
Abstract
Background:
The aim of this study is to report short- and long-term results using video-assisted ablation of pilonidal sinus (
Methods:
We included all consecutive patients with a recurrent
Results:
Sixty-three patients were included in the analysis. Recurrence rate at 1-year follow-up was 4.7% (3 patients on 63), at 3-year follow-up was 11.7% (4 on 34), and at 5-year follow-up was 23.07% (3 on 13). A 3- and 5-year follow-up was completed by 34 and 13 patients, respectively. The mean time off work was 3.5 ± 1.5 days, time to sitting on toilet without pain was 1.5 ± 1.1 days, and time to walk without pain was 1.3 ± 0.9 days. The mean time to wound healing was 27.9 ± 10.3 days, with a rate of incomplete wound healing of 4.7%. Postoperative infection rate was 7.9%. The mean postoperative pain was 1 ± 0.9 at 6 hours after the procedure, 0.6 ± 0.6 at 1 day and 0.1 ± 0.3 at 1 week. Patients' satisfaction was good in 98.5% of patients. After the multivariate analysis, no parameters showed an influence on the postoperative outcomes.
Conclusions:
Our results encouraged to adopt an endoscopic approach even in case of recurrent
Introduction
Pilonidal sinus (PS) is a troublesome disease of the natal cleft of the sacrococcygeal region. It occurs mainly in young men with a reported incidence of about 26 per 100,000. 1 Its pathogenesis is not really known, but common risk factors included obesity, hirsutism, sedentary occupation, and local irritation.2–4
Many different approaches to this common disease have been proposed during the past decades, 5 but nowadays the gold standard treatment has still not been assessed.
The most serious problem of the various surgical approaches proposed is the recurrence rate, ranging from 0% to 40%. 6
The introduction of endoscopic approach to
However, although this kind of procedures is nowadays recognized as safe and effective in terms of recovery outcomes, patients' satisfaction,8,9 and long-term recurrence,
10
less is known about its adoption in case of recurrent
The aim of this study is to report short- and long-term results using video-assisted ablation of pilonidal sinus (VAAPS) technique to treat recurrent
Materials and Methods
Our study was approved by Institutional Review Board of “Federico II” University before review of any patient material. From a prospectively maintained database of the VAAPS, we included in this study all consecutive patients with a recurrent
Surgical technique
All the procedures were performed with a standardized surgical technique under local anesthesia with 30–60 mL of mepivacaine (Carbosen, 20 mg/mL; Galenica Senese). The patients were placed in the prone position with the legs slightly apart and the buttocks retracted by an adhesive tape.
The VAAPS procedure was performed as previously described,7,13 by using a 4-mm continuous flow operative hysteroscope (Bettocchi Office Hysteroscope “size 4,” Karl Storz) with a 30° grade optic, which incorporated a 5-Fr operative channel. After the widening of the lowest pit of the pilonidal cavity, the endoscopic was inserted through the orifice and the pilonidal cavity was irrigated with a continuous flow of saline. Under direct vision, hairs were removed with the grasping forceps and a mechanical adhesyolisis was performed. Finally, the sinus cavity was completed ablated by using a 5-Fr bipolar electrode and a complete debridement of the sinus cavity was performed with the Volkmann spoon.
Outcomes
Outcomes were classified as primary and secondary outcomes.
Primary outcomes of this study were recurrence rate at 1-, 3-, and 5-year follow-ups.
Secondary outcomes were time off work, time to sitting on toilet without pain, time to walk without pain, time to wound healing, rate of incomplete wound healing and postoperative infection, postoperative pain at 6 hours, 1 day, and 1 week, patients' satisfaction 1 month after the complete wound healing.
Recurrence was defined as an additional occurrence of local pain, discharge, or swelling after an interval following complete wound healing.
Time off work was considered as the time of inactivity from the work. The criteria for returning to work was the absence of any limitation to normal daily activities, including no pain while resting or moving, walking and sitting, and no need to dress the wound more than once a day.
Time to wound healing was defined as the days necessary to obtain a complete epithelization of the wound in absence of any wound discharge.
Incomplete wound healing was defined as persisting wound discharge or swelling after postoperative day 60.
Wound infection was defined as redness and/or edema of the skin and/or discharge.
Postoperative pain was measured by a visual analog scale, a 10-cm long line ranging to 0 for “no pain” to 10 for “worst pain ever felt.”
Patients' satisfaction was obtained by a numeric scale, which ranged from 0 for no satisfaction to 10 for a complete satisfaction. An independent observer, unaware of the allocation of each patient, collected the satisfaction scale evaluation.
Demographic data (age, gender, body mass index [BMI], and smoking and obesity status) and data about recurrence of
Statistical analysis
Statistical analysis was performed with SPSS 23.0. (SPSS, Inc., IBM, Armonk, NY). Continuous data were expressed as mean ± standard deviation; categorical variables were expressed as %. To adjust for all the variables, and to make predictions, multivariate analyses were performed with primary and secondary outcomes (logistic regression) as dependent variables, and with patients' and sinuses' characteristics as independent variables.
Results
Our analysis included 63 patients. Of these, all of patients completed the 1-year follow-up, 34 (54%) the 3-year follow-up, and 13 (20.6%) the 5-year follow-up. No patient was lost during the follow-up period.
Demographic and sinuses' characteristics are summarized in Table 1.
Patients' and Sinuses' Characteristics
BMI, body mass index; PS, pilonidal sinus.
Of the 63 enrolled patients, 42 (66.6%) were men and 21 (33.4%) were women. Mean age was 27.4 ± 5.5 and mean BMI was 26.5 ± 4.88. Obese patients were 15 (23.8%) and smokers were 34 (53.9%).
Considering sinuses' characteristic, mean number of pits was 1.7 ± 0.88, with a number of pit ranging from 1 to 4. Lateral localization of one or more pits was present in 28 patients (44.4%), with a mean distance of the most lateral pit from midline of 2.2 ± 1.2. The mean distance of the lowest pit from the anal verge was 2.7 ± 1.25. Mean number of previous
Primary and secondary outcomes are summarized in Table 2.
Primary and Secondary Outcomes
Three-year follow-up was completed by 34 patients. Five-year follow-up was completed by 13 patients.
FU, follow-up; VAS, visual analog scale.
Recurrence rate at 1-year follow-up was 4.7% (3 patients on 63), at 3-year follow-up was 11.7% (4 on 34), and at 5-year follow-up was 23.07% (3 on 13). As mentioned, all the patients completed the 1-year follow-up, 34 completed a follow-up of 3 years, whereas only 13 patients completed the 5-year follow-up. A detailed distribution of the recurrences is shown in Figure 1.
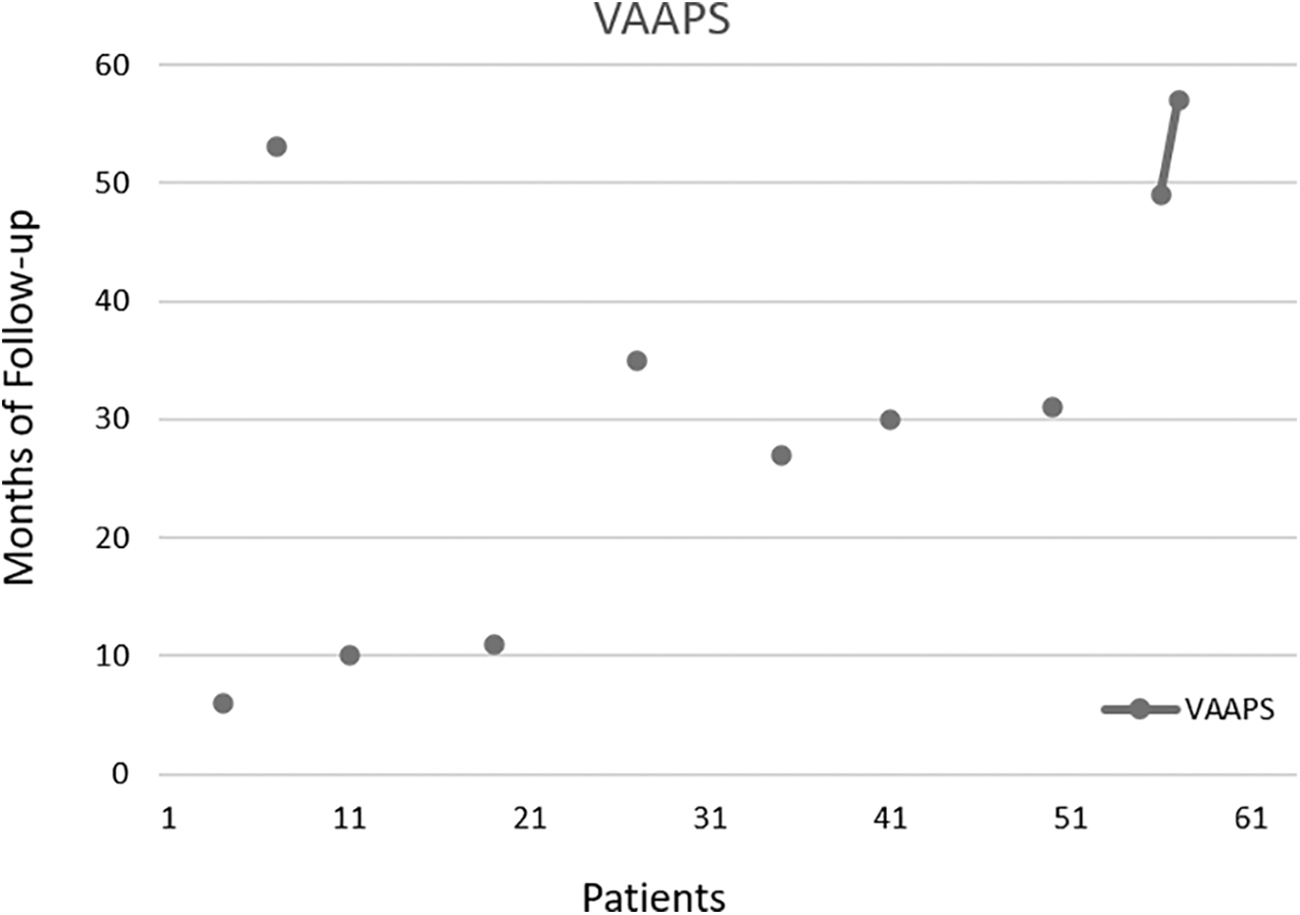
Detailed distribution of the recurrences. VAAPS, video-assisted ablation of pilonidal sinus.
The mean time off work was 3.5 ± 1.5 days, whereas time to sitting on toilet without pain was 1.5 ± 1.1 days, and time to walk without pain was 1.3 ± 0.9 days.
The mean time to wound healing was 27.9 ± 10.3 days, with a rate of incomplete wound healing of 4.7% (3 patients on 63). Postoperative infection rate was 7.9% (5 patients on 63).
The mean postoperative pain was 1 ± 0.9 at 6 hours after the procedure, 0.6 ± 0.6 at 1 day and 0.1 ± 0.3 at 1 week. Patients' satisfaction was good in 98.5% of patients (62 on 63) with a mean value of 8.1 ± 0.9. Only 1 patient was not satisfied by the treatment.
After the multivariate analysis adjusting for all the covariates (gender, age, BMI, smoking and obesity status, number of pits, localization of the pits, mean distance from the anal verge and from the midline, number of previous treatment and typology of the last surgical treatment), no parameters showed an influence on the postoperative outcomes.
Discussion
Since their introduction few years ago, the endoscopic techniques to treat the
In the past few years, several studies have demonstrated the short-term advantages of these techniques.7–9,14–19
In fact, all the performed studies concluded that, if compared with standard surgical approach, the endoscopic technique was associated with a shorter inactivity time, a low rate of postoperative infection, a better cosmetic result, and a better patients' satisfaction.7–9,14–19
Furthermore, few studies have been performed to assess if minimally invasive technique was associated with good long-term results in terms of recurrence rate, but the results are still controversial.10,20,21
In fact, Milone et al. 10 in their long-term results of a randomized clinical trial comparing endoscopic and conventional surgical techniques concluded that there was no difference in terms of long-term recurrence between the two techniques, with a higher patients' satisfaction and better cosmetic results in the endoscopic group.
Similarly, Giarratano et al., 20 in their long-term analysis of a prospective series, concluded that the endoscopic technique was an uneventful procedure, with good aesthetic results and a low recurrence rate.
On the contrary, in an analysis of long-term results comparing endoscopic treatment and Limberg flap for complicated pilonidal disease, Romaniszyn et al. 21 concluded that the endoscopic procedure was associated with a significantly lower success rate than the Limberg flap procedure.
However, although if endoscopic technique seems to be a valid surgical option to treat chronic
In the past year, two studies were performed about the endoscopic approach to recurrent
Meinero et al.
11
analyzed data from 122 patients with recurrent
Similar results were obtained from an analysis of a pediatric population performed by Esposito et al.
12
In fact, analyzing the results of the endoscopic approach on 10 children with a recurrent
The results obtained by the analysis of our prospectively maintained database are in line with the current literature.
In fact, according to Meinero et al., 11 the complete wound healing was obtained in 95.3% of the patients, with a mean time to wound healing of 27.9 ± 10.3 days, confirming the effectiveness of this technique.
Furthermore, according to Esposito et al., 12 also the short and painless postoperative course has been confirmed by our results.
In fact, the mean postoperative pain was 1 ± 0.9 at 6 hours after the procedure, 0.6 ± 0.6 at 1 day, and 0.1 ± 0.3 at 1 week, whereas the mean time off work was 3.5 ± 1.5 days.
In addition, the endoscopic approach showed to be associated with a good patients' satisfaction even in case of recurrent
However, despite these short-term results, we tried to confirm the long-term effectiveness by the analysis of the long term follow-up.
Recurrence rate at 1-year follow-up was 4.7% (3 patients on 63), at 3-year follow-up was 11.7% (4 on 34), and at 5-year follow-up was 23.07% (3 on 13), showing that this approach is associated with a recurrence rate similar with the other surgical technique.
However, according to Doll
22
and to a meta-analysis by Milone et al.,
23
a follow-up of at least 5 years should be considered the gold standard in
Unfortunately, in our study, only 13 patients completed the 5-year follow-up, and this aspect can be considered as a limitation of this study in giving adequate conclusions about long-term outcomes.
Furthermore, the retrospective design of this study and the relatively small number of included patients let larger prospective studies validate our results.
Nevertheless, our results encouraged to adopt an endoscopic approach even in case of recurrent
Footnotes
Disclosure Statement
No competing financial interests exist
Funding Information
No funding was received.