
Abstract
Over the past decade, per-oral endoscopic myotomy has been shown to be a durable minimally invasive approach to the treatment of esophageal achalasia. Patients with suspected achalasia should undergo upper endoscopy, timed barium esophagram, and high-resolution manometry to confirm the diagnosis. The procedure includes several key steps including mucosotomy, submucosal tunneling, selective myotomy of the circular muscle layer, and mucosotomy closure. Specialized endoscopic dissection tools are used during the procedure to access the submucosal space. Common procedural challenges include minor bleeding and capnoperitoneum.
Introduction
Achalasia is a rare disease affecting esophageal motility that leads to a functional obstruction of the esophagus at the lower esophageal sphincter. 1 This causes affected patients significant symptoms including chest pain, dysphagia, regurgitation, and weight loss. 2 Treatments aim to relieve this obstruction by relaxation, stretch, or disruption of the lower esophageal sphincter through Botox injection, mechanical dilation, or myotomy. Myotomy, either by the laparoscopic or endoscopic approach, has been shown to have the most durable palliative outcome.3–5
Per-oral endoscopic myotomy (POEM) for esophageal achalasia has been performed over the past decade and was recently shown to be noninferior to laparoscopic Heller myotomy in a randomized controlled trial. 6 POEM is an advanced endoscopic procedure that uses the submucosal space to access and selectively cut the circular muscle layer of the esophagus. POEM combines the advantages of the incisionless approach of endoscopy with the durability of surgical myotomy, making this procedure the ideal approach for effective treatment of achalasia. This article discusses our institutional approach to performance of POEM for esophageal achalasia.
Patient Evaluation and Selection
Given the rarity of achalasia, patients should be seen at specialized, high-volume centers that evaluate and treat patients with disorders of esophageal motility to ensure proper diagnosis. When considering treatment of a patient with achalasia by POEM, a thorough review of the patient's symptoms and workup must be carried out. Our institution uses a multidisciplinary approach to the review and discussion of patients, many of whom have had previous interventions, to select the appropriate treatment.
Patient History and Symptom Evaluation
A complete history and physical examination should be performed on all patients in the preoperative setting. Focus should be on symptoms characteristic of achalasia, history of previous interventions, and previous abdominal surgeries. We use the Eckardt score as a measure of clinical severity preoperatively, which ranges from 0 to 12, with 12 representing the most severe symptoms. This grading system focuses on the four most common symptoms of achalasia: regurgitation, dysphagia, weight loss, and chest pain. The Eckardt score is also frequently assessed postoperatively as a measure of clinical treatment effectiveness with scores ≤3 being considered clinically successful.
Patients who have undergone previous interventions such as dilation or Botox injection may have scar tissue that can make submucosal tunneling more difficult. Previous endoscopic or surgical myotomy also results in scar tissue that should be avoided by planning an alternate location for subsequent myotomy. If these procedures were performed at outside institutions, it is important to obtain and review operative reports to have a clear understanding of previous myotomy location.
Imaging and Diagnostic Testing
Physiologic studies and endoscopic evaluation are imperative in the workup of suspected achalasia to rule out other potential etiologies that may mimic achalasia symptomatology. Such pathology includes but is not limited to severe gastroesophageal reflux disease (GERD), peptic stricture, obstructing tumors, or other mechanical obstruction (pseudo-achalasia). Upper endoscopy is often the first step toward identifying these other etiologies through direct visualization and biopsy, if indicated. Patients where endoscopy is unrevealing of an alternative diagnosis should undergo high-resolution manometry (HRM) to evaluate esophageal contractility and lower esophageal sphincter tone. Based on results from HRM, a diagnosis of achalasia type according to the Chicago Classification v3.0 can be determined. Finally, a timed barium esophagram (TBE) is useful for anatomical evaluation preoperatively in addition to providing another measure of esophageal physiology that can be repeated postoperatively to evaluate physiologic success.
Anatomical considerations include detection of a hiatal hernia on endoscopy or esophagram as this would predispose patients to increased risk of GERD post-POEM. A particularly tortuous or angulated esophagus should be avoided from an endoscopic approach given the increased challenge to creating a submucosal tunnel. A laparoscopic approach to myotomy is minimally challenged by a tortuous or angulated esophagus and also allows for simultaneous hiatal hernia repair and anti-reflux procedure, reducing the risk of postmyotomy GERD.
Operative Technique
POEM is an incisionless approach to selective myotomy of the circular muscle layer of the esophagus to treat achalasia. The procedure uses several common interventional endoscopic techniques including submucosal lift and endoscopic submucosal dissection for the creation of a submucosal tunnel. The procedure is performed entirely in the small working area of the submucosal space, making it technically challenging even for advanced endoscopists. POEM has a technical learning curve that is described by several experienced POEM centers.7–10 It is therefore highly recommended that new practitioners enlist an experienced proctor to assist with early cases. The following describes our standard perioperative care and detailed technical steps of POEM, as performed at our institution.
Preparation for procedure
Our practice is to prescribe a 7-day course of oral fluconazole before the procedure given the significant esophageal retention and stasis places these patients at higher risk for candidiasis. Patients are instructed to adhere to a clear liquid diet 2 days before the procedure and standard nil per os at midnight to minimize the burden of retained food in the esophagus. In addition, proper communication with the anesthesia team is important including a plan for management of the high aspiration risk (rapid sequence intubation, cricoid pressure). We also require strict blood pressure control to avoid engorgement of the delicate submucosal vessels with a preference for the systolic blood pressure to be maintained ≤120 mmHg for the duration of the procedure.
Patients are placed in the supine position for a standard anterior myotomy and lazy left lateral decubitus position for a posterior myotomy (in the case of previous anterior myotomy). The abdomen is prepped and draped in preparation for Veress needle decompression of capnoperitoneum if needed during the case. Knowledge of previous abdominal interventions should be taken into consideration to determine best placement of Veress needle, if required. Once anesthesia has successfully secured an endotracheal airway, the operating table is moved slightly away from the ventilator and angled to allow for increased space at the head of the bed. An assistant is on either side of the surgeon, one to keep the endotracheal tube from inadvertent dislodgement and to maintain torque on the endoscope when needed, and the other to assist with instrument exchange. The endoscopy tower is placed directly adjacent to the operating room table at the level of the patient's abdomen.
Endoscopy
Before beginning a POEM, a diagnostic endoscopy is performed to assess clearance of the esophagus and evaluate for candidiasis. A standard high-definition endoscope is used with carbon dioxide insufflation to prevent hemodynamic compromise in the event of mediastinal or peritoneal cavity entrance. If significant retained food is discovered, several strategies are used to adequately clear the esophagus. Liberal flushing with bacitracin and saline solution works with mostly liquid debris and small sediment. For larger food debris, using the endoscope with the transparent dissecting cap at the end to push the debris into the stomach is an option, or utilizing endoscopic nets for retrieval and removal is an alternate option.
Once clear, find the squamocolumnar junction and use the shaft of the endoscope to measure the location of esophagogastric junction (EGJ) in relation to the incisors. This measurement is used to determine the location of the mucosotomy as well as the starting point and extent of myotomy, which will be described in detail during subsequent steps.
Submucosal injection and mucosotomy
The location for mucosotomy and initiation of submucosal tunneling should be identified 4–6 cm proximal to the start of the planned myotomy. Our practice is to perform an 8–10 cm myotomy that includes a 2–3 cm extension onto the stomach. For our standard myotomy, the location of the mucosotomy is 12 cm proximal to EGJ as measured by the location of the squamocolumnar junction during endoscopy. Once we have identified the location for mucosotomy, we begin by submucosal injection of dilute indigocarmine (20 mg/100 cc solution without epinephrine) to create a bleb that lifts the mucosal layer off the underlying muscle allowing for entrance into the submucosal space (Fig. 1A).
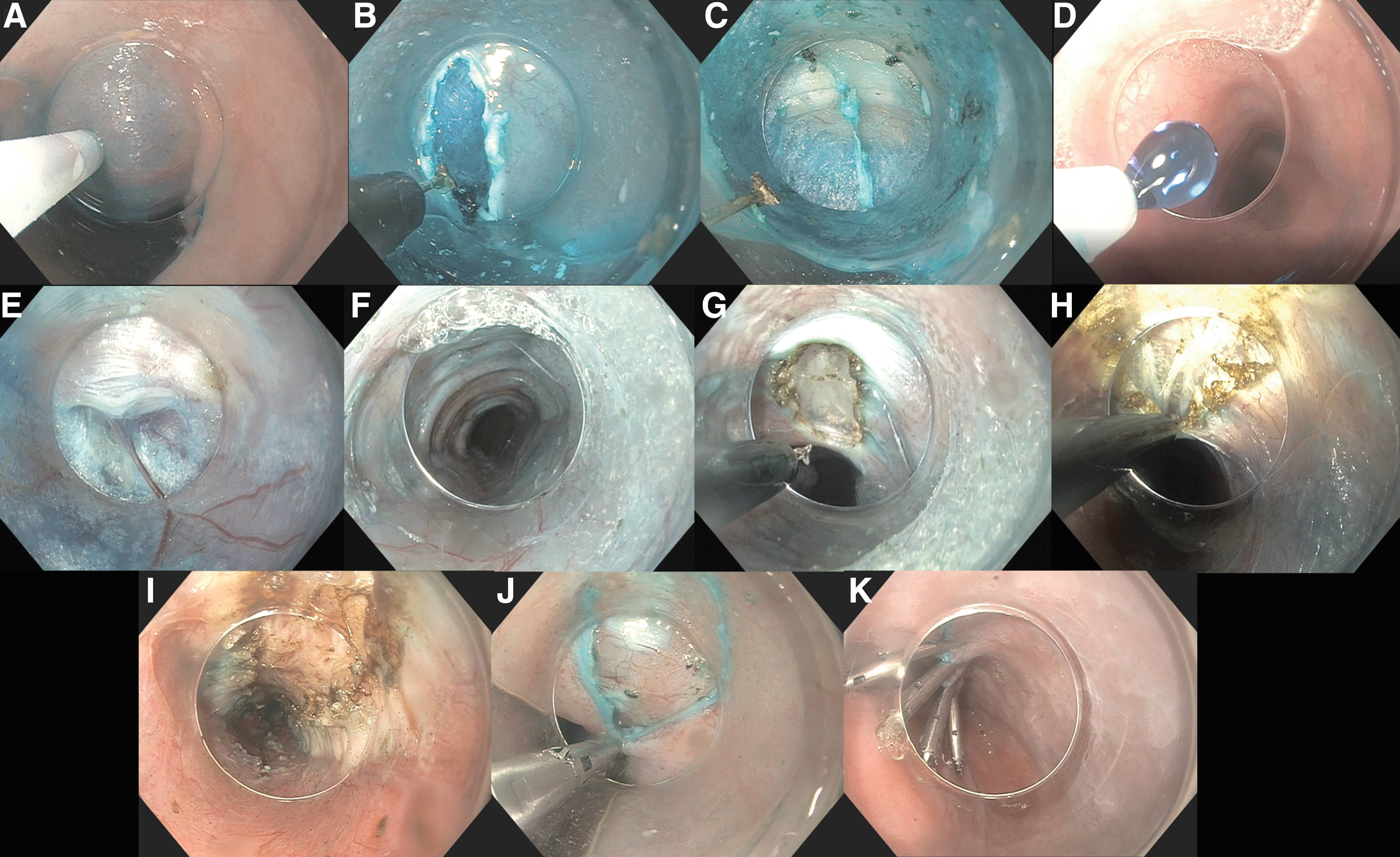
Endoscopic images of the steps of per-oral endoscopic myotomy for esophageal achalasia.
Next, we use the triangle tip electrosurgical knife (using “cut” current) to perform the mucosotomy. The mucosotomy should be longitudinal and 1–2 cm to allow for entrance of the dissecting cap and endoscope (Fig. 1B). After completion of the mucosotomy, we proceed with dissection of fibers (set to “spray coag”) that connect the mucosa to the muscle before attempting entrance into the submucosal space, which allows for easier scope entry in the submucosal space and reduces distal tearing of the mucosotomy.
Submucosal dissection and tunneling
The beveled edge of the transparent dissecting cap should face up for ease of entering into the submucosal space and to properly place fibers on stretch (Fig. 1C). If difficulty is encountered when trying to enter the submucosal space, confirm the correct orientation of the cap on the endoscope, and try dissecting more of the fibers connecting the mucosal flap to the underlying muscle to make room for the endoscope. Once successfully in the submucosal space, proceed with dissection using the triangle tip electrosurgical knife (set to spray coag). Keep the muscle anterior (or superior on the screen) and the mucosal flap posterior (or inferior on the screen) at all times to maintain orientation. To avoid spiraling, assess endoscope position by dripping injection fluid to see the direction of flow and pooling. For a standard anterior myotomy, the fluid should pool posteriorly or inferiorly on the screen. For posterior myotomy, the patient is positioned in a lazy left lateral decubitus position, so the fluid should pool superiorly and to the right on the screen (Fig. 1D).
To prevent inadvertent injury to the mucosa, dissect right on the circular muscle layer and maintain the mucosal flap inferiorly at all times. As the dissection progresses distally, additional injections along the submucosal tunnel are helpful to lift the mucosa off the muscle. This injection is performed while the endoscope is in the tunnel. We advance the injection tool into the submucosal space while keeping the needle retracted. If there is concern that the dissection tunnel is off course, an additional orientation task includes removal of the endoscope from the tunnel and inspecting the path of blue dye. The submucosal tunnel should extend ∼3 cm onto the stomach. The EGJ can be identified as a narrowing during tunneling that limits dissection space and, as a result, is the most common location for mucosal injury. If it becomes difficult to dissect across the EGJ, exit the tunnel, and decompress the stomach. A distended stomach accentuates the angle of His, which can make tunneling across the EGJ especially challenging. Once across the EGJ the tunnel will widen again, and the blood vessels and muscle fibers will appear more disorganized. Confirmation of tunnel length can also be based on comparison with predissection endoscopic measurements.
During dissection you may encounter several larger appearing blood vessels that are best cauterized using a coagulation grasper (Fig. 1E). If blood pressure becomes too high, it is best to avoid proceeding until appropriate control has been obtained as the small working space of the submucosal tunnel is easily obscured by even small amounts of bleeding. You may also notice abdominal distension during the procedure indicating capnoperitoneum. It is important to assess for and recognize this common occurrence periodically during the procedure. Placing a Veress needle for decompression is a simple and effective treatment, but it is important to first decompress the stomach to make sure massive gastric distension is not mimicking capnoperitoneum.
Myotomy
The standard myotomy is 8–10 cm in length extending 2–3 cm on to the stomach. We typically begin proximally and proceed distally using the triangle tip knife. We do not typically encounter significant vessels during myotomy; however, these are managed in a similar manner to vessels encountered during tunneling. Selectively cut the circular fibers leaving the longitudinal layer intact, although often this layer is thin and the fibers may splay (Fig. 1H). Inspect the myotomy length and completeness by comparing with predissection measurements and re-examining along the length of the myotomy for any area with remnant muscle fibers. We cauterize remnant bands that appear to hold the edges of the myotomy together or use the scope to apply slight lateral traction to avulse small fibers. At the completion of the myotomy, assess the tunnel for hemostasis. Irrigate the tunnel with bacitracin solution and prepare for mucosotomy closure.
Closure
Closure of the mucosotomy can be effectively completed with clips. We begin closure at the distal end of the mucosotomy. We attempt to precisely appose the mucosal edges, avoiding overlap (Fig. 1J). Occasionally, lining up the open clip where placement is desired and suctioning on the scope will pull the desired tissue into the clip. We typically use between 4 and 6 clips for complete mucosotomy closure. We assess the closure by driving the scope past and slowly pulling back to visualize each clip placement and the space between clips (Fig. 1K). If necessary, additional clips are placed.
Postoperative Care
Our practice is to admit patients for observation post-procedure. They are advanced to clear liquids if not suffering from nausea on postoperative evaluation. All patients are discharged on a proton pump inhibitor for 6 months following POEM and then return for formal pH testing. Most patients are discharged on postoperative day 1, although some patients feel well enough to leave the evening of postoperative day 0. Water-soluble esophagram is reserved for patients who have dysphagia, more pain then expected or if mucosal closure was challenging. Patients return for a typical postoperative clinic visit at 2–4 weeks to assess recovery. The next follow-up visit is at 6 months where symptom evaluation (Eckardt score) and physiologic studies (endoscopy, HRM, TBE, and pH testing) are performed.
Conclusions
POEM for esophageal achalasia is an advanced endoscopic procedure that should be performed by trained endoscopists at high-volume centers. With the proper tools, technique, and training, POEM is a very safe and effective treatment for esophageal achalasia.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.