
Abstract
Achalasia manifests as failure of relaxation of the lower esophageal sphincter resulting in dysphagia. Although there are several medical and endoscopic treatment options, laparoscopic Heller myotomy has excellent short- and long-term outcomes. This article describes in detail our surgical approach to this operation. Key steps include extensive esophageal mobilization, division of the short gastric vessels, mobilization of the anterior vagus nerve, an extended gastric myotomy (3 cm as opposed to the conventional 1–2 cm gastric myotomy), a minimum 6 cm esophageal myotomy through circular and longitudinal muscle layers, and a Toupet partial fundoplication. We routinely use intraoperative endoscopy both to check for inadvertent full-thickness injury and to assess completeness of the myotomy and the geometry of the anti-reflux wrap.
Introduction
Achalasia is defined as a failure of lower esophageal sphincter relaxation and a lack of esophageal peristalsis. There are three subtypes of achalasia, classified by the degree of disordered esophageal peristalsis: Type I minimal contractility, Type II pan-esophageal pressurization, and Type III premature or spastic contractions. 1 Although there are numerous medical and endoscopic treatments for achalasia, the focus of this article will be the surgical (Heller) myotomy, which involves the division of the circumferential and longitudinal muscle fibers extending from the proximal stomach onto the distal esophagus. The major controversies related to the Heller myotomy are the length of the myotomy and the choice anterior 180° (Dor) versus posterior 270° (Toupet) partial fundoplication after the myotomy. Although this article describes the laparoscopic approach to myotomy, we also have experience in robotic-assisted myotomy. The steps and fundamental technique are the same with robotics and laparoscopy, but with some minor differences in patient positioning and port setup.
We have previously published our findings that an extended distal myotomy of 3 cm through the gastric sling fibers combined with a Toupet fundoplication is associated with a statistically significant decrease in the rate of recurrent dysphagia requiring intervention compared with a standard 1.5 cm myotomy with Dor fundoplication. 2 Based on these findings, we routinely perform an extended 3 cm gastric myotomy on our achalasia patients. The proximal length of the myotomy is less controversial, and most authors advocate for a minimum 6 cm extension proximally onto the esophagus to completely divide the lower esophageal sphincter. In the case of Type III achalasia with a spastic component, we will try to extend the myotomy as proximal as is technically feasible. Some surgeons have advocated using intraoperative esophageal distensibility (EndoFLIP, Medtronic, Inc.) to guide the extent of the myotomy, 3 but to date, data for this approach are limited and we consider this investigational.
It is clear that myotomy alone results in a high rate of postoperative gastroesophageal reflux and that addition of a fundoplication markedly reduces that risk. 4 Although some surgeons in the past have advocated for a 360° (Nissen) fundoplication, 5 most surgeons prefer a partial fundoplication to minimize risk of wrap-related dysphagia.
Regarding which type of partial fundoplication to perform after a myotomy, a multicenter randomized controlled trial (RCT) published by Rawlings et al. 6 compared Dor versus Toupet fundoplication after laparoscopic Heller myotomy and found no statistically significant difference in postoperative symptoms or objective acid reflux scores between the two types of fundoplication. These findings were confirmed by two other RCTs comparing Dor versus Toupet fundoplication after Heller myotomy for achalasia,7,8 and by two recently published meta-analyses.9,10 In addition, there are no differences in outcomes between Dor versus Toupet fundoplication after Heller myotomy, as both have similar rates of complications (2.3% versus 3.5%, respectively), postoperative gastroesophageal reflux (20.8% versus 28.2%, respectively), and treatment failure (8.5% versus 9.1%, respectively). 10 Thus, the decision whether to use a Dor versus Toupet fundoplication remains largely at the discretion of the surgeon.
That being said, in the Rawlings RCT (which our center participated in), 6 there was a statistically nonsignificant difference between the two anti-reflux options, with abnormal reflux seen in 10 of 24 patients after Dor fundoplication (41.7%) versus 4 of 19 in the Toupet group (21.0%). It is our opinion that most studies in achalasia are underpowered, and given the suggestion of better reflux control with a Toupet fundoplication, it is our preference to use it after myotomy. As an exception, we occasionally will not perform an anti-reflux procedure on patients undergoing a redo myotomy or on patients with a tortuous, severely dilated distal esophagus. Another exception is that we will perform a Dor fundoplication instead of a Toupet to cover a repair after an intraoperatively recognized, inadvertent mucosal injury. Otherwise, our standard approach is to perform an extended myotomy with a Toupet fundoplication, as described in this article.
Patient evaluation and selection
We obtain a preoperative manometry and upper gastrointestinal study to confirm the diagnosis of achalasia. We also perform an upper endoscopy to evaluate for any intraluminal lesions or strictures. Preoperatively, all patients receive nutritional education on the esophageal diet that they will need to follow for 4 weeks after surgery. They are encouraged to walk at least a mile daily in preparation for surgery and are instructed to follow a full liquid diet for 3 days before surgery.
Positioning
Patients are positioned supine on a split-leg table with arms out, secured with a soft wrap. Legs are secured with hip straps to support severe reverse-Trendelenburg positioning. We place a Foley catheter if the operation is expected to last longer than 3 hours, such as for patients with a history of previous upper abdominal surgery. All patients receive preoperative heparin and wear sequential compression devices before induction to minimize the risk of perioperative venous thromboembolism.
Port placement
We start with placement of a 12 mm port where the midclavicular line intersects the costal margin (Fig. 1). We first insufflate with a Veress needle and place an optical dilating trocar under direct vision. We then place an additional 12 mm camera port 2 cm lateral to midline in the patient's left abdomen, ∼12 cm below the costal margin. We insert 5 mm ports in the patient's left lateral abdomen and right upper abdomen, and then place an epigastric Nathanson retractor to retract the left lobe of the liver.
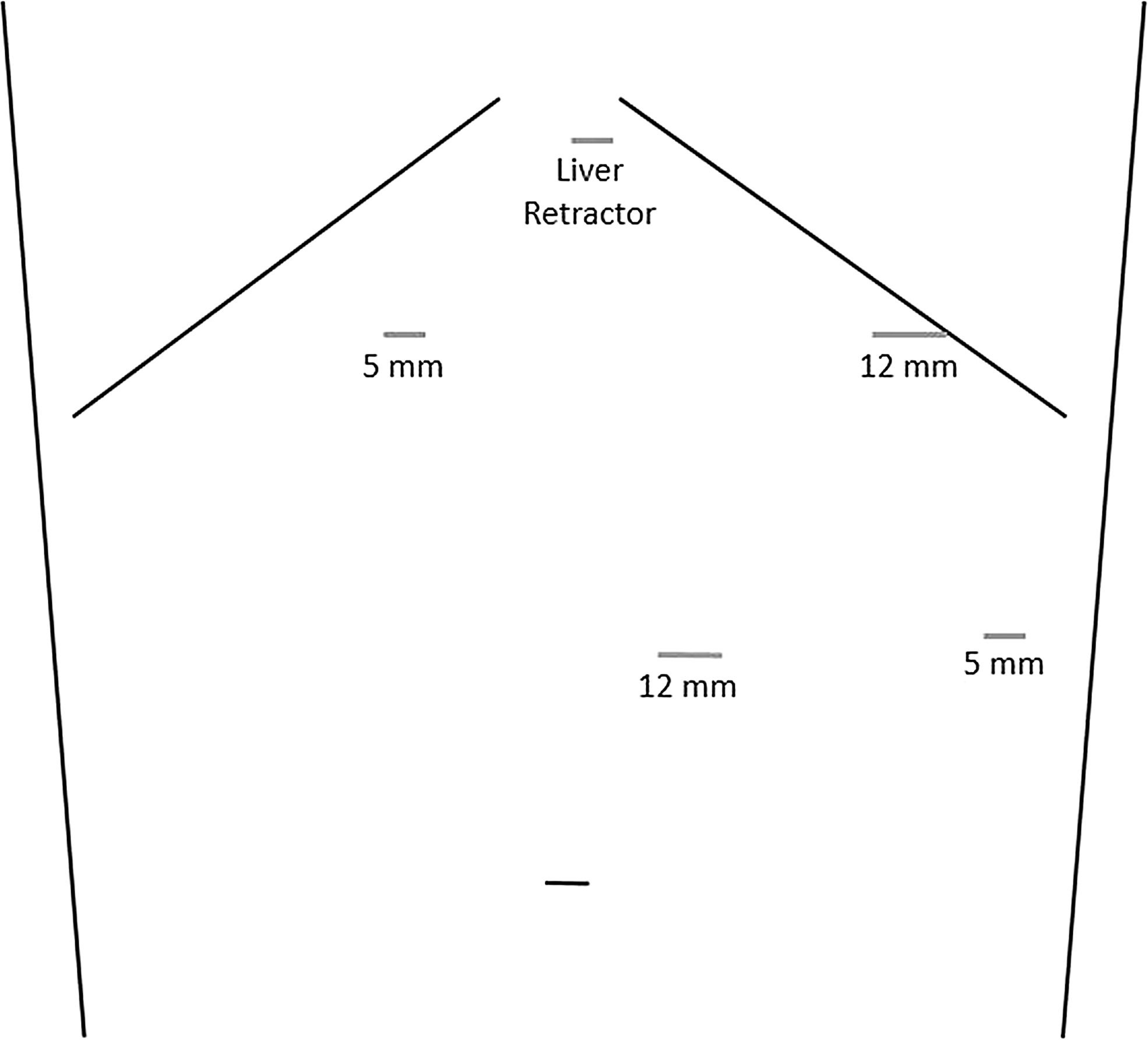
Port placement.
Initial esophageal mobilization
We start with esophageal mobilization on the patient's left crus. Although many surgeons begin their dissection on the patient's right, we typically begin on the left as we find that this helps create a space between the diaphragm, stomach, and spleen, which makes subsequent division of the short gastric vessels easier. This approach is also helpful in reoperative foregut surgery, where the right crus is often obscured by the liver and in close proximity to an adherent caudate lobe and inferior vena cava.
We begin by taking the gastroesophageal fat pad off the diaphragm and then opening the phrenoesophageal membrane with hook cautery at the base of the left crus. We then continue the dissection anteriorly along the edge of the crus, taking care to preserve the peritoneum over the crus (Fig. 2). We continue the dissection anteriorly across the top of the right crus while carefully preserving the left vagus nerve, which sits anterior to the esophagus at this level.
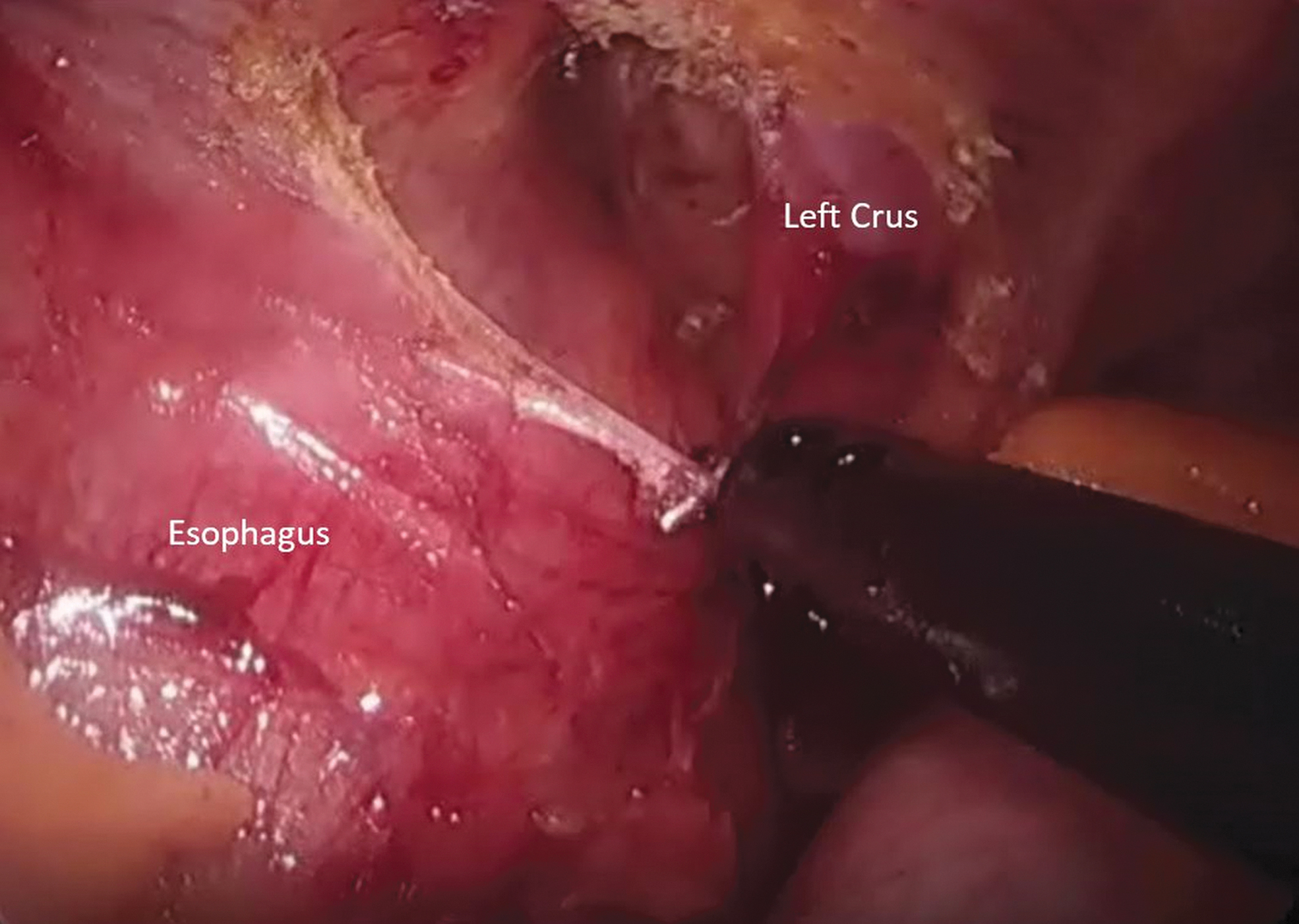
Mobilization of the left distal esophagus.
Division of the short gastric arteries
We enter the lesser sac through the greater omentum ∼10 cm distally along the greater curve of the stomach. We then divide the short gastric vessels with an advanced energy device (bipolar vessel sealer or ultrasonic dissector) and expose the base of the left crus. The posterior aspect of the fundus is cleared of all attachments to allow sufficient mobilization for the fundoplication (Fig. 3).
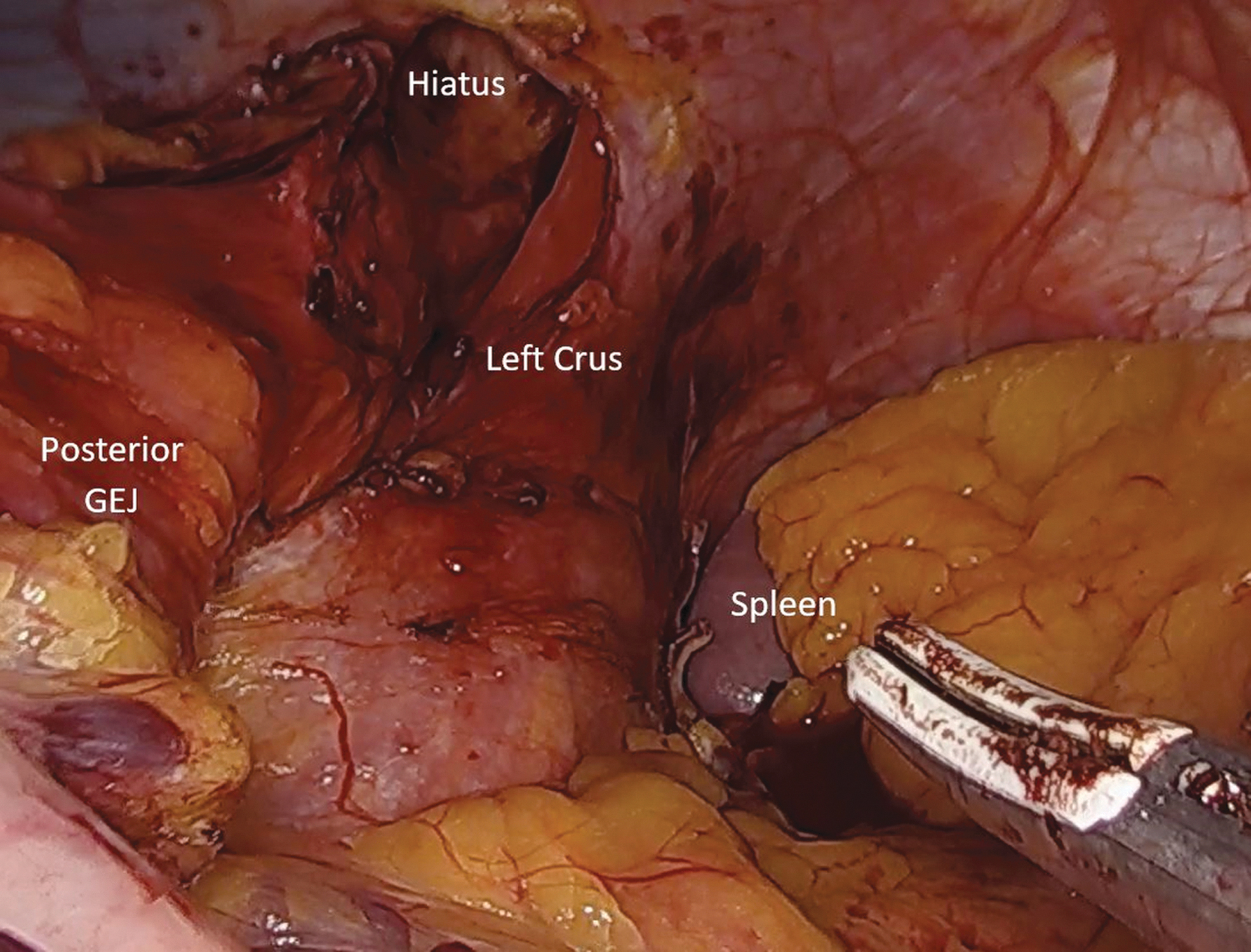
Mobilization of short gastric arteries and posterior fundus. GEJ, gastroesophageal junction.
Completion of the esophageal mobilization
We next enter the gastrohepatic ligament and proceed toward the top of the right crus to meet with the dissection that has already been performed from the left side. We then open the right phrenoesophageal membrane at the base of the right crus using hook cautery. We bluntly dissect anteriorly to meet with the previous dissection from the left. By dividing only the phrenoesophageal membrane off the crus while dividing nothing entering the mediastinum, we protect the esophagus and vagus nerves. We then dissect posteriorly to come under the esophagus and posterior vagus nerve, using the junction of the right and left crura as a guide. Once the gastroesophageal junction (GEJ) has been circumferentially mobilized, we place a Penrose drain around the GEJ to provide additional retraction (Fig. 4). We then mobilize the distal esophagus circumferentially for 7–8 cm primarily with blunt dissection, but use cautery or the vessel sealer as needed, taking care to avoid entry into the pleural space.

Distal esophageal mobilization using a Penrose drain for retraction.
Mobilization of the vagus nerve
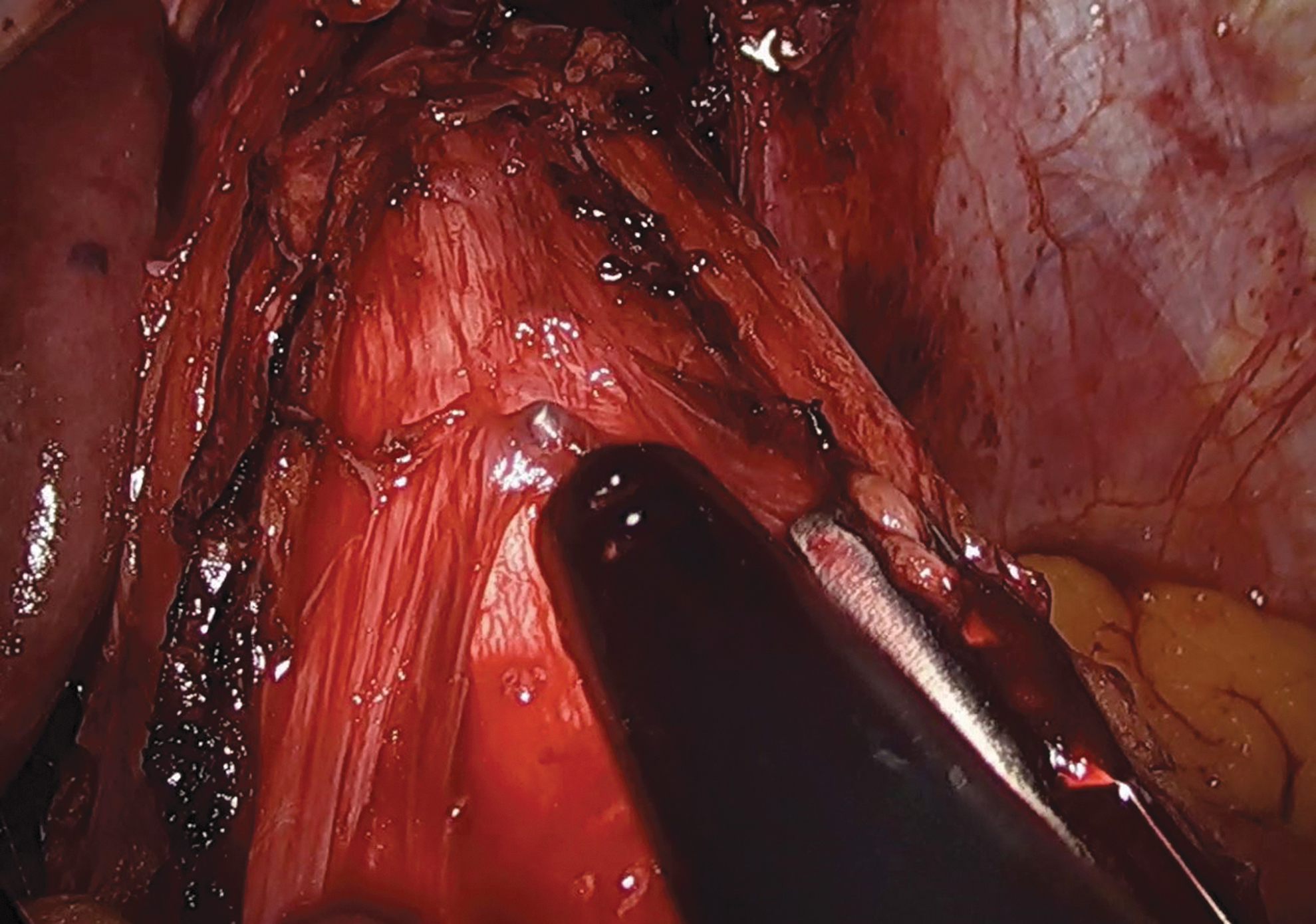
Next, we mobilize the GEJ fat pad off the stomach, beginning lateral (patient left) to the anterior vagus nerve. This allows retraction of the vagus by manipulating the fat pad, avoiding contact with the nerve itself. Placement of a 52 F lighted bougie at this time allows for better visualization of the tissue planes. We then lift the fat pad and anterior vagus nerve from the distal esophagus across the GEJ to allow space for the myotomy to cross under the vagus (Fig. 5).
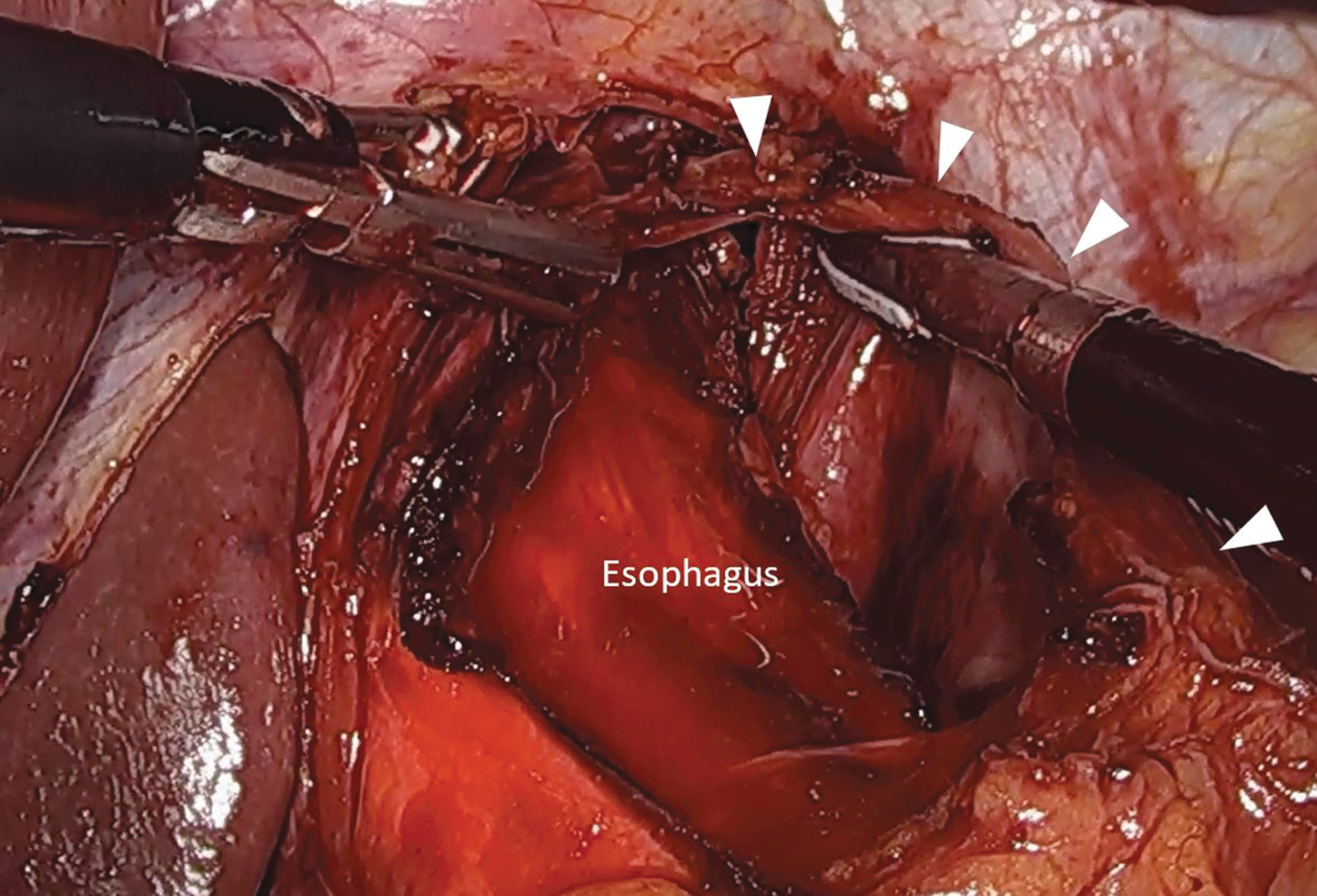
Mobilization of anterior vagus nerve (arrowheads) off the esophagus after placement of a lighted bougie.
Myotomy
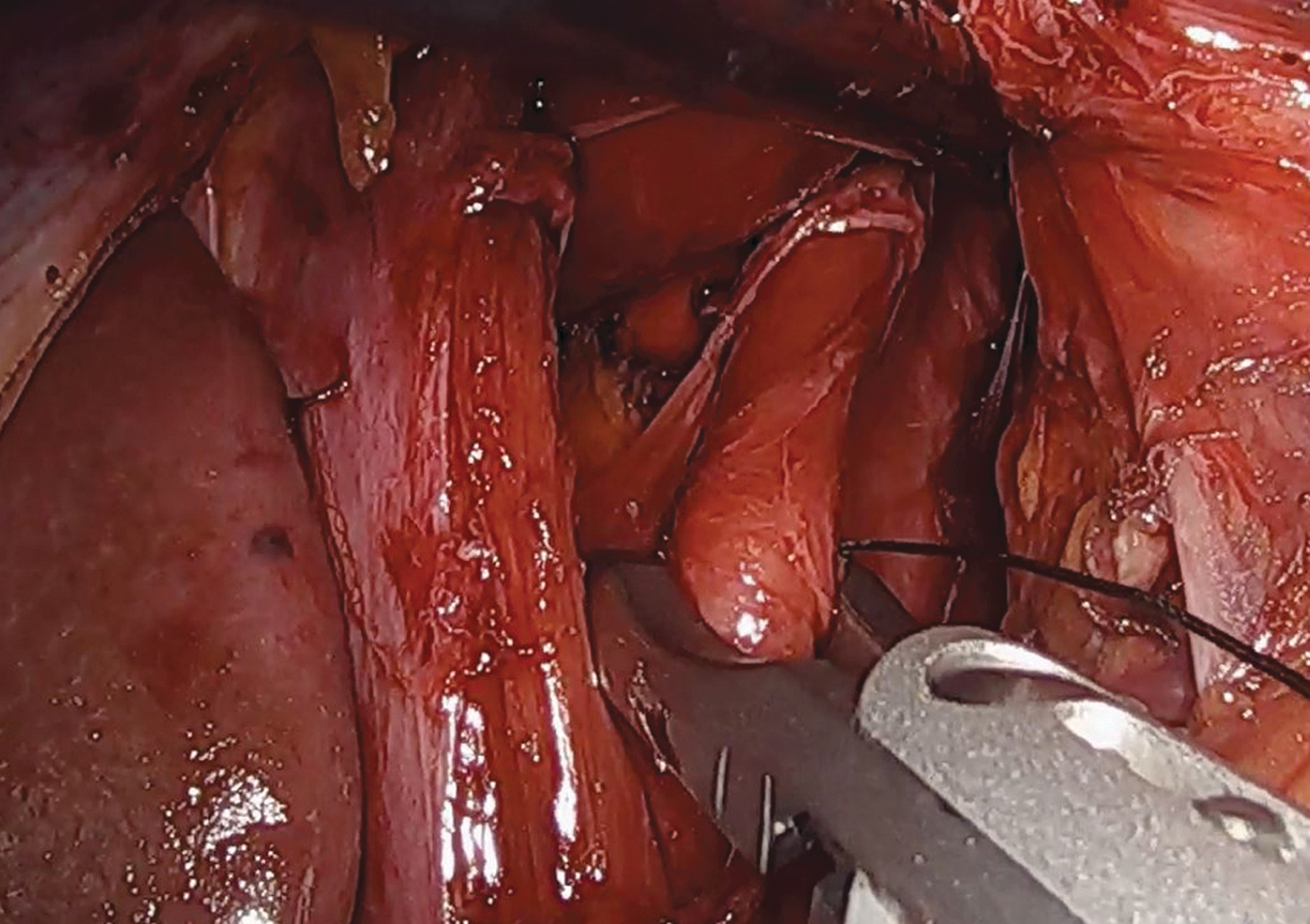
We begin the myotomy 3 cm distal to the GEJ (extended myotomy) using a cautery L-hook. The assistant helps to put the esophagus on stretch over the lighted bougie. The tip of the hook is then used to gently tease apart the muscle fibers, which are divided by gently lifting the muscle fibers until they fall apart (Fig. 6). We use minimal to no cautery to minimize risk of thermal injury to the mucosa. As the myotomy is extended proximally, we move the vagus nerve from the medial to the lateral side of the esophagus to allow the myotomy to proceed along the anterior aspect of the esophagus underneath the vagus. The esophageal myotomy is complete once it is at least 6 cm from the GEJ and proximal to any abnormal esophageal tissue.
Esophageal myotomy.
Closure of the hiatus
The hiatus is typically enlarged after esophageal mobilization and should be repaired to prevent slipping of the fundoplication. We prefer to reapproximate the crus with interrupted 2-0 permanent sutures (Fig. 7). We do not typically close the myotomy as tightly as we might in anti-reflux surgery or paraesophageal hernia repair, to avoid residual dysphagia from diaphragmatic pinch on the esophagus.
Hiatal closure.
Construction of the Toupet fundoplication
We feel that the proper geometry of the wrap is critical to prevent future problems. Many “slipped” fundoplications are actually improperly constructed wraps with too much posterior fundus behind the esophagus. To ensure proper wrap geometry, we feel that a marking stitch on the posterior fundus is critical. We use a 2-0 silk tag on the posterior fundus at a point 3 cm distal to the GEJ and 2 cm from the greater curve (Fig. 8). We then use the tag to bring the gastric fundus under the esophagus. We grasp the anterior fundus at a point 3 cm from the GEJ and 2 cm from the greater curve such that the fundus is suspended symmetrically relative to the greater curve between both graspers. We perform a “shoe-shine” maneuver to ensure that the fundoplication will be symmetric without any twisting or tension. We then construct the right (medial) aspect of the fundoplication, placing the first coronal stitch near the tag on the fundus, through the right myotomy edge, and through the right crus at the 10-o'clock position. Once the coronal stitch is secured, we remove the tag and Penrose drain. We place a posterior gastropexy stitch from the inferior aspect of the fundoplication to the base of the bilateral crus. We place two additional stitches between the right myotomy edge and the right side of the fundoplication, taking care to ensure that the sutures stay proximal to the GEJ. We then move to the left side of the wrap. We secure the previously identified symmetrical point (3 cm from the GEJ and 2 cm from the greater curve) to the left edge of the myotomy and the left crus at the 2-o'clock position, creating the posterior 270° partial wrap. Care must be taken to avoid inadvertently incorporating the vagus nerve during this process. We place two additional sutures from the left aspect of the fundoplication to the left edge of the myotomy (Fig. 9).
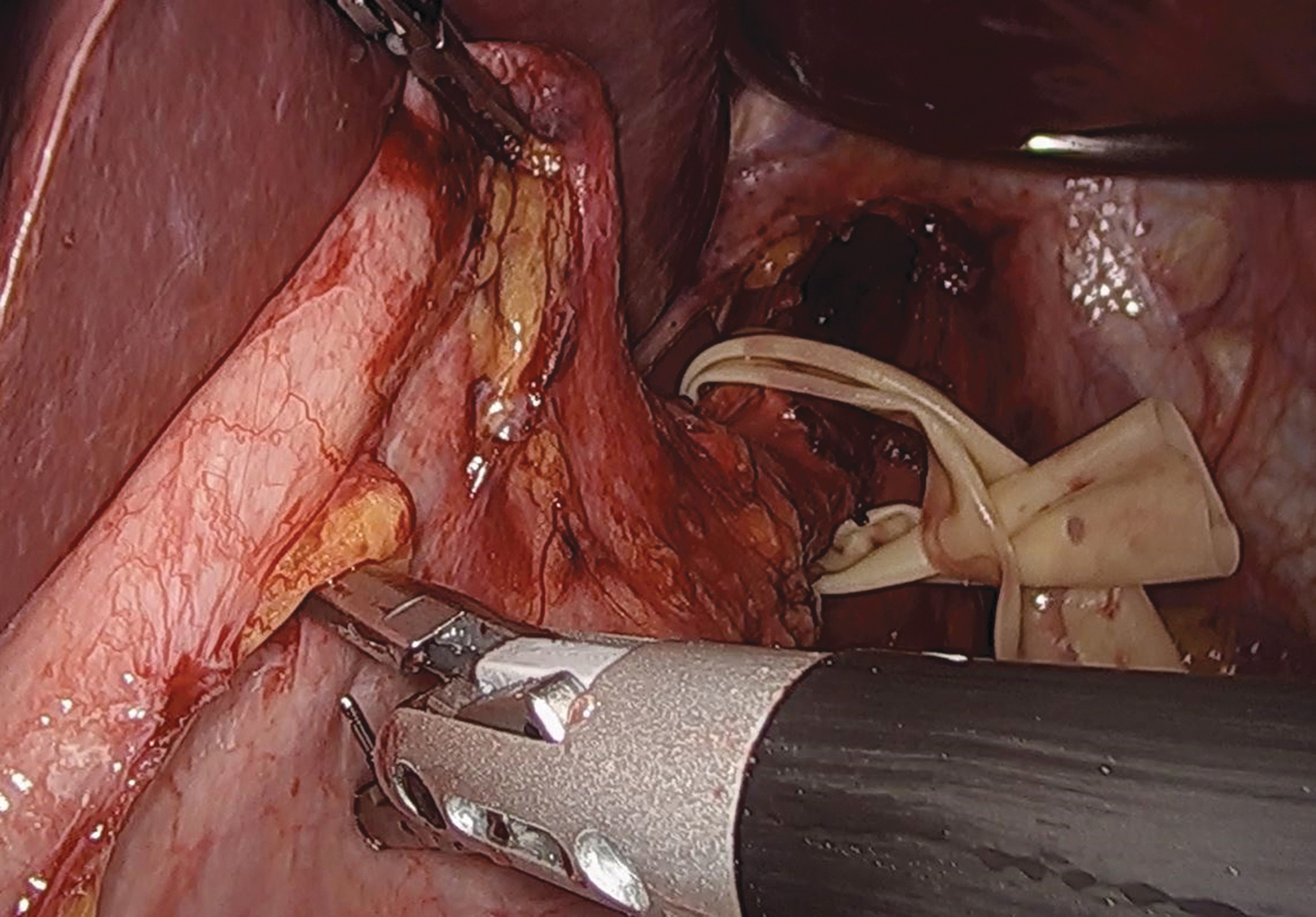
Placement of a posterior fundal stay stitch 3 cm distal to the GEJ and 2 cm from the greater curve of the stomach. GEJ, gastroesophageal junction.
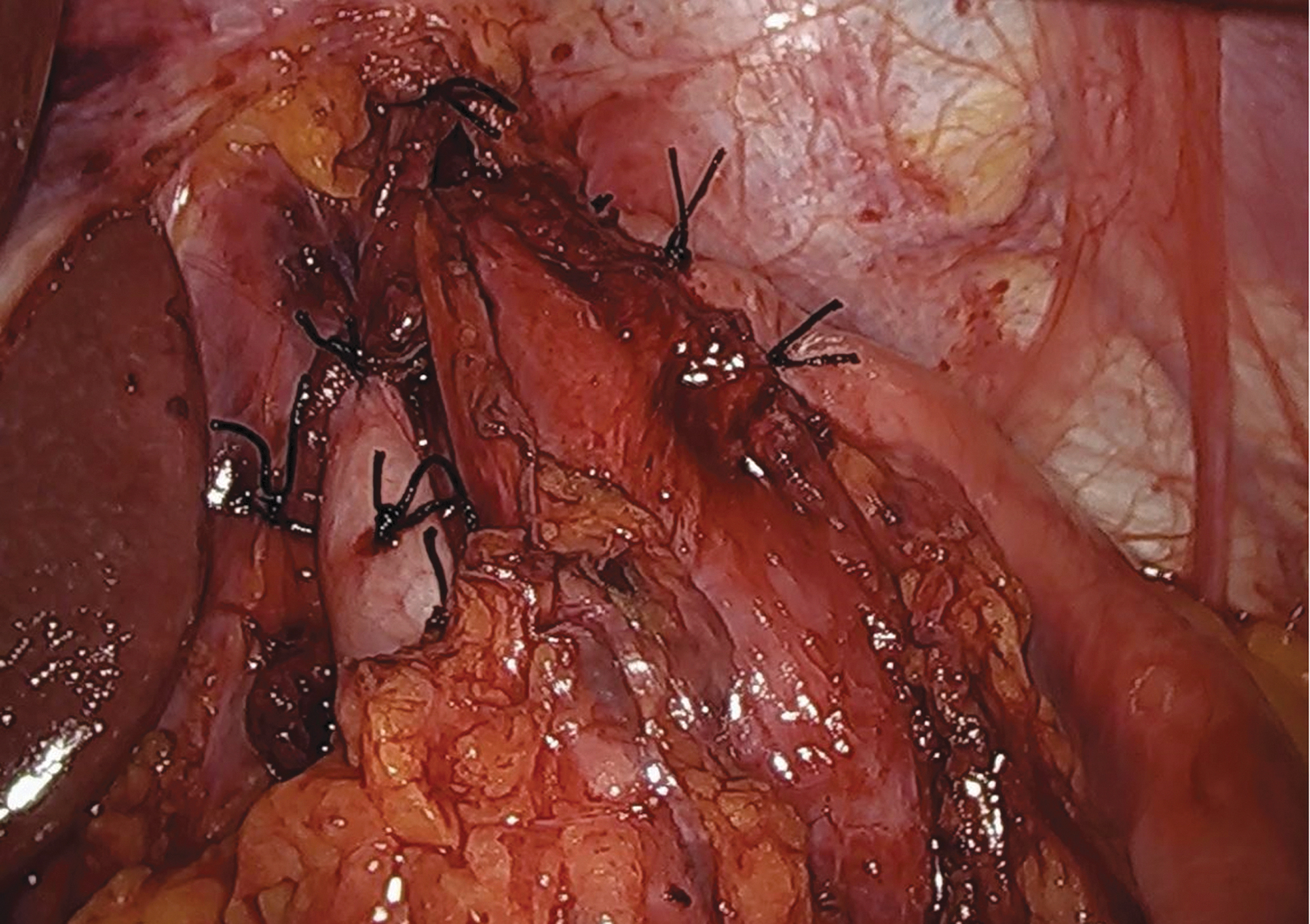
Toupet fundoplication.
Upper endoscopy
Before desufflating the abdomen, we perform an upper endoscopy to ensure there is no obstruction from the fundoplication and that the fundoplication itself appears symmetrical. At the same time, water is poured over the myotomy to ensure there is no leak from inadvertent injury to the exposed esophageal mucosa.
Postoperative care pathway
Postoperatively, patients are started on a clear liquid diet and encouraged to get out of bed and ambulate. They are given scheduled liquid acetaminophen a round the clock and crushed oxycodone and ibuprofen as needed for pain. They are monitored overnight and advance to a full liquid diet the next morning as tolerated. All patients are seen by a dietician before discharge to review details of the soft esophageal diet they will maintain for the next 4 weeks. Patients are typically discharged postoperative day 1 and seen for follow-up within 2–3 weeks after surgery. Because of the high incidence of silent reflux, even with fundoplication, we ask all patients to return at 6 months for pH testing.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding statement was provided.