
Abstract
Background:
Temporary diverting enterostomy might be the initial step while treating gastrointestinal disorders in infants. According to the level of the stoma, calorie, fluid, and electrolyte imbalance might occur. Totally parenteral nutrition (TPN), parenteral fluid, and electrolyte balancing are the choice of support. Owing to limitations of both, distal refeeding (DR) has been suggested as an alternative. However, in English literature, there is no recommended technique for how DR should apply. This article is aimed at evaluating our innovative DR approach, which was not reported earlier.
Materials and Methods:
Between 2015 and 2019, patients on whom DR was performed by a cuffed silicon-based tunneled catheter were obtained.
Results:
A total of 8 patients aged between 1 day and 7.5 years were included. Dislocation of the catheter and skin erosion were the minor complications that were observed. None of them necessitated TPN and vascular access. Moreover, patients could be discharged and were fully fed orally by their guardian at home, and any problem was observed during survival.
Conclusion:
Consequently, patients did not necessitate vascular access or TPN. They were all fully fed orally, and DR could be performed without a failure to thrive. Therefore, we believe that tunneled catheter DR is a safe and reliable method in infants. Institutional Review Board at Eskisehir Osmangazi University (Protocol no. 07/01/2020-26).
Introduction
Temporary diverting ostomy is usually necessary while treating necrotizing enterocolitis (NEC), intestinal atresia, volvulus, or spontaneous intestinal perforation in infants. Dysmotility is the other nonsurgical indication for ostomy. The acute problem could be solved in such a complicated situation; however, when oral feeding is started, the sufficiency of electrolyte and caloric intake will be obscure. 1 Moreover, after enterostomy reversal, motility capacity of distal intestine, stricture, or intestinal sufficiency for absorption are the other unknown next issues awaiting one. Having predictive information about the functional and absorption capacity of the distal intestine would be helpful for the surgeon to decide the timing of re-anastomosis.
On the other hand, the level of ostomy has great importance for the facts of liquid, electrolytes, and caloric imbalance. It could be achieved parenterally by total parenteral nutrition, fluid, and electrolyte support. Unfortunately, in infants and newborns, vascular access and long-term totally parenteral nutrition (TPN) support have their own limitations. 2 Therefore, alternative feeding approaches are still in research.
In 1972 Levy et al. and in 1985 Puppala et al. reported on distal drip feeding through distal ostomy.3,4 The increased diameter of distal intestine during reconnection and decreased volume of proximal output has been emphasized in both studies. On one hand, many studies approving DR have been reported in neonates5–13 ; on the other hand, there is no report for what the technical approach should be for DR. Although mostly the Foley catheter has been used for distal intestinal catheterization, Haddock et al. have pointed out serious problems during distal catheterizing. 14 Bleeding that required multiple transfusion, intestinal perforations, and losing patients due to septic shock are the complications that they have mentioned. 14
Consequently, even though there is consensus on the utility of DR, distal intestinal catheterization is still a problem. In this study, technical innovation that could be a key for distal catheterization in DR has been presented.
Materials and Methods
The study has been approved by the Institutional Review Board at Eskisehir Osmangazi University (Protocol no. 07/01/2020-26). A retrospective patient chart review, between 2015 and 2019, was conducted.
Demographics of patients who had undergone distal stoma refeeding were extracted. Types of ostomies, total amount of time for DR, and weight percentiles before and at the end of DR have been compared. Complications while placing or due to the catheter, DR, the necessity of vascular access, TPN, fluid, or electrolyte influences were evaluated.
Patients who had undergone ostomy were all examined thoroughly for the possibility of high proximal output, probability of dysmotility, or whether there is an image of an unused distal intestine. If one was detected, then Hickmann catheter was placed for DR.
Surgical technique
A cuffed and silicon-based catheter is placed (Fig. 1, Hickman, Leonard and Broviac catheter, Bard Access Systems), similar to the Seldinger technique. Figures 2 and 3 show a tunnel beginning from the right upper quadrant and ending adjacent to the ostomy site. The catheter is passed through the tunnel. The cuff of the catheter should be left at the subcutaneous tunnel. The distal opening of the tunnel is placed just near the edge of the stoma, and the catheter is inserted to the distal loop from ostomy (Fig. 2). As an alternative, the distal opening could end just close to the lateral intestinal wall at the subcutaneous ostomy space (Figs. 2 and 4). The catheter could be introduced through a hole from the lateral wall of the intestine if there is enough subcutaneous thickness (Fig. 4). Meanwhile, a purse or primary suture should be left around the catheter at the insertion hole. In this way, the distal opening of the tunnel will not be on the skin. An eight- to ten-centimeter-long catheter should be left in the distal stoma lumen from the ostomy entrance, which can also be inserted through the ileocecal valve.
Catheter that we used for DR. DR, distal refeeding.
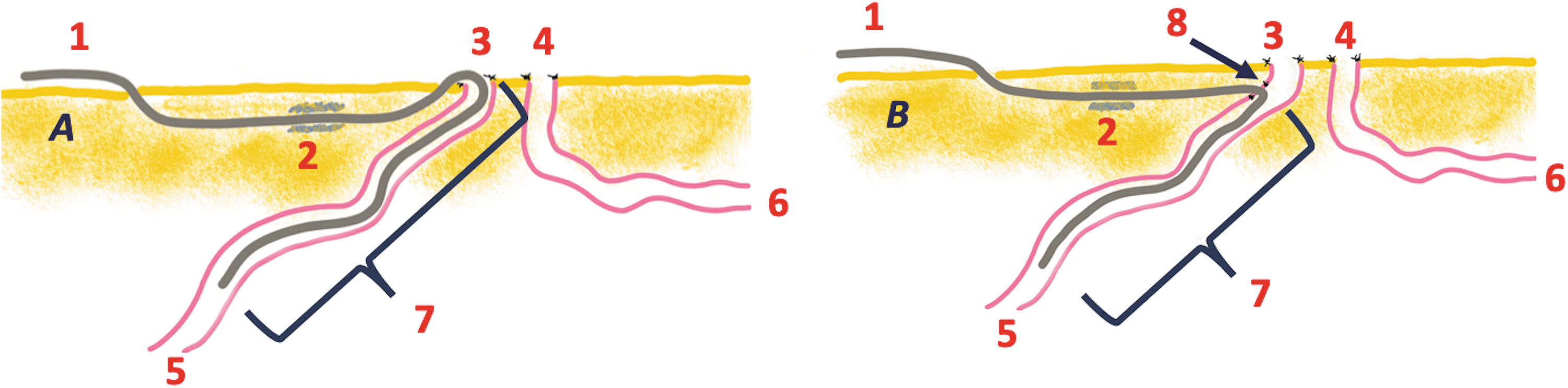
Schematic details of placing the catheter.
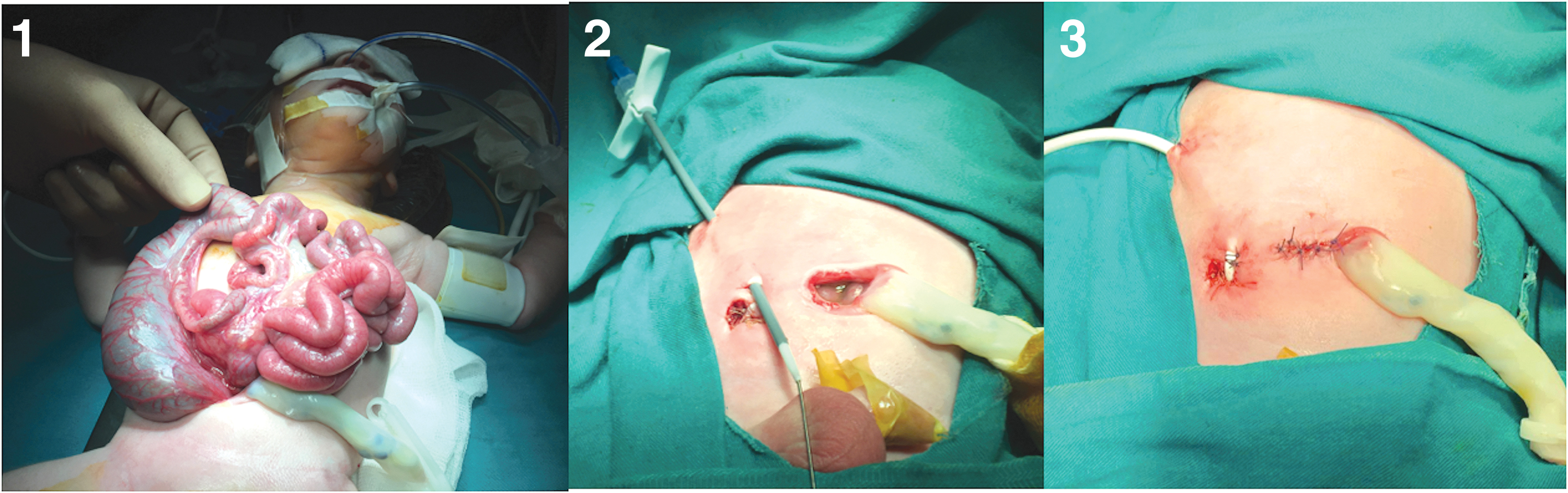
Placing the catheter in a patient (1: gastroschisis, 2: preparing the tunnel of the catheter, 3: type 1 placed the catheter).
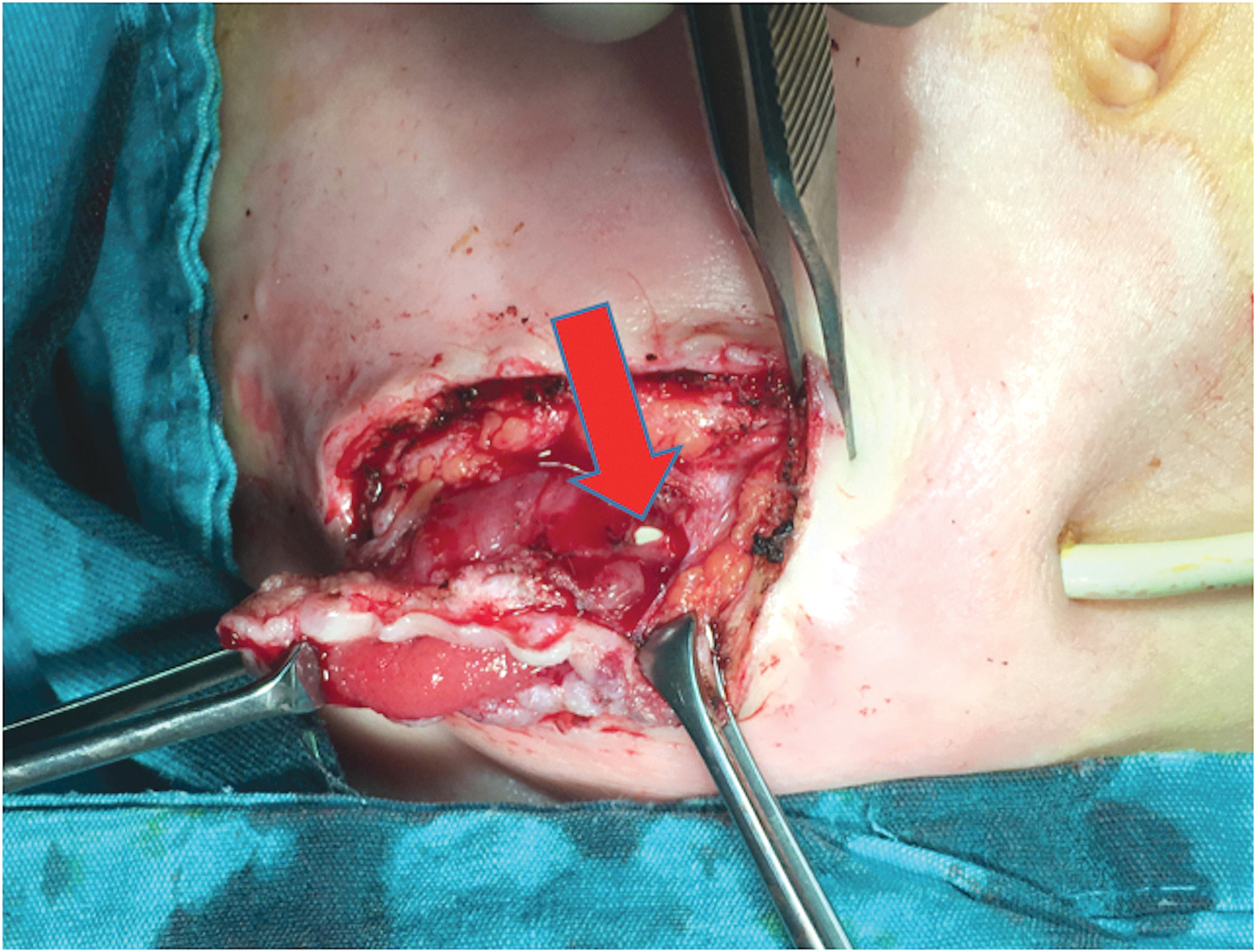
While removing the catheter in a patient with dysmotility that has been placed by the type 2 technique. Arrow points out the entrance of the catheter to the intestine.
The DR by Hickman catheter was begun by 4 × 5 cc/day and increased the volume according to defecation pattern. If it was without any problem, the volume infused was increased 5 cc in every 12 hours. The total amount was increased to as much as proximal output.
A caregiver has been educated for the maintenance of DR. In this way, patients could be discharged and patient growth charts have been followed.
Results
With our approach, DR was performed on a total of 8 patients who were 0- to 7-year-olds. Three of eight patients did not have a central line placed. And even though the other four had a central line, it was not necessitated after DR. The umbilical vein catheter was used in an extremely premature one. The newborn babies had put on TPN during short postoperative time. However, TPN was not started, if the problem was dysmotility. Any patient necessitated long-term TPN or vascular access for electrolyte or caloric imbalance. Moreover, half of the patients were discharged during DR and followed at the outpatient clinic. Details of the patients are tabulated in Table 1.
Details of Patients
Extremely preemie baby.
Patient that is awaiting for relocation.
AR, awaiting for relocation; DR, distal refeeding; SC, stoma closed; TPN, totally parenteral nutrition.
Five of eight patients did not have intestinal resection. Ileostomies were placed on 10, 15, 20, 20, and 45 cm proximal to the ileocecal valve. Two of eight patients had ileal and colonic resection: one with 28 cm ileal, 4 cm of ascending colon, and the other one was with a 32 cm ileal, 4–5 cm ascending colon resection. The ileocecal valve was excised in both. The last one had colostomy at the distal transverse colon owing to suspicion of dysmotility.
No complication was detected due to surgical technique, catheter, or DR or during follow-up after discharge. Regurgitation from distal ostomy was not detected during DR.
Spontaneous dislodgement of the catheter was a minor complication that was detected in 2 patients. It was replaced in one patient, and the other had been planned to be placed once more owing to an unknown motility disorder. The other minor problem was erosion of the skin at the distal anterior wall of the tunnel in an extremely preemie infant.
Discussion
In infants, temporary intestinal diversion might be the initial approach during the surgical treatment of NEC, jejunoileal atresia, cystic fibrosis, spontaneous intestinal perforation, or any other gastrointestinal disorder. Depending on the intestinal level of ostomy, electrolyte, fluid, and calorie imbalance may be experienced. 1 Fluid and electrolyte balance could be provided by parenteral supply and caloric intake by TPN. However, particularly in infants, long-lasting vascular access is a handicap due to weak vascular anatomy at that age. Even though TPN is a good option for support, it also has its own controversies such as infection, cholestasis, and others.15,16 Therefore, DR might be an alternative, with benefits of lowering high output; postoperative complications, lowering discrepancy between proximal and distal bowel diameter while reconnecting.7–10,12,15 Moreover, it may shed light on distal intestinal motility. Hence, the patient might be weaned from TPN; accordingly, they may be freed from TPN-related complications or discharged,
When literature was reviewed, it could be realized that considering Sancar et al. and Schafer et al., there is no suggested technical approach about how DR should be administered.6,17 Schafer et al. suggested continuous distal feeding with proximal output by an enteral feeding pump. The Foley catheter was preferred by Schafer et al., whereas feeding tube or rectal tube was recommended by Sancar et al. The Foley catheter was fixed to distal ostomy by inflating its balloon. However, there is no statement as to whether they had trouble due to the Foley catheter or its balloon. Of note, Sancar et al. have not stated any complication due to the rectal tube or feeding catheter. Moreover, there is no objection about regurgitation, which was the other important problem according to our unpublished data. Dislocation, sticking the stoma bag with the Foley catheter, and meanwhile collecting the output problems have not been reported. On the other hand, in 2015, Haddock et al. emphasized serious problems due to catheterizing the distal ostomy, although they had tried various kinds of catheters. 14 Unfortunately, due to DR technical errors, hemorrhage, intestinal perforation, and mortality are the complications that they have reported. 14 Although our group is a small one, we have not experienced such serious complications. Minor complications, such as dislocation, were resolved after increasing the intraluminal length of the catheter or lateral side (type 2) catheter insertion. Eroding skin of the anterior wall of tunnel was the other complication that was seen in an extremely preemie infant. We believe that it was due to discrepancy between the diameter of the catheter and the thickness of subcutaneous tissue. Persistent pressure, due to the catheter, was the underlying reason. This could have been prevented by a thinner catheter that is produced just for DR.
Indeed, we use a silicon-based catheter (Hickman, Leonard and Broviac catheter, Bard Access Systems) with a cuff that is produced for central venous access in human beings. Therefore, there is no controversy over placing the catheter in infants. According to our unpublished clinical practice, we have also used the Foley catheter or feeding tube for DR. Even though we did not observe serious complications as much as Haddock et al. did, dilatation of the distal intestine, mucosal bleeding, dislocation, and stoma bag adaptation problems due to the catheter were experienced. During DR by proximal output, the discordance of sticking the stoma bag to the skin with a Foley catheter was the other important problem that we faced. Fundamentally, stoma bags are produced just for collecting the proximal output that is not catheter compatible. By using our approach, the catheter is inserted through a subcutaneous tunnel, which allows the stoma bag to stick to the skin easily, as if there is no catheter. Hence, proximal output can be gathered easily. So, the DR can be provided with an intestinal output or formula.
During DR with a feeding or Foley catheter, the other important problem we had experienced was regurgitating of the content that was given distally. The increasing amount of accumulation in the stoma bag with symptoms of dehydration was estimated as regurgitation. However, we did not solve the issue with our innovative technique.
Over and above, even though there is a consensus about the advantages of DR4,7–13 patients were supported by TPN in most of the studies.8,9,11 However, in the follow-up of our group, no more TPN or parenteral fluid replacement was administered.
Besides nutritional support, the quantity and quality of the patient's defecation could demonstrate the functional capacity of the intestine, which is the other expected advantage of this approach. In addition, late onset stricture of intestine is the other known complication of NEC patients. In such situation intolerance to DR might occur and then DR catheter could be helpful for contrast imaging.
In half of the group, the guardian of the patient can give the content through the catheter by a syringe, which was not reported earlier. Hence, this allowed patients to be discharged. Gaining weight and survival of patients have shown that our approach provides the patient's fluid and caloric support at home.
Conclusion
Consequently, any complication was detected while placing the catheter and/or reconnecting the intestine. In the light of our innovative approach, the DR allows patients to wean from TPN, utilize electrolyte balance, and gain weight. Therefore, patients who do not necessitate vascular access or TPN could be discharged and followed up at home.
Therefore, we strongly suggest placing a silicon-based, cuffed long-lasting tunneled catheter as an alternative DR technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.