risk of all complications was 10.0% (6.3%–15.0%). Male gender was reported in two studies and had significant predictive ability (OR 1.59, 95% CI 1.06–2.39). The remaining factors were reported either in only one study or did not have significant predictive ability.
Conversion to open cholecystectomy
Ten studies (6331 participants) reported the predictive ability of 40 prognostic factors or predictive models (male, previous upper abdominal surgery, age, diabetes, hypertension, adhesion to the adjacent organs [on preoperative scan], alkaline phosphatase, ALT, angle of the gallbladder, antiplatelet or anticoagulant use for cardiovascular disease, artificial neural network, associated organ dysfunction, AST, bilirubin, BMI, bulging of the abdominal muscle, Charlson Comorbidity Index, C-reactive protein [CRP], discriminant analysis, hyperattenuation of adjacent parenchyma, location of gallstone, logistic regression, Mirizzi syndrome, mucosal disruption, perforation, pericholecystic fluid, preoperative biliary intervention, short-axis diameter, wall thickening [on preoperative scan], WBC, and TG13) in predicting conversion to open cholecystectomy.22–26,29–33 The median (IQR) probability of conversion to open cholecystectomy was 16.0% (11.1%–19.3%). The following factors were reported in at least two studies and had significant predictive ability:
Male (OR 4.95, 95% CI 1.99–12.27) Previous upper abdominal surgery (OR 2.69, 95% CI 1.42–5.12) Age (OR 1.03, 95% CI 1.00–1.05 per year increase in age).
The remaining factors were reported either in only one study or did not have significant predictive ability.
Health-related quality of life
None of the studies reported the ability of any of the prognostic factors or risk prediction models in predicting health-related quality of life.
Calibration results
None of the studies reported results in a format from which calibration results could be calculated, that is, none of the studies presented the expected events based on the prognostic factor or prediction model, from which calibration could be calculated.
Discussion
Summary
In this systematic review and meta-analysis, we included 12 studies and 6827 people with acute cholecystitis in one or more analysis. Only few factors were reported in a format similar enough to combine for a meta-analysis. The remaining factors were analyzed in single studies or used different thresholds, and therefore, there is no information on their reproducibility and the results may be unreliable. This is of significant concern since the predictive ability of the factors that were measured in two or more studies differed considerably.
Among the prognostic factors reported in at least two studies, TG13 Grade 3 had increased risk of all-cause mortality compared with Grade 1. However, the timing of surgery in those who underwent cholecystectomy was not reported in this study and might have influenced the outcome. The studies were also at high risk of bias.
Furthermore, most studies included only people who underwent surgery and excluded participants who did not undergo surgery. There have been no RCTs of surgery versus conservative treatment in people with severe acute calculous cholecystitis. The role of percutaneous cholecystostomy either as a bridging treatment to cholecystectomy or as a definitive treatment in patients at high surgical risk is unclear, as indicated by a Cochrane systematic review. 52 An RCT published since the Cochrane review showed that in patients with acute cholecystitis and high physiological risk but considered eligible for surgery (acute physiology assessment and chronic health evaluation II/APACHE II scores of between 7 and 15), laparoscopic cholecystectomy performed by experienced surgeons had lower major complication rates than percutaneous cholecystostomy with no planned cholecystectomy. 53 Although the study was not powered to measure differences in mortality, 53 it is extremely unlikely that conservative treatment without surgery is an effective way of treating people with severe acute cholecystitis who are fit to undergo surgery. Therefore, it appears that despite the increased risk of mortality in TG13 Grade 3 compared with TG13 Grade I, early surgery seems to be the preferred option when possible. However, early referral to high-volume specialist centers, where patients can be optimized using integrated medical care and undergo early cholecystectomy, may decrease the complications11,12 and resulting mortality, and should be considered in people with TG13 Grade 3 acute cholecystitis.
None of the factors reported in at least two studies had significant predictive ability for major and minor complications analyzed separately. The definition used for major complications was also different across studies. Male gender was associated with increased risk of “all complications” and increased proportion of conversion to open cholecystectomy. The possible factors for poorer outcomes in males include increased skeletal muscle mass, 54 particularly in the trunk, 55 and increased visceral abdominal fat in males54,56,57 (which could make laparoscopic surgery more difficult) and delay in seeking medical help in males due to misguided perception of masculinity58,59 (which could mean that the males had more severe disease than females at the time of presentation to hospital). Another potential reason for delay in seeking medical help in males could be gender differences in pain perception between genders. In a systematic review, there was no evidence of difference in visceral pain threshold or intensity between males and females. 60 However, this information is based on two studies including just 38 participants. Therefore, the reasons for the difference in the complications and conversion between males and females are not clear but may be due to a combination of the above factors. Again, referral to high-volume specialist centers is an option, particularly because the gallstone incidence and operations are twice as frequent in females as males, that is, fewer patients need referral to specialist services.61,62 However, this may need reorganization of services if one-third of patients with acute cholecystitis have to be referred to a high-volume or specialist center.
Previous upper abdominal surgery is a risk factor for conversion to open cholecystectomy. This is expected because of the intra-abdominal adhesions related to previous upper abdominal surgery. In a data linkage study in Scotland conducted in the era of open surgery, of 8717 patients who underwent upper abdominal surgery, 321 patients (3.7%) had hospital readmissions directly related to intra-abdominal adhesions and another 1962 patients (24.8%) had hospital readmissions possibly related to intra-abdominal adhesions. 63 Therefore, referral of patients with previous upper abdominal surgery to specialist centers can be considered, as the risk of complications and proportion of patients requiring conversion from laparoscopic to open cholecystectomy are lower when performed by specialists.11,12
Older age had a minor increase in the conversion to open cholecystectomy. However, the increase is cumulative, that is, elderly patients may have a clinically important increase in conversion to open cholecystectomy compared with young people. Various confounding factors such as comorbidities and higher incidence of upper abdominal surgery may contribute to the increased probability of conversion to open cholecystectomy.
Applicability of the evidence
We restricted our selection to studies that included only patients with acute calculous cholecystitis. Most studies included only patients undergoing cholecystectomy for acute cholecystitis. Therefore, the findings of this review are applicable only in patients undergoing cholecystectomy for acute cholecystitis. We included only preoperative factors or risk models based on preoperative factors. Therefore, the findings of the review are applicable only before surgery is performed and does not include intraoperative or postoperative findings. There are likely to be other intraoperative or postoperative factors such as bile duct injury during surgery or severe adhesions found intraoperatively or postoperative bile leak that affect the clinical outcomes.
The Tokyo guidelines 2018 severity grading criteria adopted the TG13 severity grading criteria in predicting outcomes in people with acute calculous cholecystitis. 64 Therefore, the results of TG13 severity grading criteria are applicable to TG18 severity grading criteria as well, although the management algorithms of TG13 and TG18 based on the severity grading criteria were different.
Quality of evidence
The risk of bias in the studies was high because of one or more reasons described in the Results section. There was significant heterogeneity in the thresholds used for measurement. Most of the prognostic factors at a particular threshold were reported in only one study. Many of these factors are routinely measured such as age, BMI, coexisting diabetes, and hypertension. Furthermore, most of the outcomes are routinely measured outcomes such as mortality, major complications, and minor complications; yet, only a few studies reported these outcomes. This raises the possibility of publication bias. Therefore, there is significant uncertainty in the ability of the prognostic factors or risk prediction models in predicting outcomes in patients with acute cholecystitis. This uncertainty can impede shared decision-making.
Strengths and weaknesses
Two people selected studies and extracted data independently. We did not apply any language restrictions and searched a wide range of medical databases. We assessed the risk of bias in the studies using PROBAST, the tool currently recommended for assessing the risk of bias in prognostic studies.
The major weakness of the review is that we had to use search filters for identifying the studies. There may be other clinical studies that looked at the prediction of different factors without mentioning terms related to risk prediction or prognosis in the title, abstract, or keywords. These studies would have been missed by using the filter. These may be related to the predictive ability of the outcomes, contributing to reporting bias. However, one has to be pragmatic and choose between performing a systematic review using these filters versus attempting to seek information from an unmanageable number of full texts, making the review impossible to complete.
We have limited the prognostic factors to preoperative factors. This is because our main objective was to determine the best method to predict the risk of death, complications, health-related quality of life, and conversion to open cholecystectomy preoperatively in patients with acute cholecystitis. We acknowledge that there are several intraoperative factors that could influence these outcomes; however, such intraoperative factors will not be available at the time of informed decision-making about the treatment. Future studies should consider adjusting for surgeon-level or center-level average levels of intraoperative factors while developing the prognostic models that can be used preoperatively.
Conclusions
There is significant uncertainty in the ability of prognostic factors and risk prediction models in predicting outcomes in people with acute calculous cholecystitis. Based on data from studies of high risk of bias, TG13-Grade 3 severity may be associated with greater mortality than Grade 1 severity of acute cholecystitis. Referral of such patients to high-volume or specialist centers should be considered. High-quality studies are necessary to provide better information on prognostic information in people with acute cholecystitis and improve shared decision-making. Such studies should be prospective, of adequately large sample size to ensure that there are at least 100 events for the outcome measured, and should use blinded collection of prognostic factors and outcomes when possible. They should also consider adjusting for surgeon-level or center-level average levels of intraoperative factors.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.