
Abstract
Aim:
Emergent biliary drainage is necessary due to acute symptoms of choledochal cysts. Percutaneous biliary drainage (PBD), laparoscopic bile duct drainage (LBD), and laparoscopic cholecystostomy (LC) are the three most common drainage treatments. So far, there is no comparative study on these three approaches, which all have been applied in our hospital. This article compares the drainage effects of these three approaches and illustrates their respective merits and demerits, with the aim of providing a reference for clinical application.
Materials and Methods:
We conducted a retrospective study of 20 children who underwent biliary drainage before their definitive surgery due to acute symptoms of choledochal cysts between June 2008 and May 2015. Among them, 6 underwent PBD, 8 underwent LBD, and 6 underwent LC.
Results:
Preoperative abdominal pain, fever, and jaundice symptoms were effectively relieved by the three approaches. There were no significant differences in terms of the recovery of liver functions. The average interval and duration of procedures of three groups were PBD (25.00 ± 4.47 minutes and 262.50 ± 35.74 minutes), LBD (84.37 ± 24.99 minutes and 283.75 ± 39.62 minutes), and LC (50.83 ± 13.57 minutes and 218.33 ± 28.58 minutes), respectively.
Conclusions:
LC has advantages of a comparatively simple operation and no foreign body sensation (external drain) in the hepatic duct, which is beneficial for relieving inflammation of the common bile duct, and thus is suitable for majority of patients needing external bile drainage. Meanwhile, PBD and LBD also have their respective applicable patients.
Introduction
The incidence of choledochal cysts is around 1 of 1000 in Asia and 1 of 100,000–150,000 in western countries, and it mainly presents in infants, young children, and females, with the ratio between males and females as 1:3–4. Over 60% cases are diagnosed before 10 years of age. 1 Choledochal cyst etiology is due to a combination of the anomalous junction of the pancreaticobiliary duct and formation of protein plugs and calculi in the bile duct.2–5 When combined with a distal biliary obstruction, it would lead to raised intraductal pressure and cholestasis and then abdominal pain, fever, and clinical jaundice. In most cases, patients are treated conservatively, such as absolutely no food intake and intravenous antibiotics, until the biliary obstruction resolves and clinical symptoms are improved. Sometimes, conservative treatment as described above does not work and patients develop serious complications such as severe cholangitis, dysfunction of the liver, poor whole body condition such as sepsis and nutritional deficiency, and perforation of choledochal cysts. Patients with these serious complications require emergent biliary drainage. Traditional external drainage is accomplished by a laparotomy-guided T-tube drainage.
However, this procedure has disadvantages of a comparatively large and painful incision and adhesion of the surrounding tissues beneath the incision, which altogether increase the difficulty and risk for the following definitive surgery. The development and adoption of a laparoscopic hepaticojejunostomy technique have allowed an increasing number of medical centers to achieve the goal of small incisions and correspondingly improved cosmesis. A minimally invasive approach to emergent biliary drainage, such as percutaneous biliary drainage (PBD), 6 laparoscopic bile duct drainage (LBD), 7 and laparoscopic cholecystostomy (LC), 8 is preferred in patients with planned laparoscopic hepaticojejunostomy for definitive treatment. Currently, there is no study that compares these three minimally invasive drainage procedures and their effects on and roles in definitive surgery for treatment of choledochal cysts. Our center utilizes all three approaches of minimally invasive external drainage and we report our experience.
Materials and Methods
Clinical data of 20 children with congenital choledochal cysts treated by external biliary drainage, followed by definitive operation, from June 2008 to May 2015 in the Department of Pediatric Surgery, Qilu Hospital of Shandong University, are collected. Six of the patients are males and 14 are females, with an age range from 1 to 72 months. The patients are divided into three groups according to different surgical approaches: six cases underwent percutaneous external biliary drainage with an average age of 9.33 ± 8.98 months, eight cases underwent laparoscopic common bile duct drainage with an average age of 30.00 ± 22.08 months, and six cases underwent LC with an average age of 35.16 ± 23.46 months (Table 1).
Clinical Manifestations of the Three Groups of Patients
LBD, laparoscopic bile duct drainage; LC, laparoscopic cholecystostomy; PBD, percutaneous biliary drainage.
Operative methods
Ultrasound-guided PBD
Ultrasound-guided percutaneous drainage is accomplished at the bedside under intravenous and endotracheal anesthesia. The Seldinger technique is used to place a 6–8F single-lumen locking drainage catheter into the cyst over the point that has the smallest distance between the cyst and abdominal wall, which is selected as the puncture point. Finally, the catheter is securely affixed to the skin with a suture around the puncture point.
Laparoscopic bile duct drainage
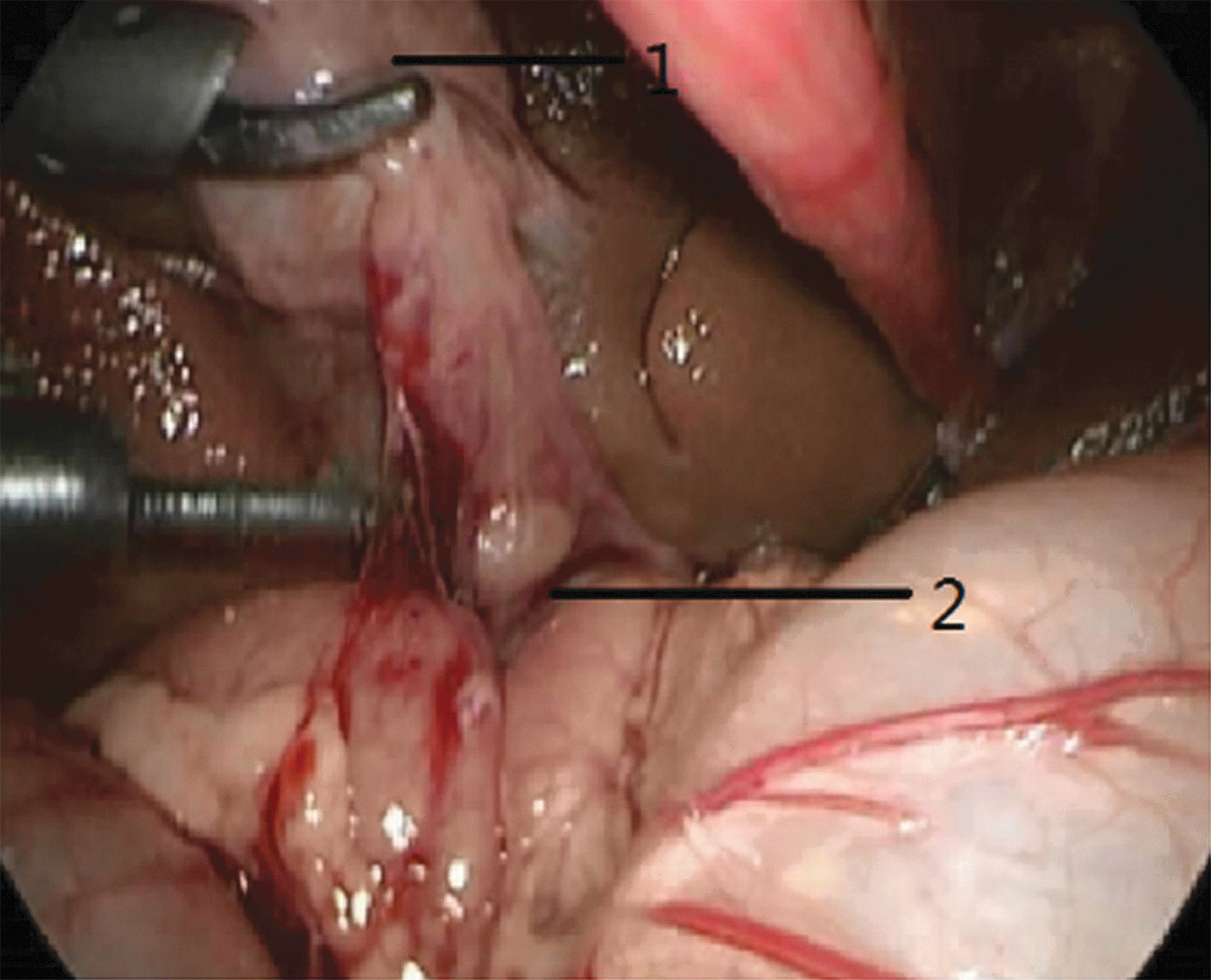
A 5-mm trocar is inserted through the middle abdominal incision and laparoscopy is conducted. Three additional 5-mm trocars are inserted at the right subcostal region along the midclavicular line, the paraumbilical area of the right rectus abdominis, and the top left rectus abdominis. The anterior wall of the common bile duct is incised. Then a 10–12F T-tube is placed and affixed with an absorbable suture. If a perforated choledochal cyst is found, then the T-tube is placed at the perforation site. Normal saline is used to flush the peritoneal cavity, and an indwelling drainage tube is placed within the cavity (Figs. 1 and 2).
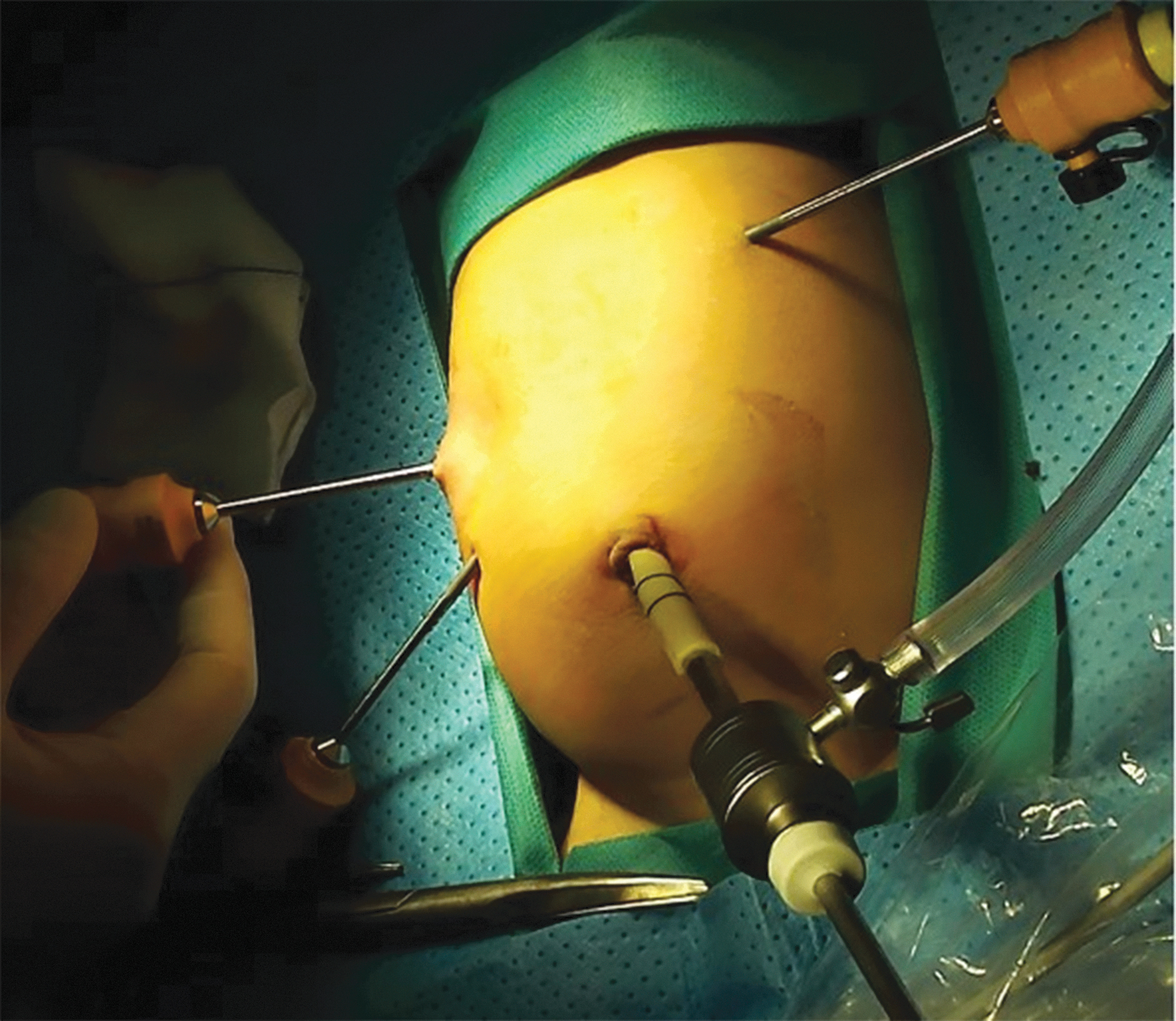
Port placement of laparoscopic bile duct drainage. Color images are available online.

Placement of the T-tube in laparoscopic bile duct drainage. Color images are available online.
Laparoscopic cholecystostomy
A vertical incision through the umbilicus is made and laparoscopy is performed. A second 5-mm trocar is placed in the right subcostal region. The abdominal cavity is explored to see if there is effusion and its nature, the diameter of the common bile duct, presence of perforation, location of the perforation, degree of filling of the gallbladder, and whether there are abnormalities such as twisting and narrowing of the gallbladder neck and cystic duct. A Satinsky clamp is then used to grasp the bottom of the gallbladder and after relieving the pneumoperitoneum, the bottom of the gallbladder is exteriorized out of the abdominal wall. A 38% diatrizoate meglumine solution is then infused through a fine needle into the gallbladder for cholecystocholangiography to define the anatomy and check for perforation or obstruction.
If an obstruction of the cystic duct or serious biliary tract perforation is found in cholecystocholangiography, bile duct drainage would be carried out. If there is no stenosis of the cystic duct and there is no obvious fistula in the common bile duct of the perforated patient, or leakage of the contrast medium is less, the bottom of the gallbladder is cut, an 8–12F silicone dual-lumen catheter is inserted, and the gallbladder wall around the catheter port is sutured. Then, the gallbladder is returned to the abdominal cavity, and the balloon is filled with saline to prevent prolapse. After checking the tube incision for leaks, the pneumoperitoneum is released. If perforation of the duct is found, another 5-mm trocar would be inserted in the right lower quadrant and an indwelling drainage tube would be placed within the peritoneal cavity after it is flushed using water.
In this process, the length of the intraperitoneal tube should be adjusted appropriately. The drainage tube and surrounding skin are properly fixed and bandaged, and finally the drainage bag is connected.
Laboratory tests, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transpeptidase (GGT), total bilirubin (TBIL), and direct bilirubin (DBIL), demonstrated a decrease in levels between the preoperative and postoperative fifth day in all three patient groups. The decrease in rate is calculated as (preoperative values − postoperative values)/preoperative values. The patients' 24-hour bile flux was also recorded after the postoperative normal oral feeding. Meanwhile, according to the clinical data, the corresponding operative time of the three procedures, interval between two operations, and duration of definitive operation were also recorded for analysis. All data were compared by R software through a series of Kruskal–Wallis tests.
IRB approval and written consent were not needed for this article.
Results
All external drainage operations were successful. When patients' uncomfortable symptoms such as fever, abdominal pain, and jaundice disappeared, their liver and coagulation functions improved and white blood cell count and C-reactive protein (CRP) were normal, which proved that patients have passed the acute inflammatory stage and they could undergo laparoscopic cyst excision and hepaticojejunostomy. As shown in Table 2, no statistical significance was found in the descent rates of ALT, AST, GGT, TBIL, and DBIL and patients' 24-hour bile flux among the three groups. The comparison and distribution of operative time, interval between two operations, and duration of definitive operation of the three groups are shown in Table 3 and Figure 3.
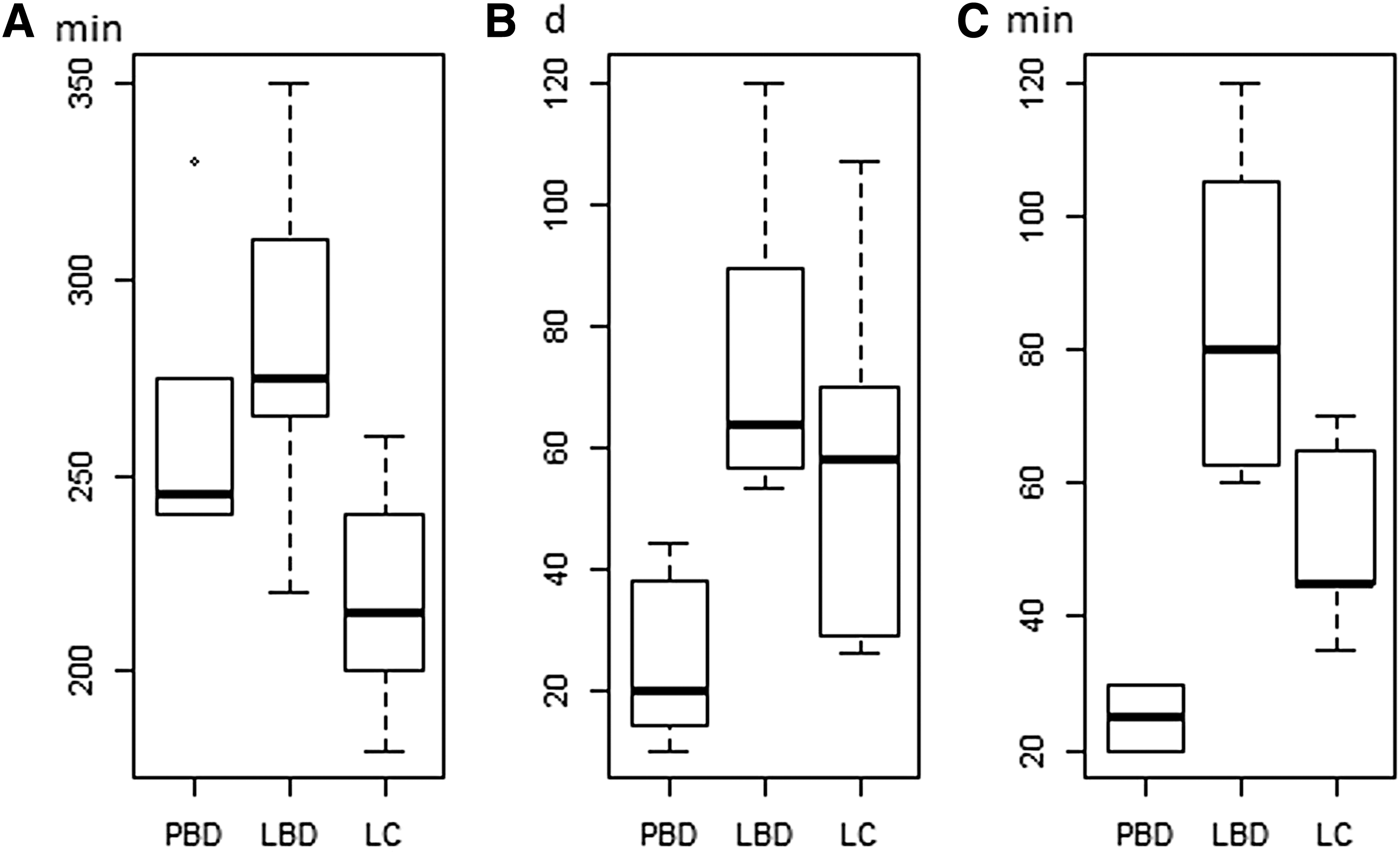
Distribution of operative time, intervals, and duration of the definitive surgery for the three groups.
Comparisons Among Three Drainage Methods on the Decrease in Rates of Alanine Aminotransferase, Aspartate Aminotransferase, Gamma-Glutamyl Transpeptidase, Total Bilirubin, Direct Bilirubin, and Daily Drainage Between Pre- and Postoperation
ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; GGT, gamma-glutamyl transpeptidase; LBD, laparoscopic bile duct drainage; LC, laparoscopic cholecystostomy; PBD, percutaneous biliary drainage; TBIL, total bilirubin.
Comparisons Among Three Drainage Methods on the Operative Time, Interval Between Two Operations, and Duration of the Definitive Surgery
LBD, laparoscopic bile duct drainage; LC, laparoscopic cholecystostomy; PBD, percutaneous biliary drainage.
There was one patient suffering from catheter blocking after PBD, while the other groups had no obstruction or detachment of tubes. Adhesions were observed mainly between the bottom of the gallbladder and the abdominal wall in definitive surgery after LC. Few adhesions were found around the common bile duct with relatively less inflammation. However, in the definitive operation after the LBD procedure, adhesions could be clearly seen around common bile duct fistula, in the intestinal canal, and greater omentum; the inferior border of the liver covered the anterior wall of the common bile duct; the hepatoduodenal ligament developed edema and thickening; and inflammation in the wall of fistula was obvious.
Discussion
The exact pathogenesis of congenital choledochal cysts is not clear, but anomalous pancreaticobiliary duct union exists in 30%–70% of patients. The common pancreaticobiliary duct is too long and the common bile duct merges into the pancreas at a right angle. The joint site is outside the ampulla of Vater ring muscle, resulting in reflux of pancreatic juice containing trypsin into the common bile duct, thereby causing inflammation and destruction of the bile duct wall mucosa and elastic fibrous tissue, leading to dilation of the biliary tract. If protein plugs or gallstones are formed in the bile duct or inflammation of the distal bile duct narrows or blocks the distal bile duct, increased pressure in the bile duct and cholestasis will occur.
Under high intraductal pressure, perforations caused by rupture of the thinned wall are found. If the obstruction cannot be relieved, the intraductal pressure would progressively increase, leading to rupture of the dilated biliary tract and leakage of bile into the liver. The leakage would further cause serious hepatic cell and synthesis injury and corresponding abnormal liver and blood coagulation functions. Undoubtedly, bleeding can easily occur. 9 Hence, it is necessary to relieve obstructions, perform bile drainage, and decrease the intraductal pressure when there are choledochal cysts complicated with infection of the biliary tract, hepatic dysfunction, and cyst perforation.
Compared with the traditional, laparotomy-guided T-tube drainage, PBD, LBD, and LC are increasingly applied due to their advantages of less trauma, small incision, speedy recovery, and improved cosmesis. However, so far, there is no report comparing the drainage effects of these three methods. By comparison, we did not find significant differences in the descent rates of ALT, AST, GGT, TBIL, and DBIL and patients' 24-hour bile flux among the three groups.
Meanwhile, they were all effective in relieving uncomfortable symptoms such as fever, abdominal pain, and jaundice. Therefore, we can draw the conclusion that these three approaches are all effective in temporarily relieving obstructions, draining bile, and decreasing intraductal pressure. However, different operative methods endow the three approaches with their respective strengths and weaknesses.
With regard to PBD, no incision or entrance into the abdominal cavity is needed. B-mode ultrasonography helps to locate the point through which bile drainage is conducted percutaneously. However, without entering the abdominal cavity, the existence of perforation in the bile duct or encapsulated effusion cannot be determined by naked eyes. What is more, if the insertion is very close to the duodenum, ligation of the distal end of the common bile duct in definitive surgery would be difficult. In addition, the drainage tube is comparatively thin and small and affixed only by skin, therefore long-term drainage would lead to obstructions and prolapse of the tube. However, eliminating inflammation around a dilated biliary tract caused by perforation or infection of the bile duct normally requires 2 months. 10
Summary
PBD is recommended for patients with comparatively large cysts or those in poor general medical condition who cannot safely undergo definite surgery; due to its convenience; and because there is no need for an abdominal incision and pneumoperitoneum, which is very advantageous. According to our experience, intraperitoneal adhesions are relatively weak within 20 days (Fig. 4) and will be worsened with the extended duration of an indwelling drainage catheter.
No serious adhesion adjacent to the hepatic portal after PBD by secondary stage operation.
LBD allows for exploration of the abdominal cavity and irrigation of perforations and peritoneal effusion at the same time if those conditions are encountered. The catheter is located within the common bile duct, thus it conducts bile drainage directly. Since the catheter is relatively thick and in the shape of a T or mushroom, it is not easy to prolapse or be obstructed. However, this method requires porta dissection, which is more complicated compared with the other two procedures, so the operation is longer with relatively high risk. Postoperative foreign body stimulation would easily cause adhesions at the intestinal canal, greater omentum, or even inferior border of the liver to form sinus. The catheter would stimulate the wall of the cyst, which leads to chronic inflammation and fibroplasia as well (Fig. 5). Therefore, when performing exteriorization of cyst excision, the volume of blood loss would increase and cyst exteriorization becomes difficult.

More serious adhesion adjacent to the hepatic portal after LBD by secondary stage operation.
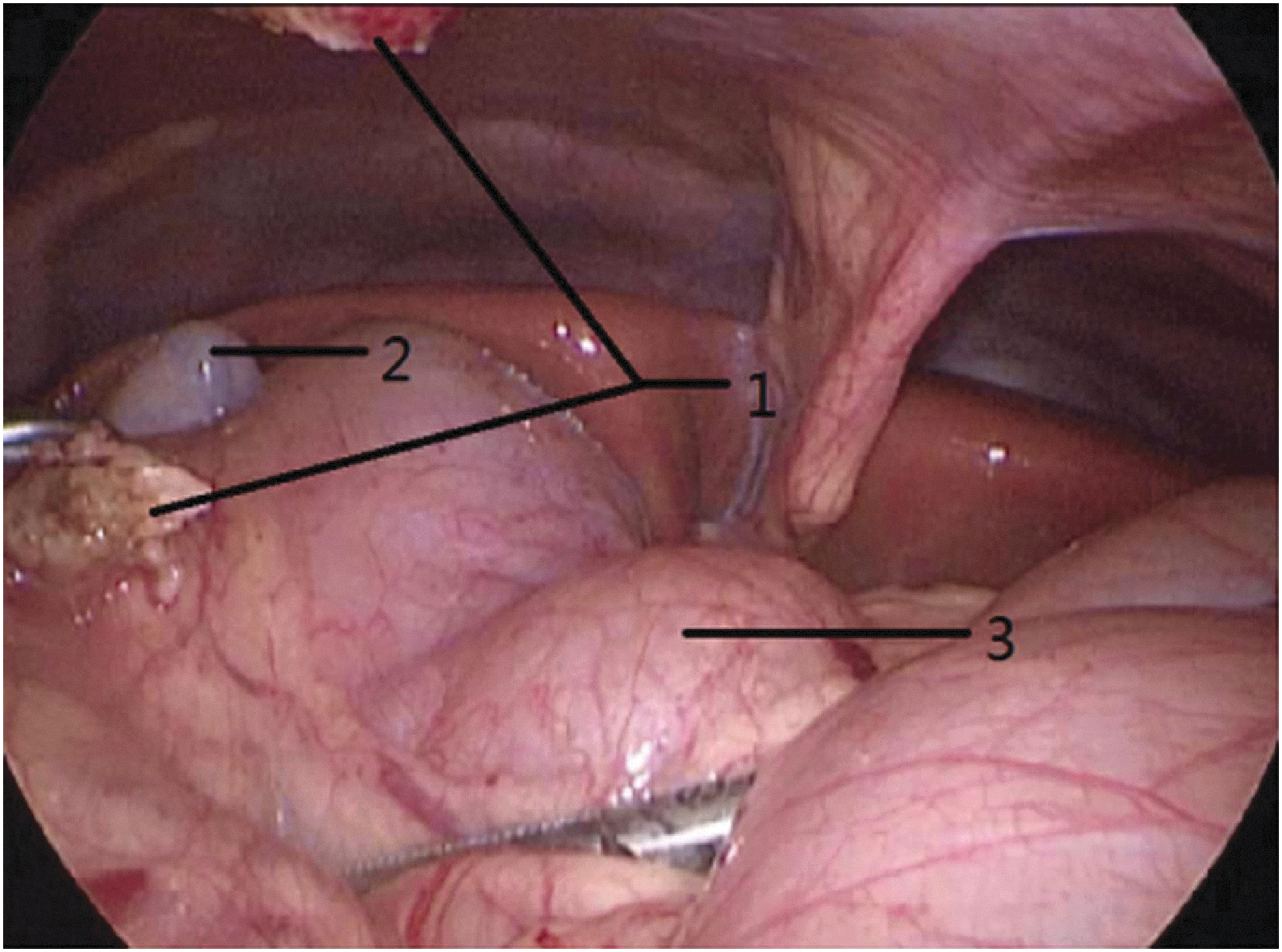
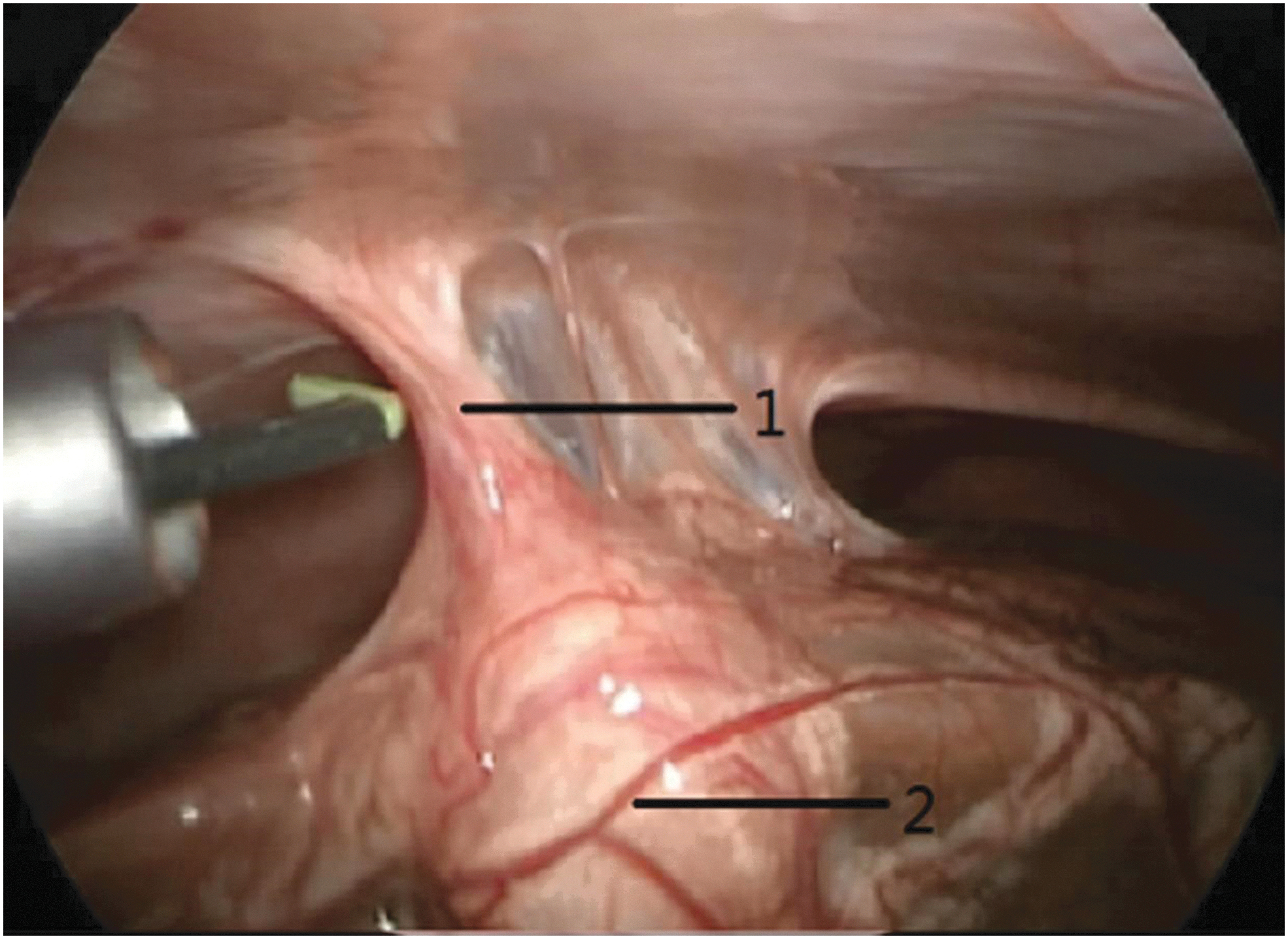
LC was believed to be inferior to the above methods or even had the possibility of ineffective drainage. Cholangiography was conducted first to test whether there was a slender, twisted, or obstructed cystic duct. If so, LBD would be performed to avoid ineffective drainage. Actually, our results show that the drainage effect of LC is comparable with that of LBD. Since the bottom of the gallbladder is close to the abdominal wall with a certain extension, it is easier to exteriorize the cyst through the trocar incision without dissecting the porta. Moreover, postoperative adhesions develop between the bottom of the gallbladder and the abdominal wall (Fig. 6), which is relatively distant from the choledochal cyst. In addition, without foreign body stimulation, inflammation or edema of the choledochal cyst and its surroundings would easily decrease (Fig. 7), which makes separation of the choledochal cyst much easier. 11 For patients with perforations and bile peritonitis, irrigation of the abdominal cavity and drainage can be conducted concurrently. If the perforation is small, the relief from adhesions of the surrounding tissues and decrease of intraductal pressure would help the fistula recover naturally. 4
Gallbladder and abdominal wall adhesion after LC by secondary stage operation.
No serious adhesion adjacent to the hepatic portal after LC by secondary stage operation.
Limitations
Cases of patients in serious conditions, especially those who require bile drainage, are quite few, which limits the sample size of our study. From our limited samples, we provided the following suggestions: LC, due to its simple operation, stable fixation, least influence on the common bile duct, and benefit of definitive surgery, is suitable for majority of patients needing external biliary drainage. If the intraoperative cholangiography indicates the existence of relatively large perforations or a narrow, twisted, or obstructed cystic duct, LBD is more safe and effective. As for patients with relatively large cysts and no complicated perforations, PBD, as a temporary drainage method with no need for abdominal incision and pneumoperitoneum, would be the first choice among the three procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.