
Abstract
Surgical treatment of gastroesophageal reflux disease (GERD) aims to control patients' symptoms, improve patients' quality of life, and prevent GERD-related complications (bleeding, esophageal stenosis, Barrett's esophagus, and/or esophageal adenocarcinoma). A careful patient selection and a properly executed operation are key for the success of the procedure. We aimed to describe the operative technique of a laparoscopic Nissen fundoplication, stressing the critical surgical steps we believe should be respected to obtain good surgical outcomes.
Introduction
Gastroesophageal reflux disease (GERD) prevalence is increasing around the world, especially in developed countries. In the United States, it is estimated that ∼20% of the adult population is affected by this disease, with increasing incidence rates in the past decades mostly due to the obesity epidemic. 1 Medical expenditures related to GERD are alarming, with direct health care costs of ∼$10 billion per year (medical therapy being the largest contributor to these expenses).2,3
Although most patients affected by GERD will adequately respond to lifestyle modifications and medical therapy (proton pump inhibitors), some will require an antireflux operation: partial control of symptoms (e.g., regurgitation or cough) with medication, presence of large hiatal hernia, poor patients' compliance with medical therapy, refusal to be on long-term medical treatment, or complications related to medication. 4
Surgical treatment of GERD aims to control patients' symptoms, improve patients' quality of life, and prevent GERD-related complications (bleeding, esophageal stenosis, Barrett's esophagus, and/or esophageal adenocarcinoma). To achieve these objectives, patients must be evaluated and treated by surgeons with vast experience in gastroesophageal disorders because a careful patient selection and a properly executed operation are key for the success of the procedure.5–7
We aimed to describe the operative technique of a laparoscopic Nissen fundoplication, stressing the critical surgical steps we believe should be respected to obtain good surgical outcomes.
Preoperative Phase
After induction of general endotracheal anesthesia, an orogastric tube is inserted to keep the stomach decompressed. The patient is positioned supine in low lithotomy position over an inflated beanbag with the lower extremities extended on stirrups, with knees flexed 20°–30°. Pneumatic compression stockings are used to reduce the risk of deep vein thrombosis. The surgeon stands between the patient's legs, and the first and second assistants on the left and right sides of the operating table, respectively.
Ports placement
Five 10 mm ports are used for the operation. Port 1 is placed in the midline or slightly to the left ∼14 cm below the xiphoid process. This port is used for insertion of the 30° scope. Ports 2 and 3 are placed ∼2 cm below the right and left costal margins (forming an angle of ∼120°). Port 4 is placed at the level of port 1 in the right midclavicular line (this is used for the liver retractor) and port 5 is placed at the level of port 1 in the left midclavicular line (Fig. 1).
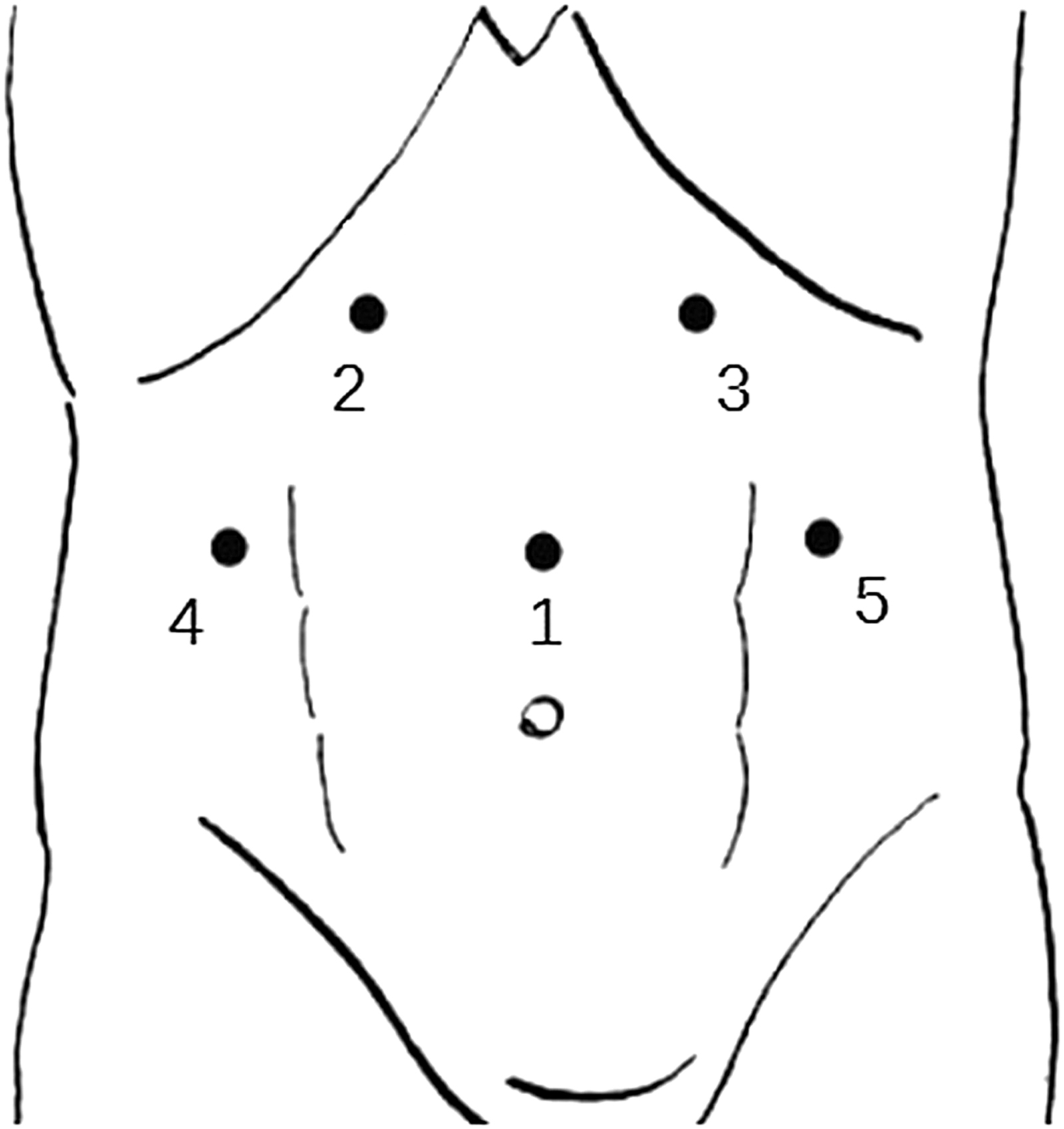
Placement of abdominal ports.
Division of gastrohepatic ligament
Once the left segment of the liver is retracted, the gastrohepatic ligament is divided starting above the caudate lobe of the liver toward the right crus. The crus is then separated from the right side of the esophagus by blunt dissection and the posterior vagus nerve is identified. The right crus should be dissected all the way down toward the junction with the left crus (Fig. 2).
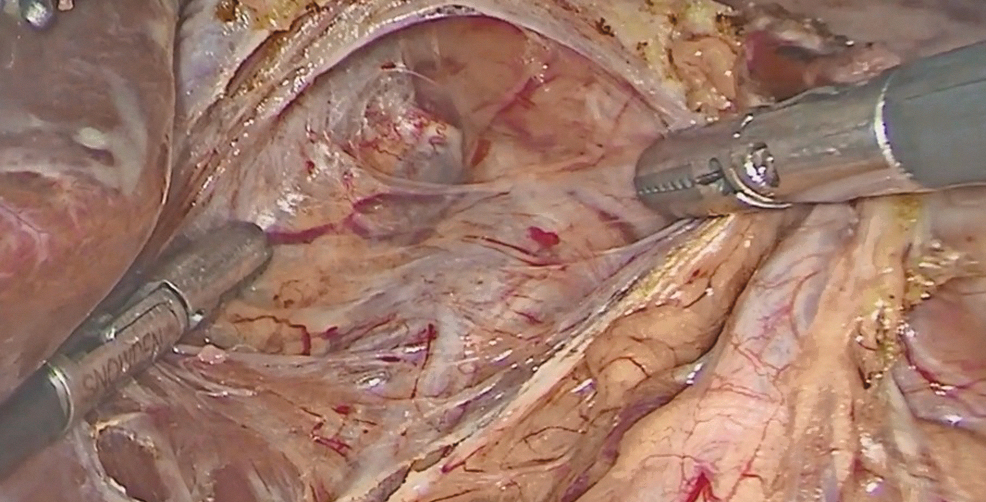
Dissection of the right pillar of the crus.
Division of phrenoesophageal membrane
The phrenoesophageal membrane is incised and divided with electrocautery above the esophagus. The anterior vagus is identified and left attached to the esophageal wall. The left pillar of the crus is separated from the esophagus and dissected bluntly downward toward the junction with the right crus (Figs. 3 and 4).

Division of the phrenoesophageal membrane.
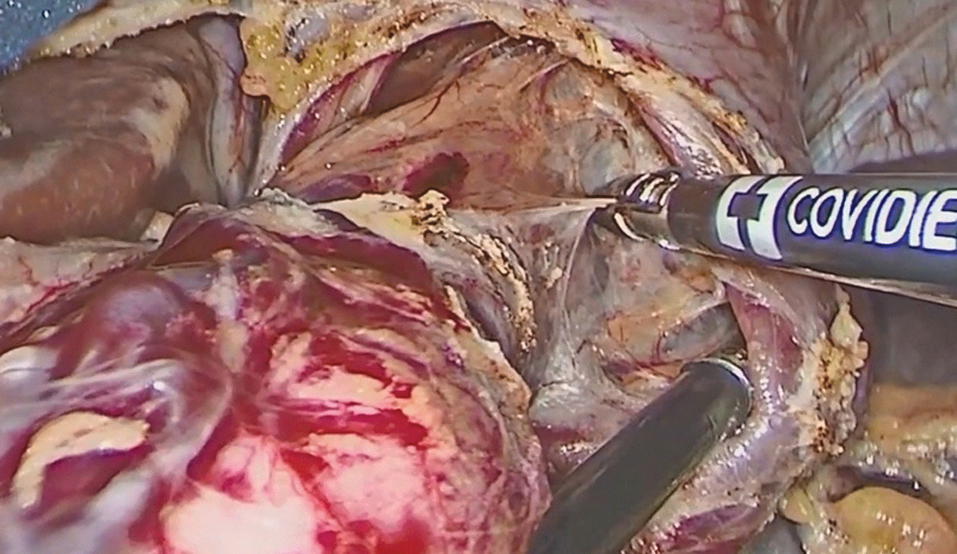
Dissection of the left pillar of the crus.
Division of short gastric vessels
Starting from a point midway along the greater curvature of the stomach, the short gastric vessels are taken down with a vessel sealing system toward the fundus and all the way to the left pillar of the crus. The division of these vessels will ensure a tension-free wrap. Excessive traction of the short gastric branches should be avoided to prevent bleeding from the spleen (Fig. 5).

Division of short gastric vessels.
Esophageal mobilization and mediastinal dissection
The esophagus is retracted upward using a Babcock clamp applied at the level of the gastroesophageal junction, and a window under the esophagus is opened by blunt dissection. A Penrose drain is then passed around the esophagus, incorporating both anterior and posterior vagus nerves. The Penrose drain should be secured with a large clip or a loop suture tie and will be used to provide adequate and safe traction on the esophagus. The dissection should be carried up into the mediastinum until at least 3 cm of esophagus comes into the abdomen without tension.
Closure of the crura
Appropriate exposure is obtained retracting the esophagus upward and toward the patient's left with the Penrose drain. Crural closure is done with interrupted nonabsorbable sutures (2-0 silk or polyester). The first stitch should be placed just above the junction of the two pillars. Additional stitches are placed 1 cm apart, and a space of ∼1 cm should be left between the uppermost stitch and the esophagus. The crura should not be too tight, and a close grasper should slide easily between the esophagus and the crura (Fig. 6).
Closure of the crura.
Nissen fundoplication
Before starting the fundoplication, a bougie should be inserted into the esophagus to (performing a fundoplication without a bougie in the esophagus significantly increases the risk of postoperative dysphagia). The orogastric tube is removed, and the anesthesiologist inserts a 56F bougie down the esophagus through the esophagogastric junction. The bougie should be properly lubricated and the anesthesiologist should advance it slowly to avoid an esophageal perforation.
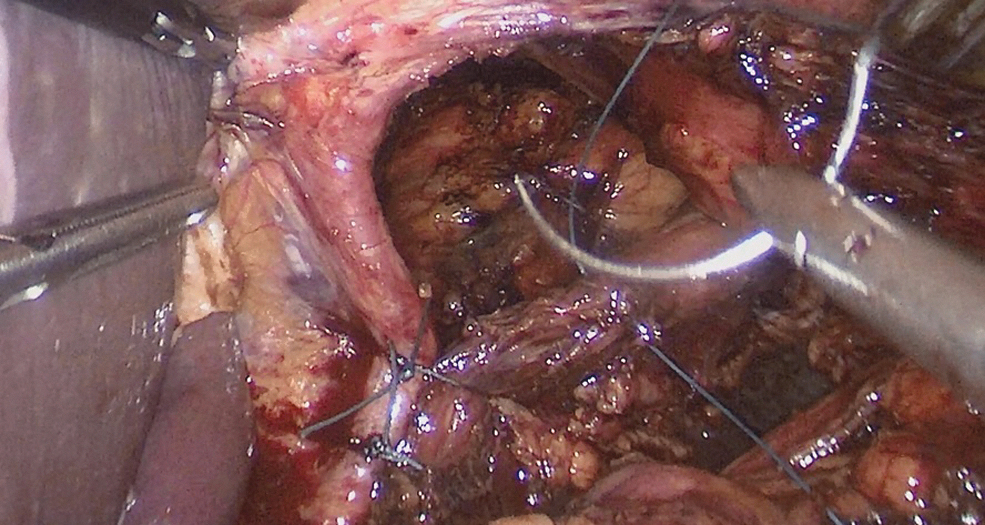
The stomach is passed behind the esophagus and a “shoe-shine” maneuver is performed to verify sufficient fundic mobilization and to avoid having part of the gastric fundus above the wrap. The Nissen fundoplication is a total 360° fundoplication: the gastric fundus is pulled under the esophagus, and the left and right sides of the fundus are wrapped with a Babcock above the esophagogastric junction during the placement of the first stitch. We use three stitches of nonabsorbable material (2-0 silk or polyester) at 1 cm intervals to approximate the right and left sides of the fundoplication. The goal is to create a short (∼2 cm in length) and floppy wrap (Fig. 7).

Nissen fundoplication.
Final inspection
The bougie is removed from the esophagus and the Penrose drain is cut and passed out of the abdomen. After hemostasis is achieved, the liver retractor, instruments, and the trocars are removed from the abdomen under direct vision. All the port sites should be closed.
Postoperative Course
Patients are fed the morning of the first postoperative day with clear liquids and then soft diet. Most patients are discharged within 48 hours and resume their regular activities within 2 weeks. Acid-reducing medications should be discontinued after 6 weeks at the latest.
Mild dysphagia is very common, and patients are instructed to eat soft diet until symptoms resolve. Persistent dysphagia >6 weeks is rare, and it should raise concern for a technical problem (tight closure of the crura, tight or long wrap, or wrap made with the body of the stomach rather than the fundus).
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.