
Abstract
Background:
To explore the safety and efficacy of laparoscopic extralevator abdominoperineal excision (La-ELAPE) and open extralevator abdominoperineal excision (Op-ELAPE) for patients with lower rectal cancer.
Materials and Methods:
Consecutive 101 patients with lower rectal cancer who underwent La-ELAPE or Op-ELAPE in our institution from January 2014 and May 2018 were analyzed retrospectively. The patients' clinicopathological data and postoperative outcomes were compared between the two groups.
Results:
A total of 101 patients were enrolled in the study, 43 (42.6%) patients successfully underwent La-ELAPE and 58 (57.4%) Op-ELAPE. The Op-ELAPE group had more intraoperative blood loss (P = .03), and longer postoperative hospital stay (P = .01) compared with the La-ELAPE group. There were no significant differences between the two group in terms of the operation time (P = .08), circumferential resection margin positivity (P = 1.00), intraoperative perforation (P = .73), and number of positive lymph nodes (P = .91). There were no significant differences in postoperative complications such as colostomy-associated issues (P = .79), intestinal obstruction (P = 1.00), urinary retention (P = 1.00), perineal wound complications (P = .64), and chronic perineal pain (P = .70) between the two groups. According to the Kaplan–Meier survival analysis and log rank test, the overall survival rate and progression-free survival rate between the two groups also showed no significant difference.
Conclusion:
This study showed that La-ELAPE significantly reduced the intraoperative blood loss and the postoperative hospital stay without increasing postoperative morbidity for patients with lower rectal cancer when compared with Op-ELAPE. It suggests that La-ELAPE is safe and effective for patients with lower rectal cancer. For the experienced endoscopic surgeons, the La-ELAPE might be an alternative surgical treatment.
Introduction
Rectal cancer comprises 40% of all colorectal cancer cases approximately, and nearly half of all rectal cancer cases are diagnosed at the locally advanced stage initially. Due to the special anatomical position of the rectum and lack of serosa enveloping the rectum, locally advanced rectal cancer have higher risk of local recurrence and metastasis than colon cancer. More than 50% of rectal cancer are low rectal cancer. 1
Extralevator abdominoperineal excision (ELAPE) has been increasingly utilized in the treatment of lower rectal cancer over the past decade. The procedure of ELAPE could avoid the occurrence of the “surgical waist,” which usually located to the anal verge 3–4 cm after abdominoperineal excision (APE) procedure. 2 It has the advantages of lowering the local recurrence through reducing the rate of intraoperative perforation (IOP) and circumferential resection margin (CRM) when compared with the abdominoperineal resection.3,4
In recent years, with the rapid development of laparoscopic techniques, laparoscopic surgery has the advantages of minimal invasive, excellent visualization, and meticulous operation, which has led to the realization of laparoscopic extralevator abdominoperineal excision (La-ELAPE). However, it remains controversial whether the La-ELAPE is superior to the conventional open extralevator abdominoperineal excision (Op-ELAPE) with regard to the efficacy and safety.
According to the National Comprehensive Cancer Network (NCCN), laparoscopic surgery has not been recommended as the main procedure for low rectal cancer. 1 Some studies have reported that laparoscopy is associated with similar short- and long-term outcomes when compared with open surgery.5,6 Whereas other studies have shown the laparoscopic approach to be associated with higher rates of CRM positivity and incomplete total mesorectal excision (TME).7,8 For these reasons, the aim of the study was to investigate whether La-ELAPE is comparable with Op-ELAPE for patients with lower rectal cancer in our institution.
Materials and Methods
Patients
This was a single-centered retrospective study of 101 consecutive patients with lower rectal cancer (≤5 cm from the dentate line to the lower margin of the tumor) in Beijing Chaoyang hospital, Capital Medical University between January 2014 and May 2018. Of these patients, 43 patients successfully underwent La-ELAPE and the remaining 58 patients underwent the procedure of Op-ELAPE. All patients successfully underwent R0 resection. The procedure of La-ELAPE or Op-ELAPE was chosen according to the patients' wishes and specific conditions. The protocol of our study meets with the standards of strengthening the reporting of cohort studies in surgery (STROCSS) criteria. 9 All patients were diagnosed with lower rectal cancer according to the preoperative colonoscopy and pathological biopsy (adenocarcinomas). The preoperative clinical staging was assessed by the chest radiography, abdominal and pelvis enhanced CT, and abdominal and pelvis magnetic resonance imaging. The preoperative adjuvant chemoradiotherapy were conducted according to the NCCN guidelines. 1 Surgery was performed 8 weeks after adjuvant chemoradiotherapy. According to the postoperative pathologic results, chemotherapy was recommended to all patients with positive lymph nodes. A multidisciplinary team was provided throughout the course of treatment. The Institutional Review Board of Beijing Chaoyang Hospital, Capital Medical University, approved this study. Written informed consent was obtained from all of the patients before the study.
Surgical process
Both the La-ELAPE and Op-ELAPE procedure were performed by the same surgeon. ELAPE includes abdominal and perineal procedures. Op-ELAPE was conducted as described in the previous literature. 10
As for the La-ELAPE, the five-trocars method was adopted to complete the abdominal operation. First, a 10 mm trocar was inserted into the abdomen at 1 cm above the umbilicus, the left and right umbilical and lateral margin of rectus abdominis were placed with a 5 mm trocar hole. Then, a 12 mm trocar perforation was placed in the right lower abdomen as the main operating hole and a 5 mm trocar was placed at the left lower abdomen. The dissection of rectum and surrounding mesentery followed the standards of TME. 11 The mescorectum was dissected to the beginning of the levator ani muscles, and do not open the potential gap between the levator ani muscle and mesentery. Then, permanent sigmoid colostomy was performed and abdomen was closed. Finally, the patient was afterward turned to jackknife position for the perineal procedure. The dissection was continued into the ischioanal fossa, to the lateral insertion of the levator muscle on the pelvic side wall.
All postoperative specimens were detected by the Pathology Department in our hospital. All pathology reports had to record detailed information on tumor pathological type, tumor differentiation degree, lymph nodes examined, positive lymph nodes, tumor size, pathology TNM (pTNM), CRM positivity, and IOP. The IOP was defined as the perforation site of specimen located at the area of the tumor. CRM positive was deemed to be CRM ≤1 mm. All patients underwent postoperative follow-up, once in 3 months within 2 years after surgery, once in 6 months over 2 years.
Outcome measures
The detailed characteristics of the patients include gender, age, distance to anal verge, American Society of Anesthesiologists physical status (ASA-PS), pathological type, and differentiation degree. The detailed short-term outcomes include total operative time, intraoperative blood loss, duration of hospitalization after surgery, maximun tumor diameter, CRM positive rate, IOP rate, positive lymph nodes, p-TNM staging, and postoperative complications. The postoperative complications included postoperative stoma-associated complications (hernia, prolapse, and necrosis), small bowel obstruction, urinary retention, and perineal wound complications (infection, dehiscence, delayed union, and sinus formation). During the follow-up, the second and third year survival rates were also recorded.
Statistical analysis
The Graphpad Prism 7.0 software was utilized to conduct the data analysis. Student's t test was used to compare measurement data, measurement data were expressed as mean ± standard deviation, chi-square tests were applied to compare the categorical data. The Kaplan–Meier method and the Log-rank test were used to perform survival analysis. P < .05 was considered to be statistically significant.
Results
The characteristics of the two groups
From January 2014 and May 2018, 101 patients with lower rectal cancer successfully underwent ELPAE procedure (Fig. 1). Op-ELAPE was performed in 58 patients and La-ELAPE in 43 patients. There were no significant differences with regards to the gender, age, distance to anal verge, ASA-PS, preoperative tumor T/N-staging, pathological type, and differentiation degree. The detailed characteristics of the two groups were listed in Table 1.
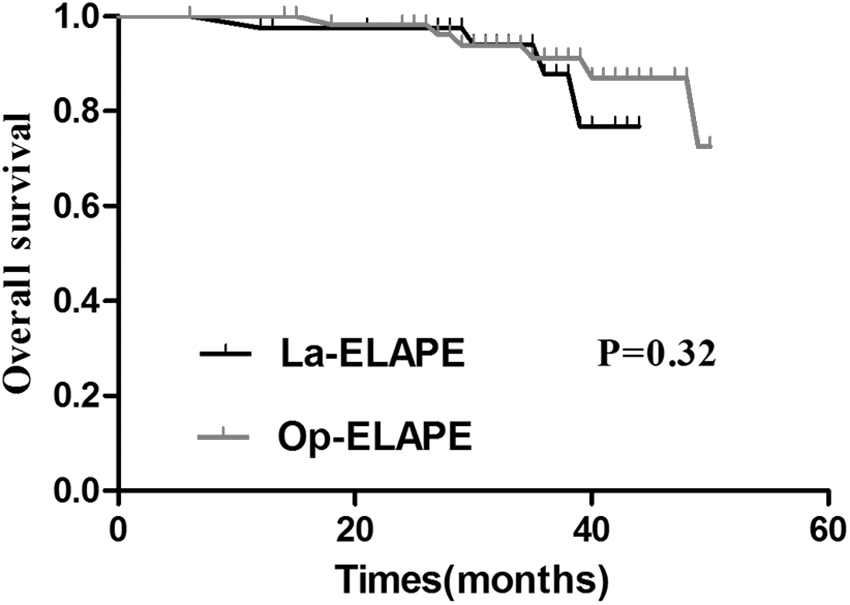
Kaplan–Meier curves showing the overall survival after La-ELAPE and Op-ELAPE (P = .32). La-ELAPE, laparoscopic extralevator abdominoperineal excision; Op-ELAPE, open extralevator abdominoperineal excision.
Baseline Characteristics of the Patients in the Two Groups
Data are from Student's t test.
Data are from chi-square analysis.
ASA-PS, American Society of Anesthesiologists physical status; La-ELAPE, laparoscopic extralevator abdominoperineal excision; Op-ELAPE, open extralevator abdominoperineal excision.
Surgical characteristics of the two groups
The detailed information on surgical characteristics of the two groups were listed in Table 2. The total operative time in the La-ELAPE group (276.42 ± 56.61 minutes) was slightly longer than that in the Op-ELAPE group (247.72 ± 51.57 minutes, P = .08). The intraoperative blood loss (123.76 ± 48.21 mL) and postoperative hospitalization day (9.32 ± 3.89 days) in the La-ELAPE group were significantly shorter than that in the Op-ELAPE group (147.45 ± 56.87 mL; 14.21 ± 4.35 days, P = .03, .01, respectively). There were no significant differences in terms of the CRM positive rate [4.7% (2/43) versus 3.4% (2/58); P = 1.00] and IOP rate [6.9% (3/43) versus 3.4% (2/58); P = .73] between the La-ELAPE and Op-ELAPE group. There were also no significant differences in the number of positive lymph nodes and postoperative pathologic T/N-staging between the two groups. The perineal defect were constructed either by running absorbable suture or biological mesh, there exists no obvious difference in terms of the perineal reconstruction style between the two groups (P = .91).
The Surgical Characteristics of the Two Groups
Data are from Student's t test.
Data are from chi-square analysis.
CRM, circumferential resection margin; IOP, intraoperative perforation; La-ELAPE, laparoscopic extralevator abdominoperineal exision; Op-ELAPE, open extralevator abdominoperineal exision.
Postoperative complications between the two groups
The detailed information on the complications of the two groups was listed in Table 3. The postoperative complications including stoma-associated complications (P = .79), small bowel obstruction (P = 1.00), urinary retention (P = 1.00), perineal wound complications (P = .64), and chronic perineal pain (P = .70) between the two groups were comparable. It is noted that the incidence rate of perineal wound complications and chronic perineal pain in the two groups were up to >20%.
The Postoperative Complications Between the Two Groups
Data are from chi-square analysis.
Stoma-associated complications including hernia, prolapse, and necrosis.
Perineal wound complications including infection, dehiscence, delayed union, and sinus formation.
La-ELAPE, laparoscopic extralevator abdominoperineal excision; Op-ELAPE, open extralevator abdominoperineal excision.
Follow-up
The median follow-up period was 35 (24–40) months for the La-ELAPE group and 43 (24–50) months for the Op-ELAPE group (P = .67). In the La-ELAPE group, 3 patients with local recurrence experienced perineal wound complications, 4 patients had distant metastasis (1 had lung metastasis, 1 had liver, and 2 had bone and lung metastasis). While in the Op-ELAPE group, 6 patients had local recurrence (among which 5 patients experienced perineal wound complications), 7 patients had distant metastasis (2 had bone metastasis; 2 had liver metastasis; and 3 had bone, lung, and liver metastasis). During follow-up, 4 patients in the La-ELAPE group died of local recurrence or metastasis. In the Op-ELAPE group, 2 patients died of LR, 1 died of metastasis, and 2 died of other factors (complications of heart failure and renal failure). The detailed information on the two groups were shown in Table 4. According to the Kaplan–Meier survival analysis and log rank test, the overall survival rate (Fig. 1) and progression-free survival rate (Fig. 2) in the La-ELAPE group and the Op-ELAPE group also showed no significant difference (P > .05).

Kaplan–Meier curves showing the progression-free survival after La-ELAPE and Op-ELAPE (P = .45). La-ELAPE, laparoscopic extralevator abdominoperineal excision; Op-ELAPE, open extralevator abdominoperineal excision.
Efficacy of Treatment, According to Histologic, Surgical, and Clinical Outcome
Data are from Student's t test.
Data are from chi-square analysis.
La-ELAPE, laparoscopic extralevator abdominoperineal excision; Op-ELAPE, open extralevator abdominoperineal excision.
Discussion
In recent years, laparoscopic surgery has gradually become the mainstream of colorectal cancer surgery because of its magnified visualization and fine operation.12–14 van der Pas et al. 15 conducted a COLOR II trial that showed laparoscopic surgery resulted in safety, resection margins, and completeness of resection similar to that of open surgery, and recovery improved after laparoscopic surgery in selected patients treated by skilled surgeons. A COREAN trial, 6 which compared open and laparoscopic surgery for middle or lower rectal cancer after neoadjuvant chemotherapy, showed that laparoscopic resection for locally advanced rectal cancer after preoperative chemoradiotherapy provides similar outcomes in terms of disease-free survival as open resection.
In our study, intraoperative blood loss and postoperative hospital stay in the La-ELAPE group were less than that in the Op-ELAPE group, and the difference was statistically significant (P < .05). The shorter hospital stay after La-ELAPE surgery was in accordance with the result of a study by Kipling et al. 16 These promising results may be attributed to the accumulated experiences in laparoscopy skill and application of the concept of enhanced recovery after surgery during the perioperative period in our center.
The incidence of intestinal obstruction were lower in the La-ELAPE group (4.7%, 2/43) than that in the Op-ELAPE group (5.2%, 3/58), but the difference does not reach to statistical significance (P > .05). Even though not statistically different, it is reported that open surgery is likely to lead to more complications in patients after surgery, and laparoscopic surgery can reduce the incidence of postoperative complications such as intestinal obstruction and intestinal adhesion. 17 Several studies have reported on the short-term or long-term outcomes of laparoscopic surgery for rectal cancer, and these studies showed that laparoscopic surgery is the best option for the surgical treatment of rectal cancer.18–20
In terms of the perineal wound complications, the rate of perineal wound complications in the La-ELAPE group was similar to that in the Op-ELAPE group (P > .05). No difference exists with regard to the primary closure of the perineal defect in the two groups, either by a running absorbable suture or biological mesh. Relevant research reported that perineal wound complications may be found in 30% of patients after the ELAPE technique, regardless of the closure technique. 21
However, it was demonstrated that neoadjuvant radiotherapy significantly increased perineal wound problems. 22 Our results showed that the perineal wound problems after primary closure in patients without neoadjuvant chemoradiotherapy was 12.5% (4/32) after La-ELAPE and 15.6% (7/45) after Op-ELAPE. However, in patients with neoadjuvant chemoradiotherapy, the percentage was 36.3% (5/11) after La-ELAPE and 46.2% (6/13) after Op-ELAPE. Among the perineal wound problems, the chronic perineal pain was the most outstanding issue. Han et al. 23 suggested that the activation of cytokines at the mesh site, resection of coccyx, injury to the pudendal nerves, and extended resection of the pelvic soft tissues during ELAPE procedure may account for the chronic perineal pain.
In the two groups, 4 patients had CRM positivity and 5 patients had IOP in our study. These results lived up to our expectations. Several systematic reviews and meta-analysis confirmed that ELAPE could significantly reduce the rate of CRM positivity and IOP rate when compared with the conventional APE.24–26 In our center, CRM positivity and IOP were rarely met after the application of ELAPE procedure since 2008. In addition, we found no differences between La-ELAPE and Op-ELAPE regarding 3-year overall survival, disease-free survival, and postoperative mortality. In our study, there were no differences between the two groups regarding the surgical steps during the perineal part, hence it does not influence the oncological outcomes.
It remains controversial whether ELAPE is superior to the conventional APE with regard to the oncological outcomes. A study of 1397 patients with APE from the Swedish colorectal cancer registry 27 showed no differences in terms of the 3-year overall survival between ELAPE and conventional APE, but a significantly higher rate of 3-year local recurrence for ELAPE.
Two main limitations of this study should be noted. First, it is a retrospective study, which can easily cause a selection bias. Second, the sample size and follow-up is relatively small and short in our study. A large prospective, randomized, clinical trial and long-term follow-up studies should be conducted to reveal significant differences between the La-ELAPE and Op-ELAPE procedures for lower rectal cancer.
Conclusions
This study showed that La-ELAPE significantly reduced the intraoperative blood loss and the postoperative hospital stay without increasing postoperative morbidity for patients with lower rectal cancer when compared with Op-ELAPE. It suggests that La-ELAPE is safe and effective for patients with lower rectal cancer. For the experienced endoscopic surgeons, the La-ELAPE might be an alternative surgical treatment.
Authors' Contributions
All authors have contributed significantly and are in agreement with the content of the article.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.