
Abstract
Objective:
To compare the surgical feasibility, oncological and functional results between sutureless and suture techniques in retroperitoneal laparoscopic nephron-sparing surgery (LNSS).
Materials and Methods:
This retrospective study collected consecutive patients with a renal mass who underwent retroperitoneal LNSS in two high-volume centers. Propensity score matching (PSM) analysis was conducted to select two baseline homogeneous cohorts. Descriptive statistics was performed both before and after PSM. Moreover, univariate and multivariate logistic analyses were carried out to identify the risk factors of postoperative acute kidney injury (AKI), whereas Kaplan
Results:
After PSM at a ratio of 1:3, the sutureless group (n = 65) was compared with the suture group (n = 152) with no remaining statistically significant differences in baseline characteristics. With regard to patient outcomes, differences in warm ischemia time (WIT) (P < .001), estimated blood loss (P < .001), AKI (P = .002), length of hospital stay (P = .020), and eGFR at discharge (P < .001) were statistically significant. Meanwhile, the postoperative complication rates (9.2% versus 13.8%, P = .378) and positive surgical margins (0% versus 2.0%, P = .556) were not statistically different. At the last follow-up, the eGFR decline percent was the same (−1.5% versus −2.2%, P = .192). No difference was detected on Kaplan
Conclusions:
Sutureless technique in LNSS is safe and feasible, compared with the traditional suture method, with shorter WIT, lower AKI rate, and comparable long-term oncological and functional outcomes.
Introduction
It is the standard of care that a renal mass should be managed with nephron-sparing surgery (NSS) whenever feasible. Minimal invasive approaches are currently the predominant choices with potentially lower complication rates, faster recovery time, and comparable oncologic control. 1
Usually, during tumor excision and defect reconstruction, the on-clamp technique is utilized to temporarily occlude blood supply for better margin visualization. Thus, ischemia
In a traditional fashion, both suturing and knotting steps can be time-consuming and challenging. Hence, several different sutureless techniques have been innovated and they exhibited potentially superior functional preservation capacities.4–12 Among them, mono-polar has attracted extensive interests due to its low cost, easy-to-master characteristic, and considerable safety.5,6,8,11 However, most reports on the sutureless technique are only single-arm studies or those with non-comparable baseline characteristics. Moreover, little is known regarding the sutureless fashion compared with the conventional knot-tying method in NSS. Typically, the propensity score matching (PSM) analysis is a widely accepted method for homogeneous comparison in a retrospective controlled study.
This study aimed at comparing the sutureless technique with the conventional suture method after PSM, so as to assess their comparative effectiveness in terms of safety, long-term oncological and functional outcomes.
Materials and Methods
Patient selection
Our study protocol was approved by the Institutional Review Board of the local ethical committee and registered on Chinese Clinical Trial Registry (Registration No.: ChiCTR2000031084). Informed consent was obtained from all participants.
From January 2014, when a prospectively maintained electronic database was first established, to September 2019, patients with single-sited and ipsilateral lesion who underwent retroperitoneal laparoscopic nephron-sparing surgery (LNSS) were retrospectively reviewed in this study. Patients undergoing surgery by the suture or sutureless technique were identified, whereas those with multiple masses and who received the transperitoneal approach surgery were excluded. All procedures were completed by two senior urologists (Prof. C. Ge and Prof. D. Wang). The inclusion criteria were as follows: patients with a tumor diameter of ≤4 cm, predominant exophytic growth, and a RENAL score of ≤7 with item N 1–2. Tumors were resected with cold scissors, and the tumor bed was coagulated or cauterized with a mono-polar hook as described by Simone et al. 8 Hemostatic agents were placed on the tumor bed at the surgeons' discretion in both groups.
Data collection
The following information was collected from the hospital electronic databases: demographic data (age, gender, and body mass index [BMI]), tumor information (lesion location, diameter, and RENAL score), surgery information (operation time, warm ischemia time [WIT], estimated blood loss [EBL], and conversion to nephrectomy), and postoperative outcomes (complications defined according to the Clavien-Dindo classification and length of hospital stay). Renal functional decline included percent change and acute kidney injury (AKI) defined by the RIFLE criteria 13 at discharge. Renal functional deterioration was defined as a new-onset stage 3 chronic kidney disease (CKD), estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2, or CKD upstaging after surgery during the 3–57 months of follow-up (median, 22 months).
Statistical analysis
A 1:3 PSM analysis was conducted to minimize the selected bias between the two groups (the baseline characteristics were age, gender, BMI, lesion location, ASA grade, baseline eGFR, CKD rate, RENAL score, tumor diameter, and endophytic percent). All data were presented as mean ± standard deviation or medians with interquartile ranges for continuous variables, and percent frequency for categorical variables, respectively. Categorical variables were analyzed by the Fisher's exact tests, whereas continuous variables were compared by Wilcoxon tests both before and after PSM. Univariate and multivariate logistic regressions were applied in identifying the risk factors that affected AKI. Kaplan–Meier analysis and log-rank test were conducted after PSM to compare the functional deterioration between two groups. The STATA 15.1® (Stata Corp., College Station, TX) and GraphPad Prism 8.0® (GraphPad Software, Inc., San Diego, CA) were employed for statistical analysis. A difference of P < .05 (two-sided) indicated statistical significance.
Results
Patient- and tumor-related characteristics
The patient- and tumor-related characteristics both before and after PSM are summarized in Table 1. After PSM, a total of 217 patients (including 65 from the sutureless group and 152 from the suture group) were included, and the baseline variables, including tumor size (P = .602), RENAL score (P = .450), BMI (P = .568), and baseline eGFR (P = .730), were all homogenous. Malignancy accounted for 88.9% in the final pathology, among which renal cell carcinoma constituted 83.6%.
Baseline Patients' Characteristics Before and After Propensity Score Matching
P < .05.
ASA, American Society of Anesthesiologists; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; PSM, propensity score matching.
Operation-related outcomes
In PSM analysis, variables remained significantly different in relation to WIT (P < .001), AKI rate (P = .002), length of hospital stay (P = .020), and eGFR at discharge (P < .001). The long-term eGFR decrease between two cohorts was comparable during the median follow-up of 22 months (−1.5% versus −2.2%, P = .192) (Table 2). Kaplan
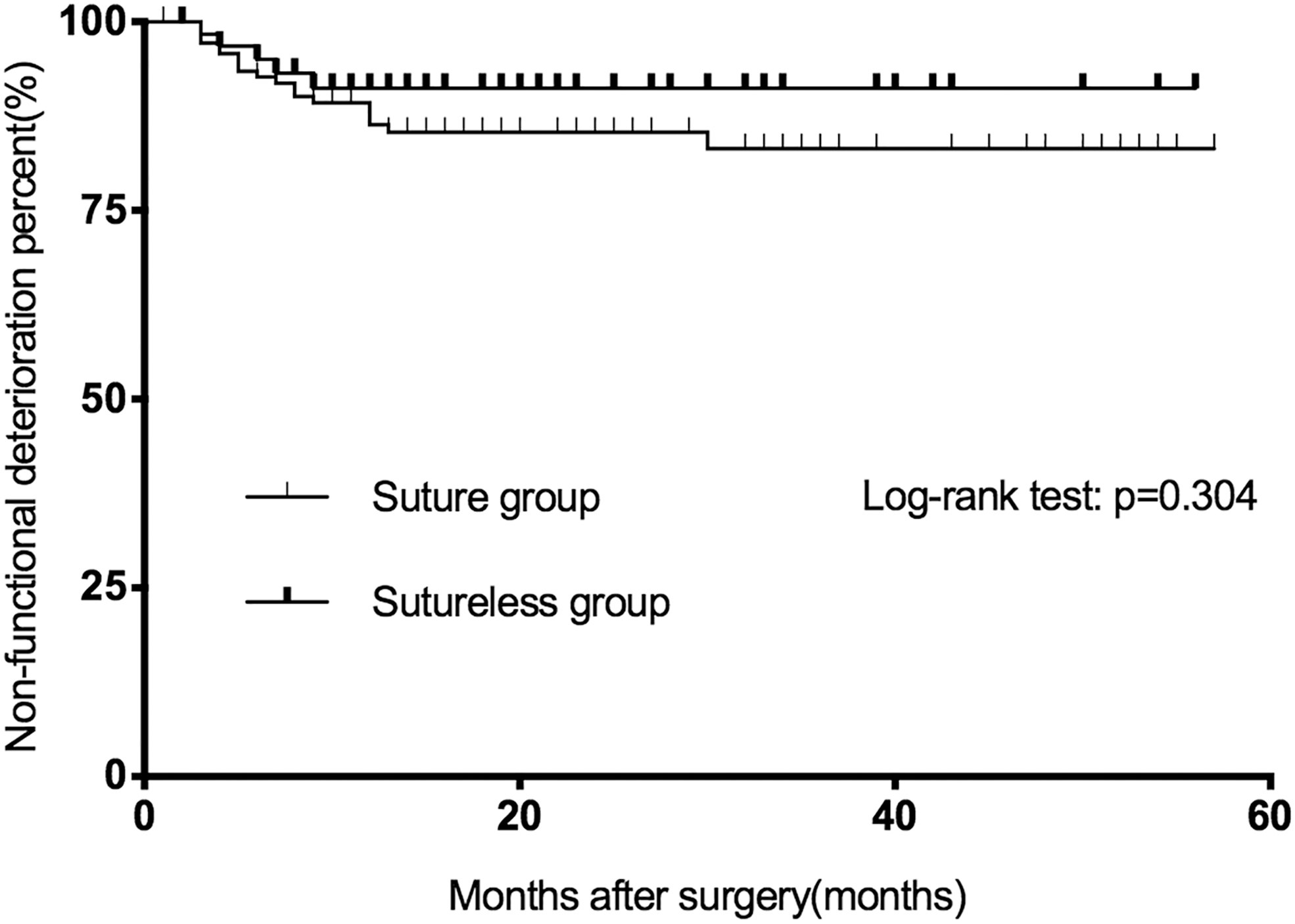
Kaplan–Meier analysis that compares the risk of developing a new-onset stage 3a CKD or CKD upstaging during follow-up between the propensity score matching cohorts. CKD, chronic kidney disease.
Surgical Outcomes Before and After Propensity Score Matching
P < 0.05.
EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; OT, operation time; PSM, propensity score matching; WIT, warm ischemia time.
In the sutureless group, 2 cases experienced bleeding and received endo-embolism (Table 2). No tumor recurrence was detected in the sutureless group (disease-free survival [DFS], 100%), whereas in the suture group, 2 patients were identified with ipsilateral recurrence and underwent radical surgery (DFS, 98.7%). In Tables 3 and 4, factors were identified as the risk factors of AKI. Moreover, the suture group had a 5.75-fold (odds ratio 5.75, 95% confidence interval 1.20–27.53, P = .029) increased risk of AKI compared with the sutureless group at discharge. One patient needed suturing to ensure complete hemostasis.
Univariable and Multivariable Logistic Regression Analyses to Identify Predictors of Acute Kidney Injury
CI, confidence interval; eGFR, estimated glomerular filtration rate; OR, odds ratio; WIT, warm ischemia time.
Characteristics of Sutureless Versus Suture Technique in Off-Clamp Subgroup After Propensity Score Matching
P < 0.05.
EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; OT, operation time.
Discussion
Over the past decade, the refinements of surgical techniques for eliminating suturing, such as bipolar,4,7 mono-polar hook5,8 or scissors,6,11 vessel-sealing devices, 8 ultrasound scalpel, 11 fibrin gel, 12 laser, microwave, and radiofrequency, have been reported (Table 5). However, most reports are limited by their single-arm design5,6,8–11 or potentially heterogeneous baseline characteristics compared with those of the suture technique, ranging from tumor size and complexity to endophytic depth.4,7 These features may have a profound impact on the surgical outcomes. In our database, all baseline information between the two groups was comparable after pairing all known influencing factors by PSM.
Studies Reporting About Sutureless Techniques
NA, not available.
The concerns of safety and therapeutic effectiveness have been raised for the sutureless technique. In our study, both positive surgical margin and postoperative complications were identified to be the same after PSM (P > .05). Meanwhile, the postoperative complication rate was 9.2%, which was equivalent to that obtained after suture LNSS (9.2% versus 13.8%, P = .378) and those reported for the sutureless techniques7–9,12 (0%–10.4%). Minervini et al. 4 reported that tumor complexity and WIT were the significant risk factors affecting postoperative complications identified in multivariate analysis. Further, the inclusion criteria vary substantially among previous studies, and most patients have small renal masses (diameter ≤4 or ≤2.5 cm) with a low RENAL score (≤6 or 7) due to the limits of the technique characteristics. This may explain the low complication rate in most literature. Apart from complications, in the sutureless group, no one was identified with a positive surgical margin in the final pathology. The positive margin rate reported in literature is low, with a rate of 1.4%–5.3%.5,9,10,12
The goal of NSS is to preserve renal function without oncological compromising. In this study, no recurrence was detected in the sutureless cohort, which might be partly due to the small sample size. As for functional preserving, 3 factors have been identified to be potentially important in renal functional loss at present, including removal of normal parenchyma, sutured parenchymal volume, and ischemia time. Notably, the sutureless technique prevents the loss of sutured parenchyma by coagulating the tumor bed. Zhang et al. 5 confirmed that the damage depth in porcine kidney was 1.8 mm, which indicated that the sutureless technique was safe if the distance between the tumor and the collection system was more than 2–3 mm.
Apart from this, previous studies have suggested that, during the reconstruction of the renal bed after tumor removal, the needle may lacerate the renal arterioles, which subsequently become pseudoaneurysms, with an incidence of as high as 15%.14,15 During the follow-up period, computed tomography scan revealed no pseudoaneurysm in the sutureless group, indicating that the sutureless technique might prevent the possibility of pseudoaneurysm. To create a visible surgical field to identify the tumor margin, the on-clamp technique was utilized for tumor excision and defect reconstruction, which might cause damage to renal function, even though the actual threshold was unknown. The significantly lower WIT in the sutureless group (11 minutes versus 16 minutes, P < .001) might remove these doubts. On the whole, the sutureless technique eliminates two factors affecting renal function and those explaining the lower AKI rate (4.6% versus 23.7%, P < .001).
With regard to long-term renal functional deterioration, there was no difference between the two groups (log-rank test, p = .304). In our study, most of the AKI cases recovered during the follow-up period. Such a result was consistent with those obtained by Simone et al., 8 who found that the 1-year decrease in split renal function was 1% (0%–5%) on renal scintigraphy, and those by Kihara et al., 10 who discovered that the average decrease in eGFR at 3 months after surgery was 2.4%. According to previous studies, up to 40% patients receiving off-clamp minimal invasive NSS could shift to on-clamp, 16 whereas in our subgroup analysis, no one in the sutureless and off-clamp cohorts shifted to on-clamp, showing its excellent hemostasis ability. The sutureless technique possesses numerous advantages, yet it is limited in small and superficial renal tumors. Recently, the inner suture and parenchymal non-renorrhaphy technique has been introduced and reported to attain promising outcomes in larger tumors (T1b). 17
To the best of our knowledge, our research is the only control study so far that compares the sutureless technique with the suture technique with comparable baseline characteristics and the longest follow-up time. Some of our findings are noteworthy. First, the sutureless technique significantly decreases AKI rate, thanks to the more parenchymal preservation and less ischemia time. Second, postoperative complications in the sutureless group are comparable but not superior to those in the suture group. Third, compared with the suture group, the long-term functional decline in the sutureless group is observed to be equivalent without any oncological compromise. Fourth, this technique avoids suturing and knotting, the challenging and technically demanding procedure during NSS, making it more feasible for novice urologists. Nevertheless, this study is limited by its retrospective nature and relatively small size of cohorts.
In conclusion, the sutureless technique utilizing mono-polar in LNSS is a safe and feasible procedure relative to the traditional suture method, which attains shorter WIT, decreased EBL, lower AKI rate, and comparable long-term oncological and functional outcomes. The sutureless technique can be available in appropriately selected patients.
Footnotes
Acknowledgment
The authors thank Prof. Chuan Liu for critical reading and suggestions.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (Grant No. 81801507 and 81803057) and Kuanren Talented Program of the second affiliated hospital of Chongqing Medical University (No. KY2019Y004).