
Abstract
Morbid obesity afflicts one third of the population in the United States and decreases life expectancy by 5–20 years. Laparoscopic Roux-en-Y gastric bypass (LRYGB) has been an established operation for the treatment of morbid obesity for nearly three decades. There are several different techniques for performing a LRYGB. We describe our circular stapled gastrojejunostomy technique and our preoperative and postoperative management of patients.
Introduction
Laparoscopic Roux-en-Y gastric bypass (LRYGB) has been one of the standard operations for the treatment of morbid obesity for nearly 3 decades. It was developed in 1994 by Dr. Wittgrove and Dr. Clark. 1 Since then various surgical techniques to perform it have been described including hand-sewn, use of linear or end to end anastomosis (EEA) staplers. 2 Although, the way in which it is performed has been debated, the results of the procedure have stood the test of time. After LRYGB, patients have durable weight loss, with positive effects on comorbidities like diabetes and gastroesophageal reflux disease. 3 Although laparoscopic sleeve gastrectomy (LSG) has surpassed RYGB as the most common operation for the treatment of morbid obesity, LRYGB is still a valid choice as it offers better control of reflux and diabetes mellitus type II. 4 In this chapter, we will describe our technique for performing LRYGB using an EEA stapler.
Patient Evaluation and Selection
Patients who wish to undergo bariatric surgery are seen first in our multidisciplinary clinic. At their initial visit, they meet with a dietician, psychologist and their future surgeon. The dietician better understands the patient's relationship with food and the behaviors that may have led them to become morbidly obese (or remain morbidly obese). Once patients have an understanding of their own food habits, they can begin to make changes and start the weight loss process. The psychology visits identify any potential mental health issues that may pose a risk during or after surgery. For example, a patient with undiagnosed/untreated depression or eating disorders may develop maladaptive eating patterns that may impair their health in the postoperative period and put them at risk for dehydration, readmission, or nutritional deficiencies. The psychology evaluation also helps identify if the patient has adequate social support and if they understand the gravity of the decision that they are making.
The surgeon is the last component of the initial visit. A careful history and physical examination is completed. Comorbidities that may be related to surgery are identified such as diabetes, hypertension, obstructive sleep apnea, and gastroesophageal disease. It is during this visit that we discuss patient risk factors that guide the choice of a bariatric operation. For example, patients with severe gastroesophageal reflux disease are likely to be better served with an RYGB.3,5,6 The available data on the function and presence of pathologic level of acid in the esophagus consistently show the LSG is an inferior option. In addition, there is emerging evidence that patients with preoperative gastroesophageal reflux disease (GERD) who undergo an LSG are more likely to be reliant on proton pump inhibitors, and require conversion to an RYGB or develop de novo Barrett's esophagus. The head to head comparison of the LSG and RYGB outcomes indicates that GERD is vastly improved in those who opted for an RYGB. 5
We typically follow the National Institutes of Health Consensus guidelines for bariatric surgery and offer RYGB to patients with a BMI of 35 with an obesity-related comorbidity, or BMI ≥40. For BMI ≥50 we are more likely to recommend an RYGB or biliopancreatic diversion with duodenal switch (BPD-DS) as this operation has better long-term effects for the super morbidly obese compared to LSG. If the patient does not wish to undergo a BPD-DS, then we recommend RYGB over LSG for the super morbidly obese as it has better mid and long-term outcomes for weight loss and resolution of comorbidities. 7 Once this visit is complete, the patient begins the weight loss journey.
Although, there is no mandated weight loss, in high BMI patients, we may suggest preoperative weight loss. The purpose of this is to kick start their healthy eating and exercise habits and to create a routine that they can continue postoperatively. After the initial visit, we perform an esophagogastroduodenoscopy. The purpose of this study is to identify any hiatal hernias, Barrett's esophagus, cancer, or other anatomic abnormality that would affect our procedure choice. 8 This has been debated and current recommendations by both SAGES and ASMBS are for the decision to be individualized. Obese patients have a significant risk of developing cancer. 9 We feel the risk of missing a malignancy by deferring an esophagogastroduodenoscopy outweighs the risk of the procedure itself. A barium swallow has been shown to have low sensitivity in primary bariatric surgery and therefore is only obtained in revisional cases. 10
We also obtain basic laboratory studies of serum chemistry, vitamin and mineral levels, and complete blood counts. A standard chest radiograph and an electrocardiogram are used to screen for pulmonary and cardiac disease respectively. Anyone with a history of cardiac disease will undergo cardiac clearance before surgery. Once the preoperative checklist is complete, the patient is scheduled for surgery and evaluated by an anesthesia provider before surgery.
Our institution utilizes an expedited recovery after surgery. The purpose of this bundle is to minimize narcotics, provide a judicious use of fluids, and encourage early ambulation. Patients have prescriptions filled before surgery (with the exception of narcotic pain medication) and risk of deep vein thrombosis and pulmonary embolism is calculated in the office. If they qualify for prophylaxis, they are expected to fill their prescription preoperatively, so they may use this medication once they are discharged from the hospital.
In the pre-op area, patients are provided non-narcotic analgesia to minimize their narcotic requirements during general anesthesia. Deep vein thrombosis prophylaxis is also provided to minimize the risk of venous thromboembolism.
Technique
Patients are positioned supine on the operating table. Their arms are padded and secured to arm boards The extremities are positioned at 45° from the bed, to minimize risk of peripheral nerve injury. Two safety straps are positioned over the patient's hips and legs. A footboard is used to stabilize the feet and provide support of position changes during the case. Perioperative antibiotics are administered within 60 minutes of incision time. The patient's abdomen is then prepped from the nipple line to the pubis and to posterior axillary lines bilaterally.
The Medtronic VersaStep System (Minneapolis, MN) is used in bariatric cases. A STEP needle is inserted into the abdomen at Palmer's point in the left upper quadrant. After a saline drop test is performed, the peritoneal cavity is insufflated with carbon dioxide to 15 mm of Hg. A 5 mm incision is made in a supra umbilical, left paramedian position. A 5 mm optical port and a zero-degree laparoscope is inserted through this into the abdominal cavity. The abdomen is inspected for injury related to the STEP needle and trocar. Additional ports are placed under direct visualization. Final port placements are 5 mm port in the right lateral abdominal wall, 12 mm port in the right supra umbilical para median space, 12 mm in the left supra umbilical para median space, and 5 mm port in the left lateral abdominal wall. A 5 mm stab incision is made longitudinally in the sub-xiphoid area to facilitate placement of a Nathanson liver retractor (Cook Medical, IN). A transversus abdominus plane block is performed using lipoidal bupivacaine after initial port placement.
The goal of the operation is to create a 50 cm biliary limb, a 30 cc stomach pouch, and a 150 cm Roux limb. The gastrojejunal anastomosis is antecolic and antegastric. The case begins by placing the patient in slight reverse Trendelenburg position and measuring the bowel from the ligament of Treitz. The bowel is rotated clockwise and divided 50 cm distal to the ligament of Treitz using a 60 mm tan load endo GIA laparoscopic stapler. The associated mesentery is not divided here. The purpose of preserving the mesentery is to avoid creating a large defect for future internal hernia formation and having good blood supply to the divided bowel. In our experience, this does not place excessive tension on the anastomosis.
Next, the bowel is rotated another 150 cm counterclockwise. A harmonic scalpel is used to create enterotomies in the future biliary limb and the Roux limb for creating a stapled jejunojejunostomy. A 45 mm tan load linear cutting stapler is used in a double-fire technique to create the anastomosis (Figs. 1 and 2). The common enterotomy is then closed transversely using a 60 mm tan load stapler. The staple lines are carefully inspected for hemostasis, disruption, and narrowing. This completes the fully stapled jejunojejunostomy (Fig. 3).
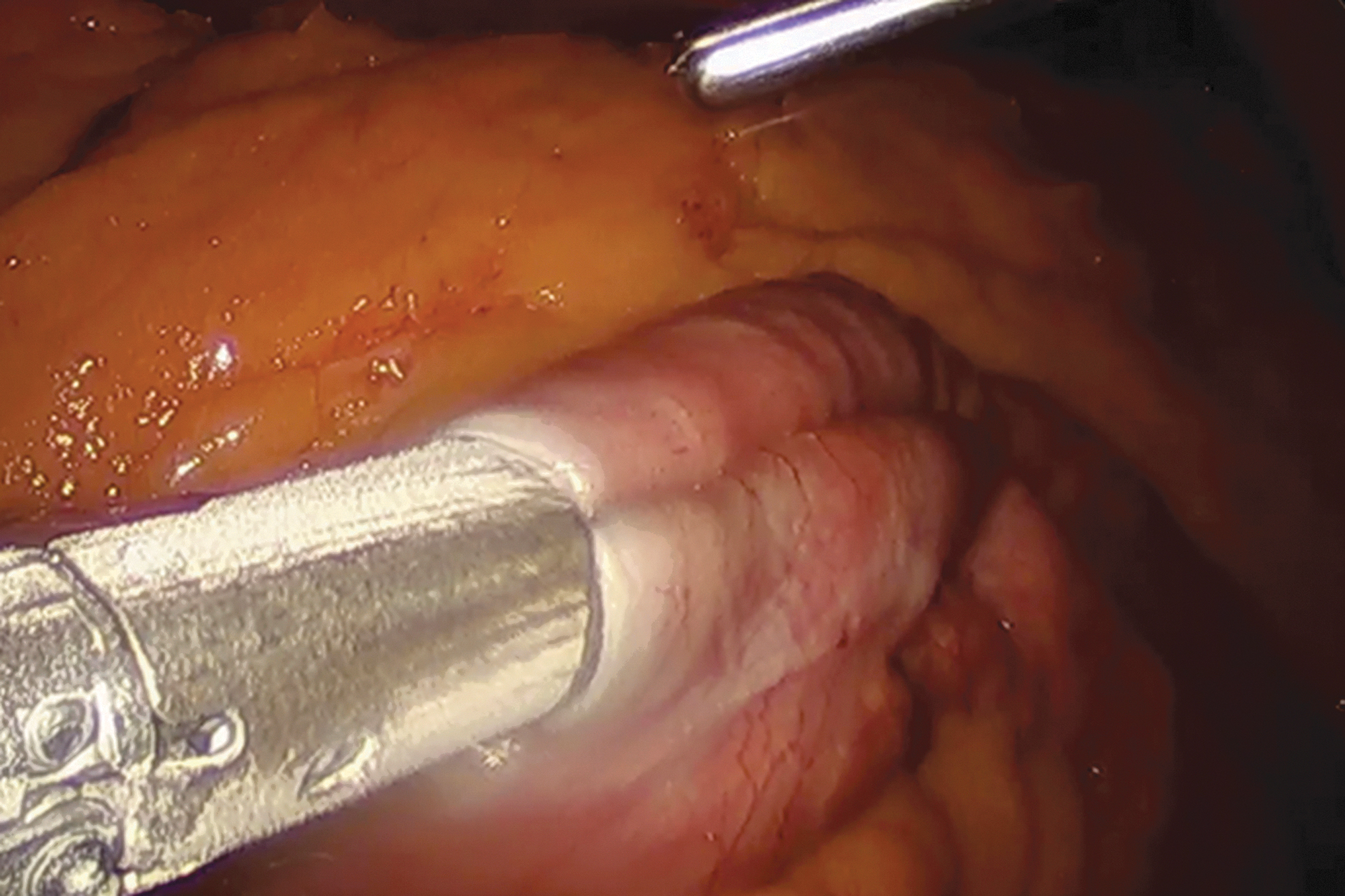
Creation of jejunostomy.
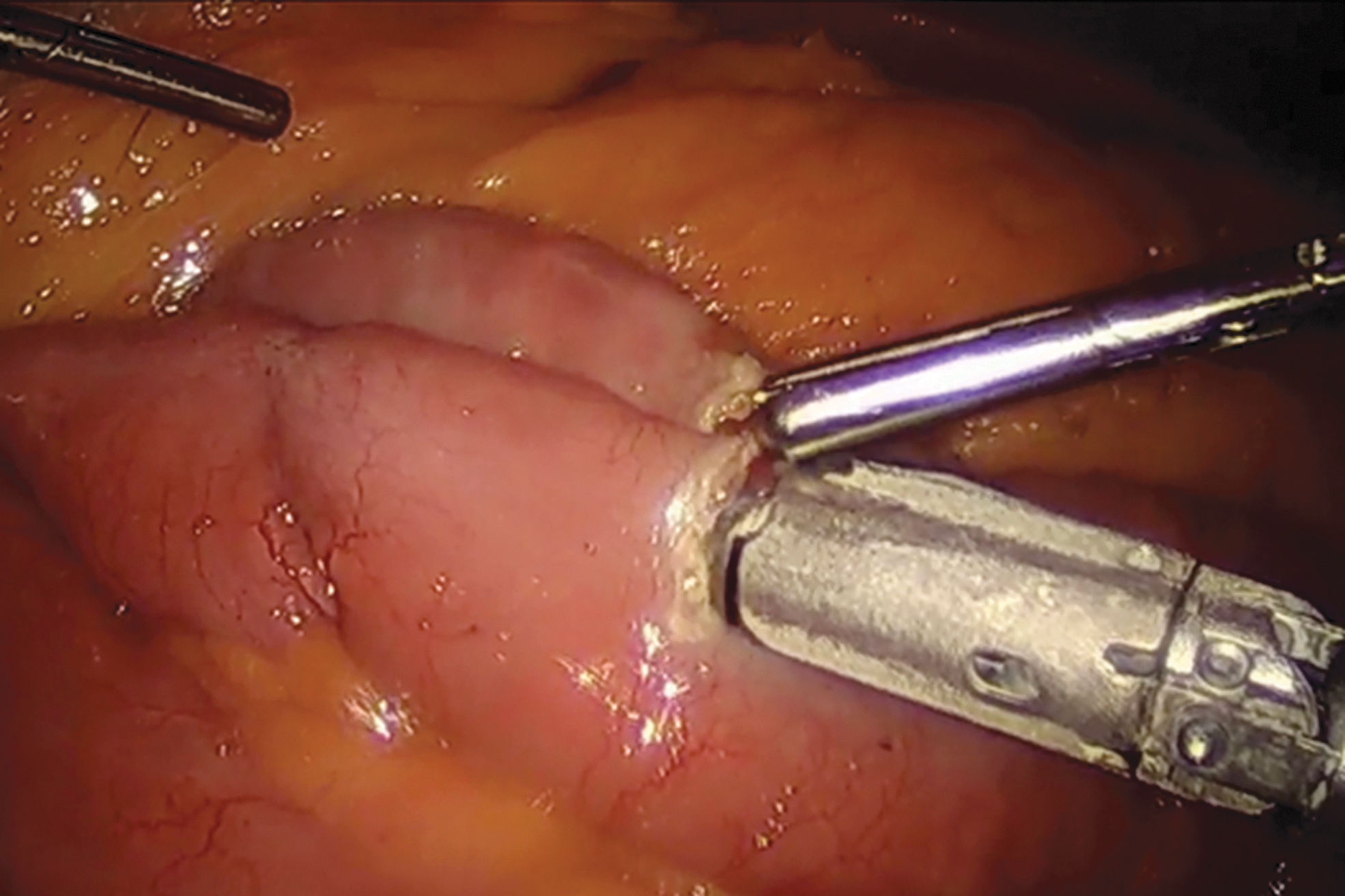
Bidirectional staple fire.
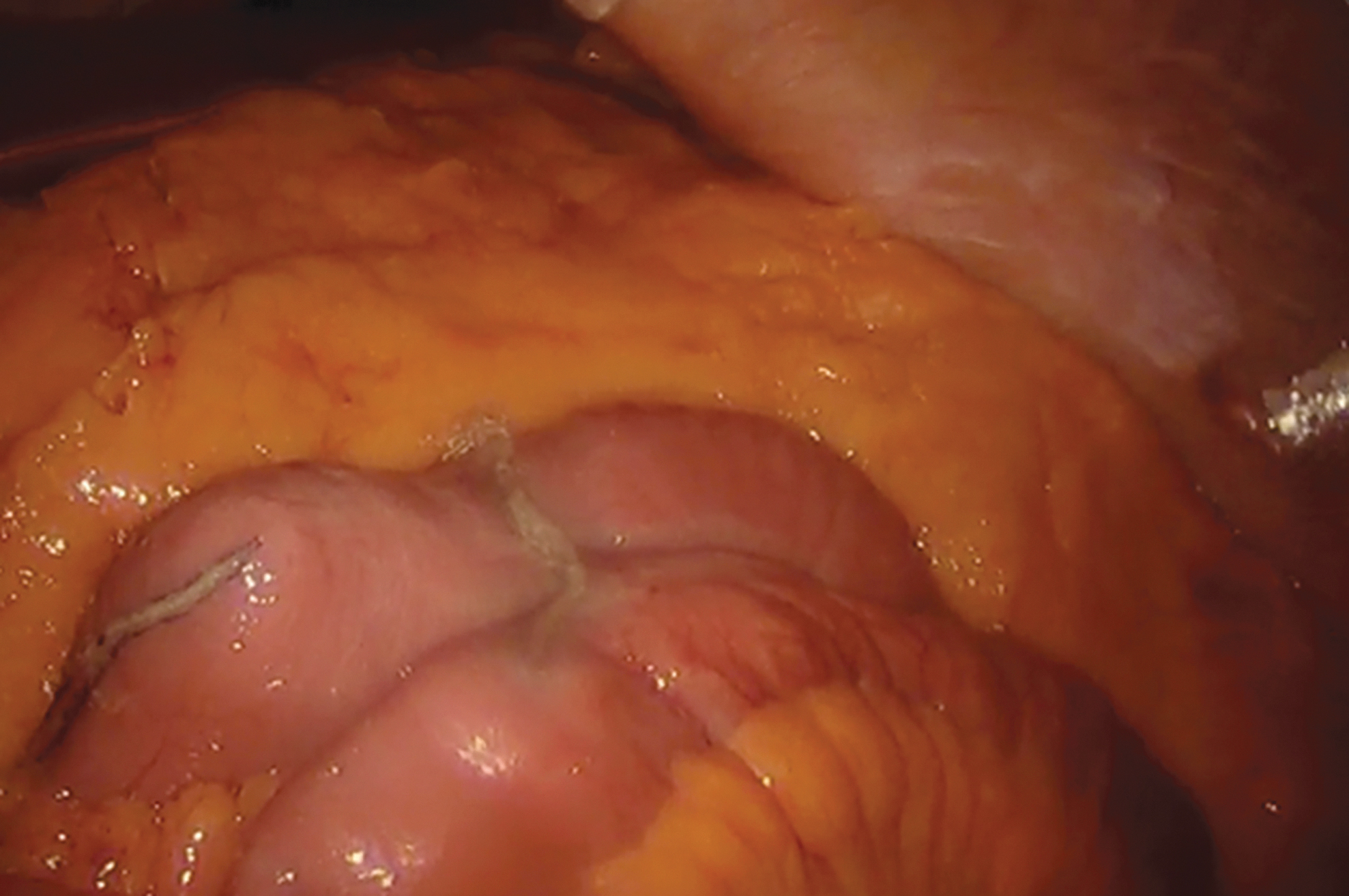
Completed jejunostomy.
A straight clamp is passed in the epigastric area to create a tract through which the Nathanson retractor is passed to elevate the left lobe of the liver and expose the hiatus and gastroesophageal junction clearly. After the liver retractor is secured to the post, the hiatus is inspected for the presence of a hiatal hernia. If a hiatal hernia is present, it is repaired as part of the operation.
The creation of the gastric pouch begins with dissection of the lesser curvature of the stomach. The stomach pouch is sized to 30 mL using a sizing balloon. The peri-gastric technique is used to gain entry into the lesser sac, taking care to preserve the main trunks of the vagus nerve, the lesser curvature vasculature and the left gastric artery (Fig. 4). A combination of gentle blunt dissection with laparoscopic graspers and the harmonic scalpel is used to enter the lesser sac. Once entry is gained into the lesser sac, a 60 mm tan linear cutting stapler is fired nearly perpendicular to the lesser curve to create a landing zone for the anvil of the EEA stapler. Additional 60 mm tan loads are used to complete the division of the stomach and create a 30 cc gastric pouch.

Perigastric dissection.
The alimentary limb is then brought up to the epigastrium, ensuring that there is no twist in the mesentery.
The next step is to create the gastrojejunostomy using a size 21 EEA OrVil system (Medtronic, MN). The OrVil is passed by the anesthetist and requires excellent communication between them and the surgical team. The delivery tubing of the OrVil is passed trans-orally by the anesthetist until it is seen indenting the stomach pouch. A small gastrotomy is made overlying the indentation using the harmonic scalpel, and is typically posterior to the staple line of the pouch (Fig. 5). The gastrotomy is barely the size of the tip of the tubing that delivers the anvil. The tube is then pulled through the gastrotomy into the abdominal cavity until the anvil is positioned well in the stomach pouch. The 12 mm port in the left anterior axillary line is removed and the port tract is dilated using a straight clamp. The OrVil 21 stapler is passed through this tract. The blind end of the Roux limb is brought up to the epigastrium and an opening is made in the bowel using the harmonic scalpel that is large enough to easily accommodate the EEA stapler. An EEA stapled anastomosis is created by engaging the stapler with the anvil (Fig. 6). The stapler with anvil is retrieved from the left 12 mm port site. The enterotomy for the stapler is closed with a linear cutting tan 60 stapler (Fig. 7).
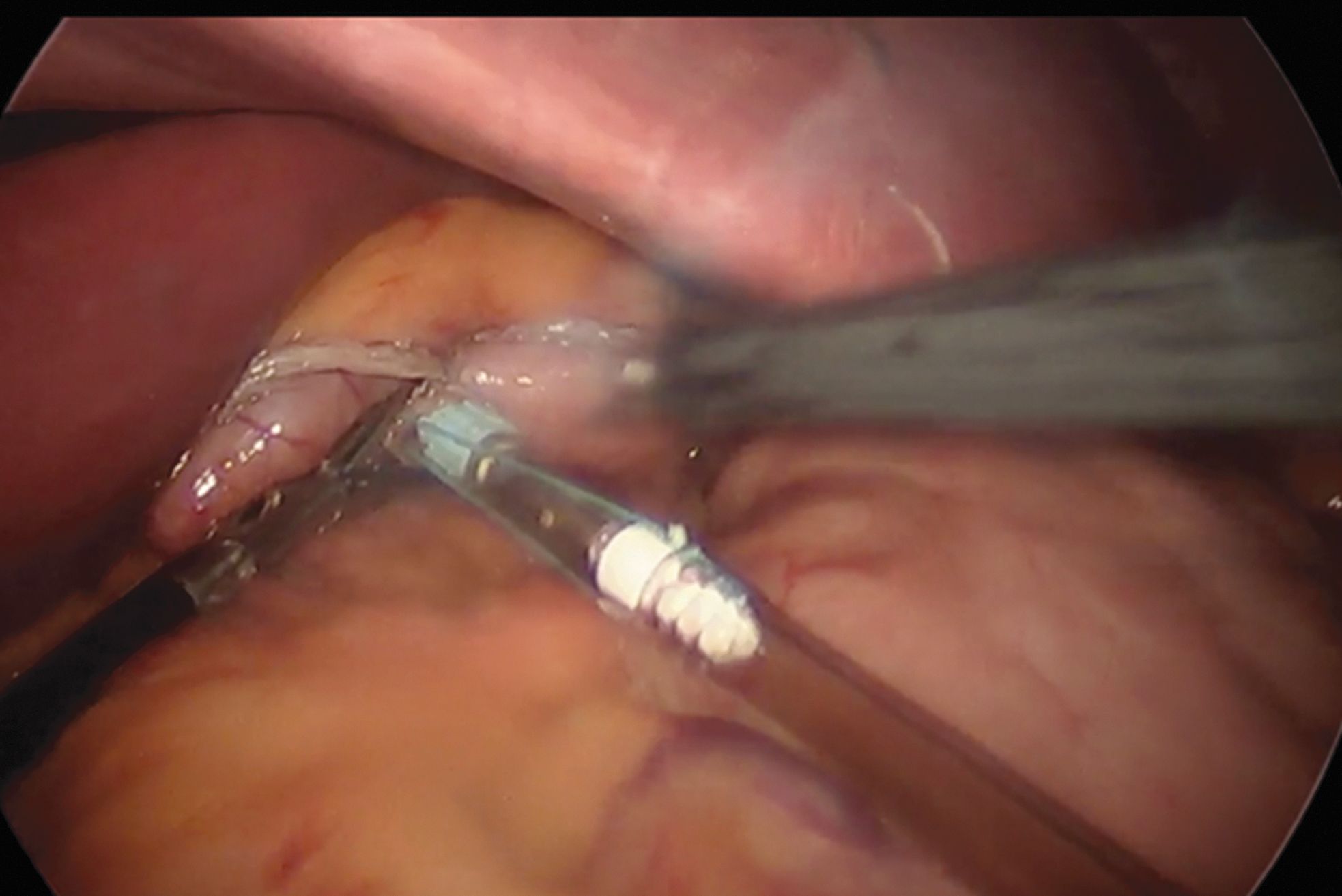
Delivery of anvil in gastric pouch.

End to end anastomosis gastrojejunostomy.

Completed gastrojejunostomy.
The Roux limb is approximated with a permanent suture to the remnant stomach to take the tension off and prevent twisting. The mesenteric defect between the transverse mesocolon and the alimentary limb is closed with running nonabsorbable suture. The mesenteric defect between the alimentary limb and biliary limb is also closed using nonabsorbable suture in a continuous fashion.
An adult upper endoscopy scope is passed through the mouth and into the esophagus and down to the gastric pouch. The gastrojejunal anastomosis is inspected and confirmed for patency and hemostasis. We then perform an air leak test after placing a bowel clamp on the Roux limb externally. The air leak test completes the laparoscopic RYGB. The liver retractor is removed, abdomen desufflated, and the incisions closed with absorbable suture.
Postoperative Course
Postoperatively all patients are admitted to the surgical floor and are maintained on continuous cardiac monitoring for 24 hours. They are started immediately on a stage 2 diet, which consists of clears liquids and proteins. Multimodal pain control is utilized for postoperative pain management and minimal narcotics are administered as needed. Most LRYGB patients stay overnight in the hospital and are discharged when they are tolerating 64 fluids ounces and 60 g of protein. All discharged patients receive a follow-up call within 72 hours of discharge. Their first postoperative group is at 2 weeks, which coincides with their postsoperative appointment with a medical provider. At this visit their progress is reviewed, incisions are inspected, and they are advanced to a stage 3 diet.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.