
Abstract
Introduction:
To reoperate a patient with Hirschsprung disease (HSCR) can be technically demanding and most surgeons would resort to conventional laparotomy. This article describes a series of patients with postoperative obstructive symptoms who underwent minimally invasive redo pull-throughs (MIRPT) (either laparoscopic or robotic) to assess the role of minimally invasive surgery (MIS) in complicated HSCR patients.
Patients and Methods:
All consecutive HSCR patients with postoperative obstructive symptoms, who underwent MIRPT with fast track concepts of care between January 2012 and January 2020, have been included. Data regarding indications, surgical details, complications, and outcome have been compared to those of a series of patients who underwent conventional laparotomic redo.
Results:
Sixteen patients were included. Male to female ratio was 4.3:1. Median age at surgery was 78 months. Eleven patients underwent laparoscopic redo and 5 underwent robotic redo. Median length of follow-up was 49 months. Reasons for redoing were transition zone pull-through, residual aganglionosis, anastomotic retraction or leak, rectal diverticulum, and refractory anastomotic stricture. No major intraoperative complication occurred. No conversion to laparotomy was required. One patient experienced cuff stricture requiring laparoscopic release. Two patients reported bouts of enterocolitis postoperatively. Compared to classic laparotomic redo pull-throughs (49 patients with complete data), overall complications were significantly less frequent, accounting for 1 and 21 events, respectively (6% versus 43%) (P = .0067). Continence after a median of 21 months postoperatively scored excellent to good in 9 out of 12 patients, who were assessed on this regard (75%), without statistically significant differences.
Conclusions:
MIRPT proved to be effective and safe in HSCR patients complaining postoperative obstructive symptoms. Robotic surgery could play a crucial. Our study confirms that complicated HSCR cases can be safely managed by means of MIS, applying concepts of fast track care to serve the best for our patients.
Introduction
The management of patients with Hirschsprung disease (HSCR), who experience postoperative obstructive symptoms, can be extremely demanding even for experienced centers, both from a diagnostic and therapeutic point of view.1–5 This is the reason why most surgeons dealing with this delicate subset of HSCR patients would resort to conventional open laparotomy.1–3,6 Nonetheless, although anecdotical, colonic mapping, cuff release, and even complete redo pull-through have been recently reported with good results, suggesting a room for laparoscopy even for complicated and plurioperated HSCR patients.7–11 The aim of our article is to describe a bicentric series of HSCR patients with persistent postoperative obstructive symptoms, who underwent laparoscopic or robotic redo pull-throughs.
Materials and Methods
All consecutive HSCR patients who underwent a redo pull-through for persistent obstructive symptoms between 2012 and 2020, and who are being followed up at the Umberto Bosio Center for Digestive Diseases, The Children Hospital, Alessandria, have been retrospectively included. Institutional Ethical Committee approval was deemed unnecessary, given the retrospective observational nature of this study.
Inclusion criteria were as follows: (1) reliable HSCR diagnosis; (2) presence of postoperative obstructive symptoms; and (3) reoperations performed with laparoscopic approach
Exclusion criteria were as follows: (1) unclear and/or unreliable HSCR diagnosis and (2) lack of follow-up data in the long term
Confirmation of HSCR diagnosis
Two experienced pathologists (P.N. and/or N.M.) reassessed the slides belonging to either rectal suction biopsies or full-thickness intraoperative samplings harvested during pull-through. Slides stained with conventional histology, enzymohistochemistry or immunohistochemistry, were reassessed to confirm the exact HSCR diagnosis.
Diagnostic workup
Each patient with postoperative obstructive symptoms underwent a comprehensive diagnostic workup with repeated rectal suction biopsy, barium enema, rectal examination under anesthesia, and further investigations (i.e., full-thickness rectal biopsies, laparoscopic colonic mapping, etc.) according to what was published by our group in 2010, 4 which is consistent to a more recent publication by Langer et al. 5
Redo pull-through
Each procedure consisted of three major steps: (1) laparoscopic or robotic isolation of the previously pulled-through bowel from surrounding structures, including ureters, vas, tubes, vagina, and small bowel; (2) ligation of mesentery by means of advanced bipolar energy devices (Ligasure, Minneapolis, MN); (3) transanal isolation of the pulled-through bowel and coloanal anastomosis to the “normally innervated biopsy” (detected during a previous elective laparoscopic innovative mapping). All postoperative management was performed according to fast-track concepts of care, including early feeding, mobilization, and discharge.
Collected data
Demographic data, extent of aganglionosis, associated anomalies, symptoms and complaints leading to surgery, indications for a redo, surgical details, complications, and functional outcome have been recorded according to data protection Act.
Functional outcome
The results of redoes performed with a minimally invasive approach were compared to those of a series of consecutive HSCR patients, who underwent a redo with conventional laparotomy (part of these data have been previously published by our group 4 ).
Definitions:
Extent of aganglionosis
○ Classic HSCR—aganglionosis extending up to the splenic flexure
○ Long HSCR—aganglionosis extending beyond the splenic flexure, but confined within ascending colon
○ Ultralong HSCR or total colonic aganglionosis—aganglionosis extended to the terminal ileum with variable small bowel involvement
Continence—continence was assessed only in patients older than 4 years of age, without intellectual disability, and with a minimum 6 months of follow-up according to modified Wingspread scoring system. Continence was graded into Excellent, Good, Fair, and Poor. 12
Enterocolitis Hirschsprung associated enterocolitis (HAEC)—defined according to Pastor criteria 13 and graded according to El halabi criteria (mild, moderate, and severe) 14
Perineal rash—severe perineal excoriation that interferes with a normal quality of life lasting longer than 6 weeks and requiring medications or change of diet
Statistical analysis
Descriptive statistics were reported as absolute frequencies and percentages. Median and ranges were used to describe semiquantitative and quantitative variables. Two-tailed Fisher's exact test was used to compare categorical variables. Unpaired t-test was used to compare continuous variables. A P lower than .05 was considered to be statistically significant.
Results
Demographics and phenotype
A total of 16 HSCR patients underwent 16 redo pull-throughs with laparoscopic approach between March 2012 and March 2020. Male to female ratio was 4.3:1. Median age at surgery was 49 months (ranging between 14 months and 16 years). Median time span between the last pull-through (2 patients underwent 2 previous pull-throughs) and the laparoscopic redo was 36 months (ranging between 6 months and 15 years). Twelve patients suffered from Classic-HSCR. Five associated anomalies were detected, including 2 central nervous system and 1 skeletal congenital abnormality, 1 Ondine Syndrome, and 1 visual impairment.
Clinical features
Fifteen out of these 16 patients were operated elsewhere. All patients complained of obstructive symptoms. Symptoms included severe constipation requiring regular washout (14 patients), abdominal bloating (8 patients), recurrent HAEC occurrences (9 patients), perianal excoriation (4 patients), and failure to thrive (2 patients). Three patients complained recurrent bouts of HAEC both preoperatively and postoperatively showing clear predisposition.
Procedures—redo pull-throughs
Indications for redoing were transition zone pull-through in 7 patients, residual aganglionosis in 3, anastomotic retraction in 3, anastomotic leak in 1, iatrogenic posterior rectal diverticulum in 1, and refractory anastomotic stricture in 1 (Fig. 1 shows water-soluble contrast enemas of patients with residual innovative issues, who underwent laparoscopic or robotic redo pull-throughs). Eleven patients underwent laparoscopic redo pull-throughs and 5 underwent total robotic redo pull-throughs. Robotic approach was adopted since September 2017, when we implemented the program of pediatric robotic surgery at the Umberto Bosio Center for Digestive Diseases, The Children Hospital, Alessandria, Italy (see Table 1 for details). Since then, all patients were approached robotically, but 2 who were operated with conventional laparoscopic approach due to the nonavailability of the robotic system (shared with other adult specialists). No intraoperative complication occurred. No conversion to laparotomy was needed. Median hospital stay was 7 days (range 5–10 days). All patients, but 2, experienced complete resolution of preoperative obstructive symptoms. The remaining 2 patients experienced transient persistence of obstructive issues. One patient experienced cuff stricture that underwent successful laparoscopic release. The same patient experienced postoperative HAEC. One patient experienced mild transitory constipation that settled a few months postoperatively after a short treatment with stool softener. Median follow-up of laparoscopic redoes was 21 months (ranging between 6 and 65 months). Two patients experienced bouts of mild HAEC postoperatively. Given the age and cognitive requirements needed to assess continence, only 12 out of 16 patients who underwent a laparoscopic redo could be assessed on this regard. Four patients reported an excellent continence, 5 a good outcome, 2 fair, and 1 poor (this patient required laparoscopic cecostomy button insertion). Overall, 9 out these 12 patients (75%) reported excellent to good continence.
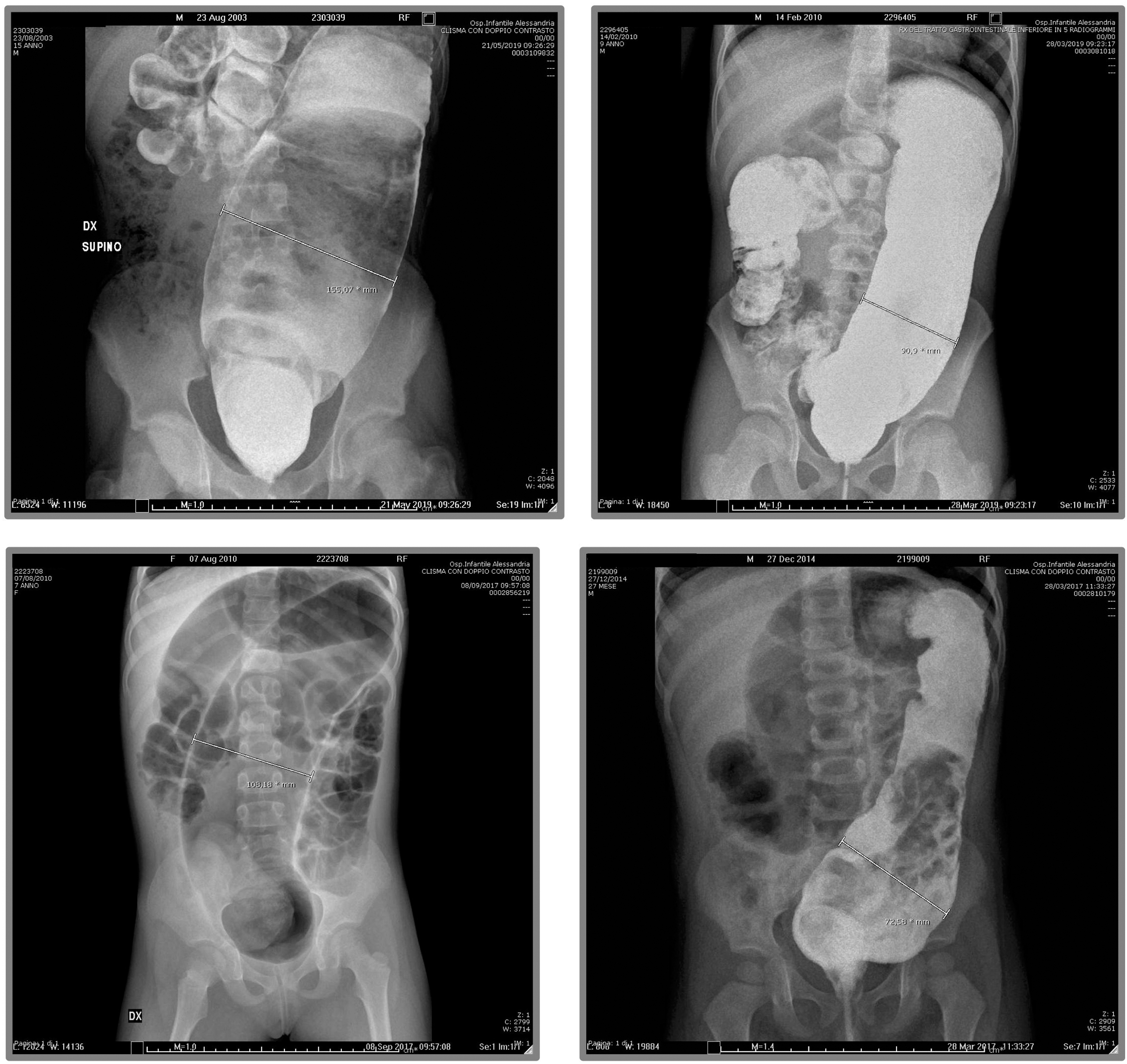
Water-soluble contrast enemas of patients with innovative issues who underwent laparoscopic mapping and full-thickness anastomotic biopsy. Starting from top left clockwise, we can observe the enema of a patient with residual aganglionosis and three enemas of patients with zone pull-through. The dilated descending colon is impressive in all cases. The bottom left picture shows the starting X-Ray of a contrast enema where the air-filled descending colon is evidently dilated.
Overall Series of Sixteen Patients Previously Operated for Hirschsprung Disease, Who Underwent a Laparoscopic or Robotic Redo
The incidence of complication proved to be low, well within literature ranges. Most robotic redoes have been performed since the implementation of the program of pediatric robotic surgery in September 2017.
Agan., aganglionosis; Anast., anastomosis; Divert., diverticulum; Lap., laparoscopic; n.a., not available; PT, pull-through; Retract., retraction; Rob., robotic; Strict., stricture; TCSA, total colonic aganglionosis; TZ, transition zone.
Comparison of laparoscopic and laparotomic redo pull-through
We compared these results with those of 60 patients who underwent a conventional laparotomic redo procedure since 1992, who are being followed up at the Umberto Bosio Center for Digestive Diseases of the Children Hospital, Alessandria. Only those with complete data regarding postoperative complications and continence in the long term were included in this comparative assessment (most of these data have been previously published by our group in Pini-Prato et al. 4 ). Median follow-up for patients who underwent laparotomic redoes was 95 months (ranging between 6 months and 18 years). Comparing these results, we could observe that functional outcome does not significantly differ (P = 1.0000), whereas surgical complications proved to be significantly less frequent in case a laparoscopic approach was used (P = .0067). See Table 2 for details.
Comparison of Laparoscopic and Laparotomic Redo for Complicated Hirschsprung Disease Patients
No statistically significant difference in terms of functional outcome has been detected comparing different approaches. On the other hand, we could observe a significantly lower incidence of surgical issues in those patients who underwent a laparoscopic redo (either robotic or not). When addressing complications by type, we could not identify any significant difference, although anastomotic strictures and anal sphincter achalasia showed an intriguing trend toward significance.
HSCR, Hirschsprung disease; n with data, number of patients with available data; pts, patients; TCSA, total colonic aganglionosis.
Discussion
Our study demonstrated that laparoscopic approach is feasible and safe for complicated HSCR patients, regardless of the number of previous ineffective procedures even in case of multiple laparotomies and peritoneal adhesions. Both “conventional” laparoscopy and robotic surgery proved to ensure a safe and effective reoperation.
The significantly lower incidence of surgical complications observed in our overall series of patients proved that reoperations for HSCR with a minimally invasive approach is even safer when compared to a conventional laparotomic one. Nonetheless, when complications are addressed by type (i.e., adhesions, strictures, leaks, etc.), none proved to be significantly more frequent in patients undergoing laparotomic redoes. This aspect suggests that minimally invasive surgery (MIS) provides overall safer surgery without predominant effects on specific areas of criticality for patients undergoing a redo.
From a functional point of view, continence proved not to significantly differ postoperatively with a promising 75% expectation of Excellent to Good continence in the long term.
On the ground of these considerations, we could therefore confirm the promising results previously reported by Xia et al. and Jiang et al.7,8
It is well known that residual innovative issues represent the most frequent cause of postoperative obstructive symptoms in HSCR.4,5 The results of our series confirmed this aspect as over 60% of our patients required a redo pull-through for residual innovative issues. Nonetheless, obstructive symptoms can be also due to anatomical abnormalities such as twisting, strictures, leakage, and others. The inclusion of patients with a number of anatomical issues in our series confirmed that even complex surgical issues can be safely and effectively addressed by means of a minimally invasive approach. Our series of patients thus confirmed the versatility of MIS in addressing postoperative obstructive issues in HSCR. In fact, we could treat both innovative and anatomical issues with the same safety and effectiveness.
Plurioperated patients, even those who have been previously approached by means of conventional laparotomy, can be safely and effectively managed with a minimally invasive approach. Most of the patients from this series, who experienced severe peritoneal adhesions, required prolonged adhesiolysis, but could be effectively treated with a laparoscopic approach maintaining a successful outcome and the goal of treatment. Although conversion rate proved to be marginal (none of the patients in this series), laparoscopic surgeons must be always prepared to convert. Most important, they must always consider and balance the risk-benefit ratio of a minimally invasive approach before and during surgery to avoid the increase of intraoperative complications that can occur when MIS is not safely controlled.
With specific regard to robotic surgery, our study is the first in literature to report a number of HSCR patients who underwent redo pull-throughs for postoperative obstructive symptoms with a robotic approach. Robotic surgery in HSCR has been reported only for primary pull-throughs.17–19 We recently reported a relatively large series of HSCR patients undergoing totally robotic Soave pull-through, including 2 patients who underwent a robotic redo pull-through. 20 Given the increased dexterity of robotic instrumentation, three-dimensional vision, and 10 × magnification of robotic devices, as well as the higher median age of patients undergoing a redo compared to those undergoing a primary pull-through, we can speculate that robotic approach could be even safer and more effective in this specific subgroup of HSCR patients. The limited number of patients who underwent a robotic redo pull-through compared to those who underwent a laparoscopic redo (5 versus 11) prevented any statistically reliable analysis. Even so, functional results are promising with 100% of patients who underwent robotic redoes showing Good to Excellent continence.
This study has several limitations. First, our relatively small series of patients do not allow to draw definitive conclusions even if larger series of reoperations for rare diseases are difficult to collect. As the Umberto Bosio Center for Digestive Diseases represents a national referral center for HSCR, we could enroll the largest number of HSCR patients undergoing reoperations reported in western countries so far. Second, the relatively small number of patients whose continence could be addressed made this study closer to a case series report, thus limiting the validity of interpretation of functional results in the long term. Even so, results proved to be definitely promising. Third, the referral role of our center implies a selection BIAS that can interfere with the overall interpretation of the results, even if the demographic data (male to female ratio above all) do resemble those of a “classic” HSCR population.
Conclusion
To conclude, provided the patients undergo a strict diagnostic workup as those previously reported4,5 and reoperations are performed by experienced surgeons with large caseloads of redoing, results of minimally invasive reoperations are satisfactory and do not differ from those achieved with a conventional laparotomic approach, but with the significant reduction of surgical issues and the obvious advantages of MIS in terms of postoperative pain, fast track concepts of care, and cosmetic results. 17 Although our results did not provide evidences of enough strength to promote laparoscopic redoing over laparotomic ones, we can confirm the safety of minimally invasive approaches even for complicated HSCR patients. All in all, based on the results of our series of patients, we can state that laparoscopic/robotic redo pull-throughs for HSCR patients with postoperative obstructive symptoms, in experienced hands and in dedicated centers, represent safe and effective therapeutic options to serve the best for our patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.