
Abstract
Background:
The association between morbid obesity and esophageal achalasia is very infrequent. However, over the last decade, these cases started to increase because of the disturbing rise of morbid obesity worldwide. Heller myotomy (HM) and laparoscopic fundoplication represent the best treatment option for esophageal achalasia. However, in morbidly obese patients with achalasia, the best treatment option is not established. We present laparoscopic HM and Roux-en-Y gastric bypass (RYGB) as an alternative treatment for morbidly obese patients with achalasia.
Materials and Methods:
We analyzed the course of patients with achalasia and morbid obesity in our institution undergoing a laparoscopic HM and RYGB, with at least 1 year of follow-up. Symptoms questionnaire, body mass index (BMI), and minuted esophagogram before and after treatment were performed in all patients.
Results:
Seven patients underwent laparoscopic HM and RYGB. All patients had dysphagia. The mean BMI before the onset of symptoms was 42 kg/m2 (range 40 to 50). In 5 patients, preoperative contrast esophagram showed mild or marked dilated esophagus, and in 2, one esophageal curve and severe dilation. Manometry confirmed the diagnosis. At a mean follow-up of 38 months (range 14–69), all patients reported a marked improvement in dysphagia, with median overall satisfaction rating of 10 (range 9–10), and no symptom of gastroesophageal reflux disease (GERD). The mean percentage excess weight loss (%EWL) was 77.1% (range 70.1–98.1) and the mean BMI was 25.7 kg/m2 (range 23–31).
Conclusion:
HM and RYGB are an excellent treatment for morbidly obese patients with achalasia. All patients reported a marked improvement of their dysphagia and no symptoms of GERD. The %EWL and BMI descent was very good and maintained through time, showing also an excellent control for morbid obesity.
Introduction
Esophageal achalasia is a rare motility disorder with an incidence of ∼0.5 to 1.6/100,000 inhabitants according to recent reports. It is defined as an esophageal motility disorder characterized by an absence of esophageal peristalsis with impaired (or incomplete) relaxation of the lower esophageal sphincter (LES). 1 The characteristic symptom is dysphagia, which is usually progressive and associated with secondary weight loss. Complementary studies should include an upper gastrointestinal series (UGI) that will clarify the esophagogastric anatomy, an upper gastrointestinal endoscopy to rule out organic lesion, and an esophageal manometry confirming the esophageal motility disorder diagnosis.
Obesity is reaching epidemic proportions worldwide, with 61% of the adult population being overweight or obese in the United States. 2 Obesity is an independent risk factor for esophageal motility disorders, which may exist in more than 50% of morbidly obese patients. Motility disorders associated with obesity typically include hypertensive LES, nutcracker esophagus, diffuse esophageal spasm, ineffective esophageal motility, and nonspecific motility disorders. 3 Despite its association with these specific motility disorders, obesity is not generally considered to be a risk factor for achalasia.
In general, achalasia and morbid obesity are not expected to be associated, taking into account the weight loss of achalasia patients. However, nowadays, this association is a rising product of the increasing morbidly obese population. Current data show that achalasia may coexist in morbidly obese patients with a prevalence of 0.5%–1%.4,5
In achalasia, treatment primary objective is directed to improve the symptoms, which is achieved by lowering the functional resistance of the LES and improving esophageal emptying. Heller myotomy (HM) with gastric extension associated with an antireflux fundoplication performed laparoscopically represents the gold standard for the treatment of esophageal achalasia.6,7
Patients who are morbidly obese, defined as a body mass index (BMI) greater than 40 kg/m2 or greater than 35 kg/m2 with associated comorbidities, require changes in the standard treatment approach due to the patient's weight. Bariatric surgical procedures have shown to be the best solution for these patients to control the excess weight loss during time. 8
The management of a morbidly obese patient with achalasia is a difficult proposition and the standard surgical approach for each disease does not address the other, and may have deleterious consequences if approached separately. An HM in a patient with achalasia and morbid obesity will relieve dysphagia but will increase weight gain and severe gastroesophageal reflux disease (GERD). Therefore, surgical treatment should solve both problems at the same time and both surgical procedures should complement each other. In these cases, we believe the best treatment option is to perform an HM with gastric extension and a Roux-en-Y gastric bypass (RYGB) in patients with achalasia and morbid obesity. This report examines the results of our approach in a short series of patients.
Materials and Methods
We performed a retrospective review of prospectively collected data of patients with a diagnosis of achalasia who underwent surgery in our institution. The inclusion criteria were patients who underwent an HM with gastric extension and an RYGB, with at least 1 year of follow-up. In our institution, patient selection for this primary combined procedure requires at least a recorded history of BMI greater than 40 kg/m2 or greater than 35 kg/m2 with associated comorbidities before the onset of achalasia symptoms. A thorough discussion of the risks and benefits of this procedure was explained to all patients. All patients were evaluated multidisciplinary by nutrition, psychiatry, clinical, and surgery.
Preoperative workup included a comprehensive questionnaire, UGI, manometry, and endoscopic examination.
Each patient received a questionnaire to assess various aspects of the symptoms and was asked to score the frequency from 0 to 4: 0 = never, 1 = once a month, 2 = once a week, 3 = once a day, and 4 = several times a day, and the severity on a 10-point visual analog scale with 1 being “mild” and 10 as “most severe.” Patients' BMI and excess weight were recorded.
We classified the radiological findings on UGI using the Resano–Malenchini classification 9 :
Stage I: straight esophagus, narrow channel at the gastroesophageal junction (GEJ), visible air level in gastric fundus.
Stage II: dilated esophagus, no esophageal curves, and no air level in the gastric fundus.
Stage III: marked dilation of the esophagus with one curve.
Stage IV: more than one curve, sigmoid esophagus.
Patients were followed at least at 2 weeks, 2 and 6 months, and 1 year postoperative. Symptoms comprehensive questionnaire, UGI, and endoscopic examination were done in all patients. As preoperative, the patients were asked to score the frequency and severity and whether each symptom had improved, worsened, or remained the same as before their procedure. Their perception of the procedure also was scored as to be a success, a partial success, or not a success. Excess weight loss was recorded.
The patient is placed in a low lithotomy position so that the surgeon may stand between the legs while operating. Pneumoperitoneum is established with a Veress needle. The camera port is placed 2 cm to the left of the midline and 10 cm below the costal margin. The upper two ports are used by the surgeon and should form an equilateral triangle with the camera port. The liver retractor and first assistant ports are placed at the level of the camera port in the anterior axillary line. We approach through the left crus of the diaphragm opening the phrenoesophageal ligament and we start dissecting the esophagus. Then we approach the right crus mobilizing the distal esophagus completely, with careful identification and handling of the vagus nerve. The anterior vagus nerve is dissected to free the anterior wall of the esophagus for a correct myotomy. A complete myotomy is performed at the esophagus extending at least 6 cm cephalad from the GEJ and at least 3 cm distally into the stomach.
We then performed an RYGB. We created a gastric pouch, leaving 2–3 cm of normal gastric serosa between the distal gastric myotomy and the staple line. We created a 120-cm Roux limb, performing a stapled side-to-side (functional end-to-side) jejunojejunostomy. The Roux limb is presented in a supracolic position. Depending on surgeon's choice, a gastrojejunal anastomosis is performed manually or stapled side-to-side (45 mm), being careful not to involve the previous myotomy (Fig. 1).
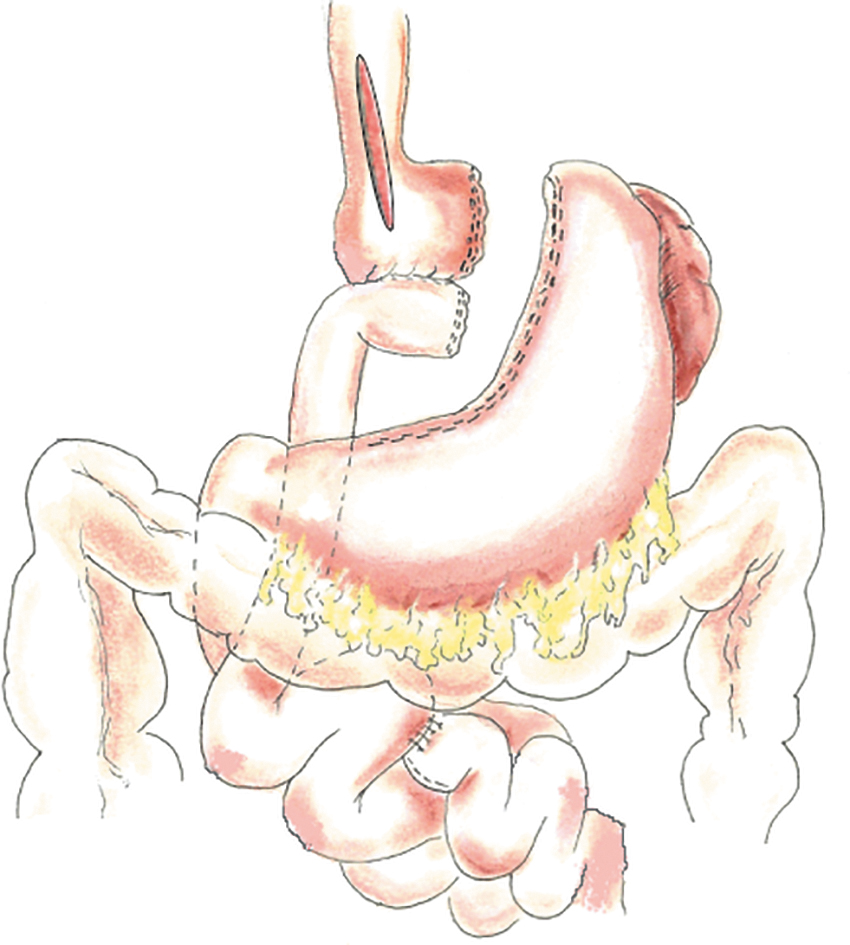
Heller myotomy and Roux-en-Y gastric bypass. Illustration created by Javier Ithurralde-Argerich.
Results
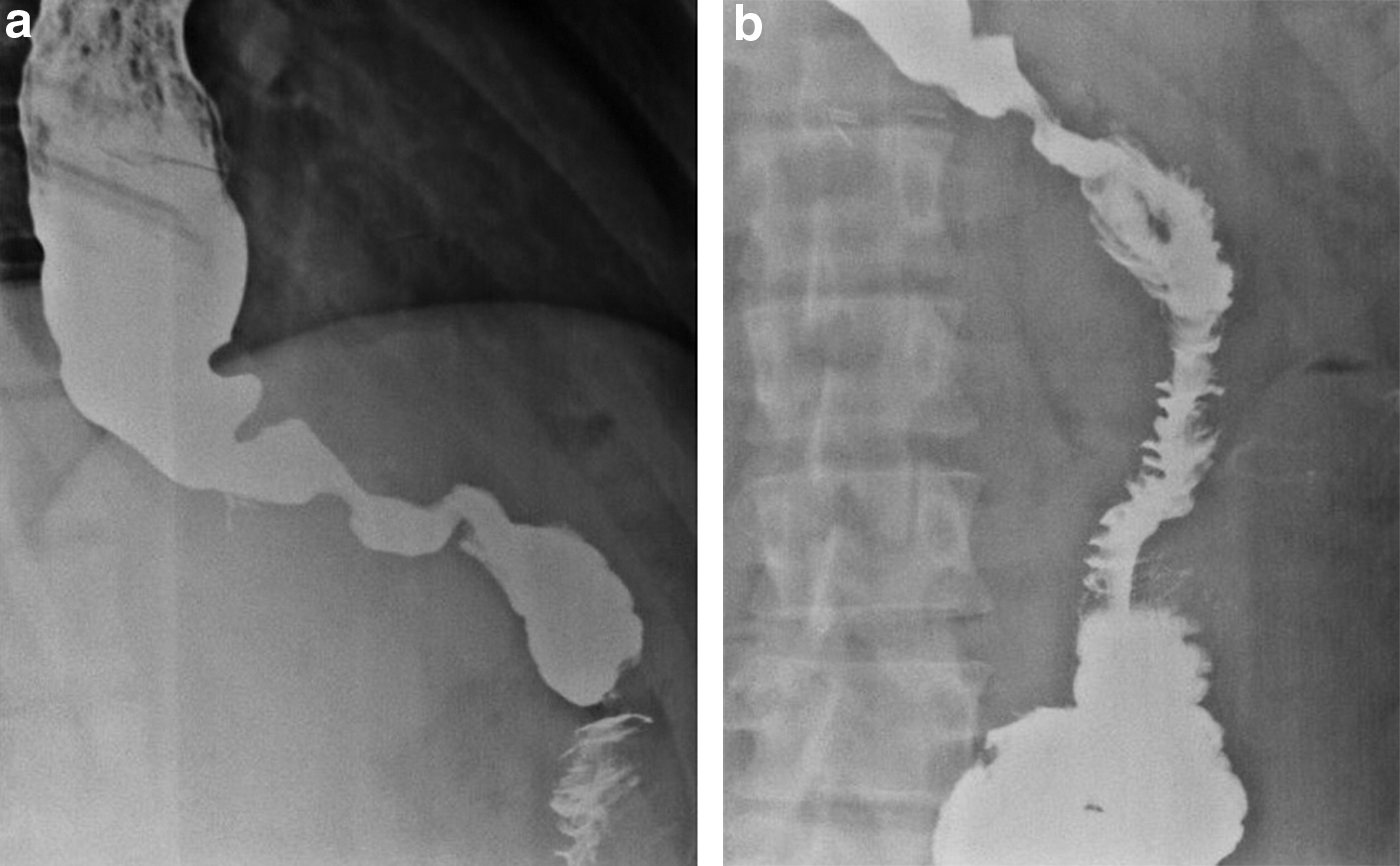
From January 2008 to January 2018, 207 patients with diagnosis of esophageal achalasia underwent surgery in our institution. Seven patients underwent a laparoscopic HM with gastric extension and an RYGB with at least 1 year of follow-up. There were 2 women and 5 men, with ages ranging from 23 to 56 years (mean 44 years) (Table 1). The main symptoms of presentation were dysphagia (100%) and regurgitation (71%). All patients had UGI, 5 patients presented a Stage II disease, and 2 patients a Stage III disease (Fig. 2). Manometry showed in all patients an absence of esophageal peristalsis with impaired relaxation of the LES. Mean BMI and excess weight were 42 kg/m2 (range 40 to 50) and 58 kg (range 47 to 70). All patients were approached laparoscopically, 1 patient needed conversion to open surgery while performing the Roux-en-Y reconstruction due to firm small bowel adhesions from previous surgeries.

Preoperative contrast esophagram showing
Results on Body Mass Index and Percentage Excess Weight Loss After Laparoscopic Heller Myotomy and Roux-en-Y Gastric Bypass
%EWL, percentage excess weight loss; BMI, body mass index; F, female; M, male;
All patients started liquids on the second postoperative day and hospital discharge on the third postoperative day. There were no major complications (Clavien II-IV).
Mean follow-up was 34 months (range 17 to 73 months). Mean percentage excess weight loss (%EWL) was 77.1% (range 70.1 to 98.1) and mean postoperative BMI was 25.7 kg/m2 (range 23 to 31) (Table 1). Questionnaire to assess postoperative dysphagia revealed for frequency a median of 0 (range 0 to 1) and for severity a median of 0 (range 0 to 3). All patients reported a marked improvement of their dysphagia. Median overall satisfaction after laparoscopic HM with gastric extension and an RYGB was 10 (range 9 to 10). Patients were asked for postoperative heartburn and none of the patients had it (Table 2). UGI revealed good esophageal clearance and good gastrojejunal anastomosis emptying in all patients (Fig. 3).
Postoperative contrast esophagram
Postoperative Symptoms and Overall Satisfaction After Laparoscopic Heller Myotomy and Roux-en-Y Gastric Bypass
Discussion
Achalasia and morbid obesity are two completely different pathologies that require surgical treatment for their definitive and effective long-term resolution. The simultaneous association of both is very infrequent, but when they present, they propose a difficult and complex challenge.
In these patients, if we individually treat the achalasia, we know that their symptoms, especially dysphagia, will be resolved. Also, we know that the weight lost due to the restriction of passage through the GEJ caused by the absence of relaxation of the LES will be regained after the extended HM. If weight is regained, these patients will increase their BMI and this will be a big concern for gastroesophageal reflux. It has been shown that in obese patients, BMI remained independently associated with the reflux score. 10 This finding is, in part, explained by the presence, in obese patients, of an increased pressure gradient between the abdomen and the chest known as transdiaphragmatic pressure gradient (TDPG). 11 In obese individuals, the intra-abdominal pressure is increased, correlating with the BMI and the waist circumference, which in many cases is worsened by obstructive sleep apnea, present almost in 70% of morbidly obese, determining a more negative intrathoracic pressure, therefore, increasing the TDPG and promoting reflux. 12
All these elements will boost the probability of developing GERD, considering that they have compromised, first, their antireflux barrier by the hiatus dissection, and second, the mechanism of the LES and the gastric fibers near the GEJ (clash and sling fibers) due to the HM.
Taking into account all the previous factors favoring GERD, one possible solution would be to associate a partial or total fundoplication with the HM. However, we know that in morbidly obese patients associating a fundoplication has a higher failure and recurrence rate for GERD establishing that this would not be the best tactic against GERD.13,14 Furthermore, let us not forget that with this tactic we would still not be solving the second pathology of these patients, which would be their morbid obesity.
Now, if we only treated morbid obesity first, we clearly would not solve the main symptom in these patients, which is dysphagia. Sometimes, the dysphagia could be very mild or not well distinguished, and achalasia could be disregarded. On the contrary, dyspahgia could be very clear and achalasia diagnosis could be easily established, but because of the big weight loss that sometimes represents a great percentage of the BMI, chronic history of morbid obesity is not diagnosed.
Here lies the main importance of diagnosing both diseases, so we can carry out the treatment of the two pathologies simultaneously.
Almogy et al. 4 published the first report in the literature that addresses both pathologies simultaneously. They described the association of an HM with a duodenal switch in a morbidly obese patient with achalasia. We must state that the author surgically left a larger fundus in the sleeve gastrectomy (SG) part of the duodenal switch than usually done, which allowed an anterior partial fundoplication. He performed this procedure on 3 patients, all with a BMI greater than 40. All the patients improved their symptoms satisfactorily. 4
Herbella et al. reported a case where he performed an open biliopancreatic diversion in an achalasia patient. This patient had a history of previously undergoing a laparoscopic heller's myotomy and a partial fundoplication. 15 The results were unsatisfactory in terms of the resolution of symptoms. The author interpreted the results as due to Chagasic etiology of achalasia and a compulsive eating habit.
More recently and published by four different authors, the HM associated with a laparoscopic RYGB was the selected technique for the simultaneous treatment of morbid obesity and achalasia.16–19 In all cases, patients had previous endoscopic treatment with balloon dilation and/or botulinum toxin. One of the patients had a previous SG and they performed an HM and the conversion of SG into an RYGB. All patients had successful weight loss and excellent resolution of dysphagia.
Hagen et al. report the case of a patient with achalasia and morbid obesity where they did a robotic approach for the HM and a laparoscopic approach for an SG. 20 The patient had a satisfactory decrease in weight with complete resolution of dysphagia.
Another technique that has been increasingly used in the past few years for the treatment of achalasia is peroral endoscopic myotomy (POEM). In 2010, Inoue et al. published the results of 17 patients with esophageal achalasia. 21 The procedure consists of an endoscopic creation of a submucosal tunnel, which allows a myotomy by transection of the circular fibers of the distal esophagus. As a counterpart, this procedure is associated with a high incidence of postprocedure gastroesophageal reflux, initially based on the inability to perform simultaneously any kind of fundoplication. Postoperative gastroesophageal reflux after POEM in short and medium follow-up can be as high as 50%.22,23
However, considering that RYGB is an excellent antireflux operation by itself, reflux should not be a problem in these patients. There are no reports of simultaneous treatment of POEM and RYGB. This could be perhaps because it is simpler to perform both procedures laparoscopically in the same act simultaneously and by a single approach, than simultaneously with two different approaches.
However, when the diagnosis of achalasia is made in a patient previously operated for a bariatric surgery, mainly an RYGB, it would seem that the endoscopic approach for performing the myotomy would be ideal, taking into account that the RYGB could prevent the expected gastroesophageal reflux.
Aiolfi et al. performed recently a literature review of treated patients with diagnosis of achalasia and history of bariatric surgery. Twelve studies were included for a total of 28 patients with prior RYGB. The time from RYGB to myotomy ranged from 14 months to 14 years. Surgical HM was performed in 17 patients (61%), while POEM was performed in 11 patients (39%). Postoperative morbidity was 3.6% without differences comparing surgical Heller's myotomy and POEM (6% versus 0%, P = .43). Follow-up time ranged from 1 to 43 months. The overall recurrence rate requiring reoperation was 7%, with no difference comparing surgical HM and POEM (12% versus 0%; P = .25). The study concluded that both HM and POEM appear feasible, safe, and effective in the treatment of achalasia in previously operated RYGB patients. 24
As we mentioned, the literature reported not many authors with one or few patients simultaneously treated for achalasia and morbid obesity and approached with different techniques (Table 3).
Studies with Simultaneous Surgical Management of Achalasia and Morbid Obesity
DS, duodenal switch; LHM, laparoscopic Heller myotomy; LRYGB, laparoscopic Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy; RHM robotic Heller myotomy.
Although small, our series represents the largest case series of patients treated simultaneously for achalasia and morbid obesity in the literature.
Laparoscopy was our approach of choice in all patients. HM associated with an RYGB was our procedure of choice. We believe that HM should be done simultaneously with a procedure that protects morbidly obese patients from postoperative gastroesophageal reflux; otherwise, significant esophageal and extraesophageal symptoms of GERD, with possible complications, would manifest in the near future or later.
As we previously mentioned, associating a fundoplication in these patients has a high risk of failure for antireflux control, in addition to not solving the present or future comorbidities of morbid obesity itself.
For this reason, we associate a bariatric procedure, in our case, an RYGB, as an antireflux mechanism and as treatment for morbid obesity. We believe that associating an RYGB as the bariatric procedure of choice in these patients is the best option. We believe that it is a very good bariatric surgery for postoperative gastroesophageal reflux. RYGB reduces the possibility of gastric reflux by presenting a very small gastric pouch and by presenting a Roux-en-Y reconstruction, deriving the biliopancreatic secretion more than 100 cm from the gastric pouch, efficiently eliminating the possibility of biliopancreatic reflux to the esophagus. 25 Moreover, RYGB has a high success for %EWL and control of comorbidities in the short and long term. 26
Studies have shown that RYGB is superior to SG to control postoperative gastroesophageal reflux.27,28 We do not like associating an HM with an SG, knowing that we will be adding two procedures that tend to give gastroesophageal reflux. Besides the known gastroesophageal reflux effects from the HM, the SG also adds its own factors: change in the angle of His during the creation of the sleeve, decrease in the basal pressure of the LES due to resection of the sling fibers, and the excessive narrowing of the sleeve with creation of a proximal gastric pocket and increased intragastric pressure. 29 Associating these two procedures is an inevitable progress for chronic postprocedure gastroesophageal reflux.
Also, we do not believe that it is more beneficial, or that we have greater control of gastroesophageal reflux, if we perform a duodenal switch or a biliopancreatic diversion. Furthermore, it is known that these procedures are more complex to perform and with a greater number of short- and long-term comorbidities due to their malabsorption. 30
In our series of patients, the association between laparoscopic HM and RYGB presented as an excellent treatment option. It was a procedure without intra- and postoperative major complications. The results were excellent for dysphagia symptom, and the patient satisfaction rate of the procedure was excellent. We achieved a %EWL and a BMI of 77.1 and 25.7 kg/m2, respectively, and the patients did not report clinical symptoms of postoperative GERD.
Conclusion
Laparoscopic HM associated with an RYGB is an excellent simultaneous treatment for morbidly obese patients with esophageal achalasia. All patients reported a marked improvement in their dysphagia and no symptoms of GERD. The postoperative %EWL and BMI were very satisfactory and maintained over time.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.