
Abstract
Aim:
Vesicoscopic Cohen's reimplantation closely replicates the open procedure and is reported to have equally good results. Robotic assisted vesicoscopic reimplantation (RAVR) is a new procedure, and the information on technique of RAVR is sparse. We present our technique, experience, and early outcome with RAVR and review of literature.
Patients and Methods:
We retrospectively evaluated patients with vesicoureteric reflux grade II and above. These patients were subjected to RAVR. Selection criteria for this procedure were age >4 years, preserved renal function, and bladder capacity >250 mL. Patients with previous bladder surgery or urethral issues were excluded. Patients were operated by DaVinci Si system, and the technique is described in detail. Three ports were placed by use of bougie. The ureters were adequately mobilized before placing in submucosal tunnel.
Results:
Total of 5 ureters were reimplanted in 4 patients (2 females and 1 bilateral). Ureteral tapering was done in 1 patient. Mean port placement time was 25 minutes with 12 minutes of docking time. Mean console time was 70 minutes for unilateral cases and 100 minutes for the bilateral case. There was resolution of reflux in all patients. The mean follow-up duration is 9 months.
Conclusions:
Robotic assisted vesicoscopic reimplantation is a feasible and safe method of replicating Cohen's reimplantation. There is a learning curve with the procedure, and nuances related to the technique need to be learned by the surgeon. This is the third report on RAVR and provides the necessary technical details required by a robotic surgeon to replicate this procedure.
Introduction
Vesicoureteric reflux (VUR) is a commonly encountered pediatric condition with the spectrum ranging from completely asymptomatic to severe high grade reflux leading to renal dysfunction. Reflux management for pediatric patients can be either by antibiotic prophylaxis with wait and watch policy for lower grades or endoscopic and reimplantation procedure for higher grades. With higher grades of VUR and failed endoscopic treatments, operative reimplantation of the refluxing ureter is needed to prevent renal deterioration. 1 Of all the available methods intravesicle Open Cohen's cross trigonal reimplantation (CCTR) is a time tested procedure with high success rate of >96%. 2 Open CCTR has been replicated by laparoscopic intravesicle pneumovesicum method, and several series have reported similar successful outcome. 3 With the advent of robotic systems, most of the laparoscopic and open surgical procedures are being replicated using the advantages of the wristed instruments. Robotic assisted vesicoscopic reimplantation (RAVR) utilizes the same technique of pneumovesicum to do Cohen's reimplantation. We present our technique, experience, and early outcome with RAVR and review of literature.
Patients and Methods
We retrospectively evaluated patients with VUR grade II and above. These patients were subjected to RAVR. Patient selection criteria for this procedure were age >4 years, preserved renal function, and bladder capacity >250 mL. Patients with previous bladder surgery or urethral issues were excluded. These patients were evaluated with a preoperative ultrasound and voiding cysto-urethrogram (VCUG) for reflux grading. A functional nuclear scan for renal function status was done in all patients.
Operative Technique
Patient positioning
Patient was positioned supine with foot end toward patient cart. Soft rolls beneath the pelvis are placed to lift the area above table surface. This is to get space while placing the ports by Bougie method. The patient cart is brought from the foot end, and the docking is very similar to what is done in prostatic surgery procedures. The table is tilted head down before docking.
Port placement
Vesicoscopic port placement is the most important and time-consuming step. We follow a bougie method as described by Abraham et al., 4 with few modifications. There are a total of 3 ports (camera 8 mm and 2 × 5 mm working ports, note that there is no assistant port) (Fig. 1). To start with, the bladder is filled with saline and is filled to 80% of its expected capacity. A size 14/16 lister bougie is placed inside the bladder and is made to poke up in the infraumbilical area. A small incision is made over the tip of the dilator, and the parietal layers are carefully split until the bladder wall is visible. The bladder is then hitched to the edges of incision on either side so that it stays up abutting the abdominal wall. The incision is deepened to incise the bladder wall. Once the bladder lumen is reached there is efflux of saline from the distended bladder. The mucosa is again hitched to the incision edges to doubly ensure that the bladder does not slip down during port insertion. The tip of the dilator will now be out of the bladder, and a 5 mm port is railroaded into the bladder lumen. The port will have a cuff of rubber glove ring for suture fixation with the skin. This provides reinforcement to the stability of the port and prevents dislodgment. The two working ports are placed along an arc centered at pubic symphysis with an angular distance of 35–40°. In this study, an effort is made to be at the lateral edge of the rectus muscle as the parietes will be thinnest at this place and fewer layers will need to be traversed. The bladder needs to stay distended every time a port is placed; this helps to keep the peritoneal contents away.
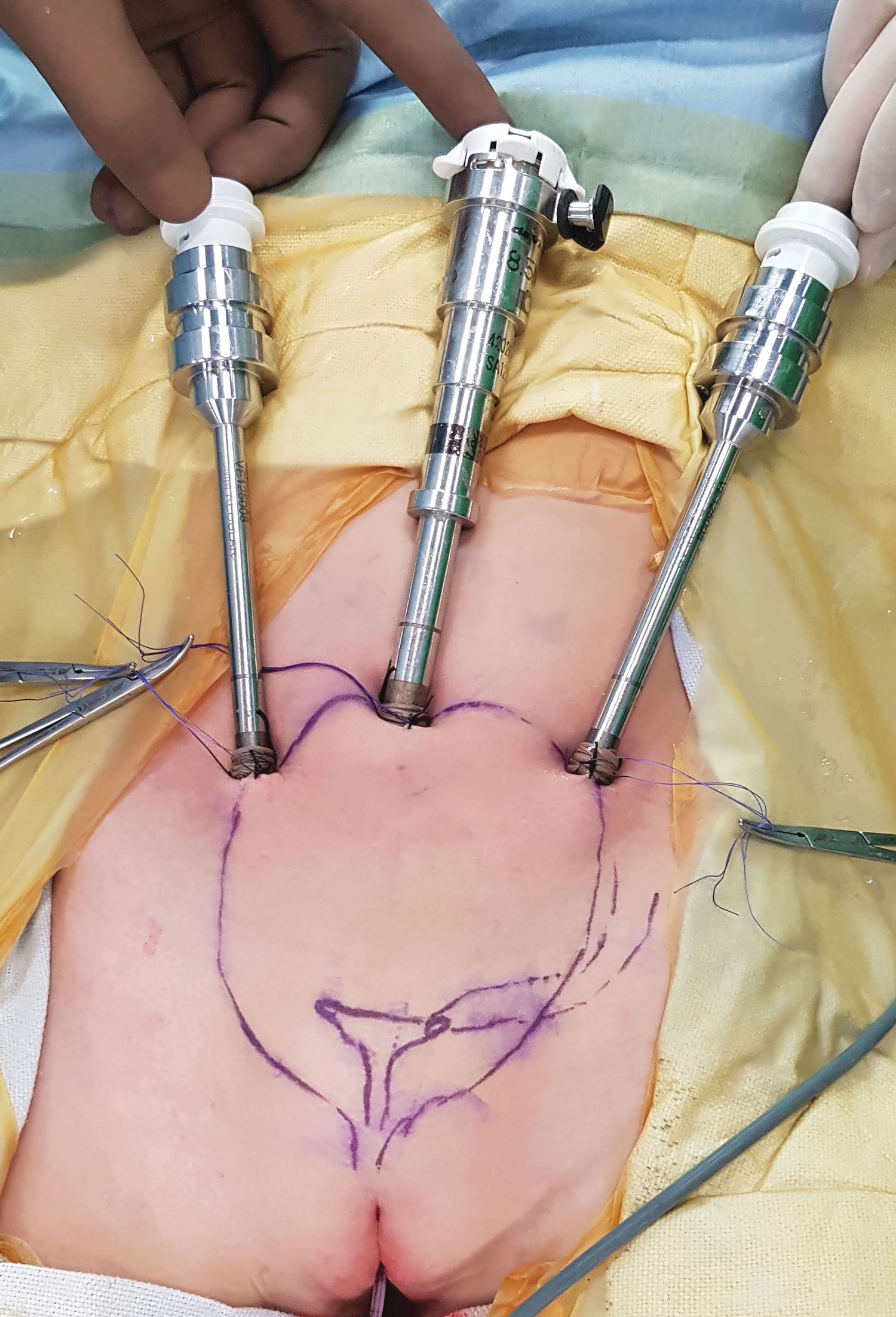
Position of ports. Center port is 8 mm, and two lateral ports are 5 mm.
Docking
We use a dual console DaVinci Si system (Intuitive Surgical, Mountain View, CA). The patient cart is placed at the foot end. The entire table is tilted head end down to 30°. This gives free range of movement for robotic arms, which otherwise tend to hit the patient abdomen and head (Fig. 2). An 8 mm camera and a hook with Maryland grasper are inserted. At this stage the bladder is filled with saline, and now the gas is connected through the camera port. It is important to note that there should be gradual insufflation with aspiration of saline to maintain the bladder bubble. Sudden decompression of bladder while using suction can result in bladder falling off its hitches and port dislodgment. Two 8F feeding tubes are inserted in urethra side by side. One will be used for suctioning, and other will be used for intubating the ureter.

Docking with Si system. Note how the table is tilted 30° head down to all movements for robotic arms.
Procedure
The ureter intended for reimplantation is intubated with 8F feeding tube coming through urethra, and a purse string suture is placed around the ureteral hiatus. The ureter is now mobilized with hook, and it is a combination of sharp and blunt dissection and is no different from what is done in laparoscopy. Once in correct plane, the ureter can be peeled off from the surrounding tissue without much of dissection (Fig. 3). Adequate length of ureter is mobilized. One has to keep in mind that the terminal 2–3 mm of ureter will be trimmed to preserve vascularity.
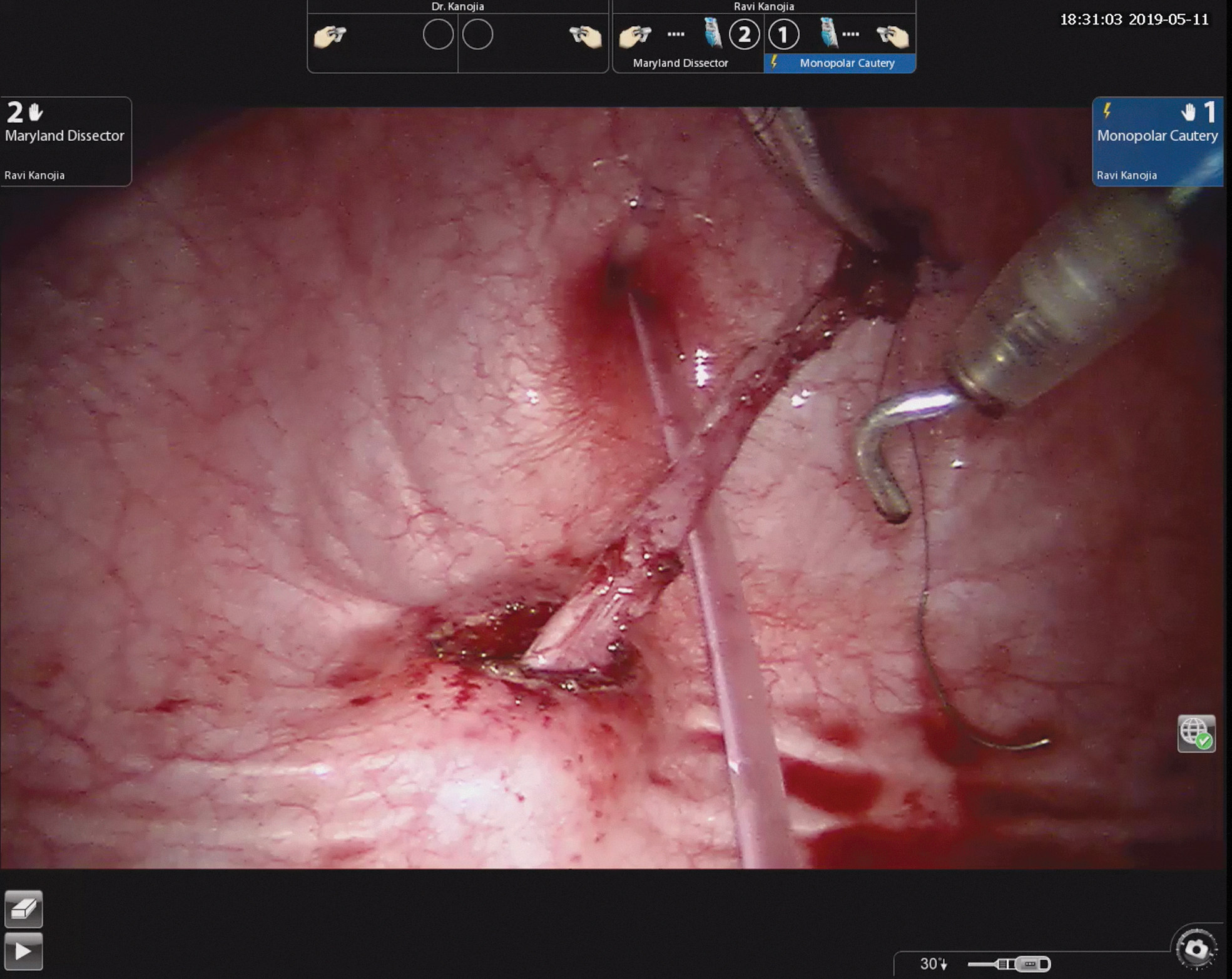
View of completely mobilized ureter. Note the feeding tube being used for frequent suctioning and smoke evacuation.
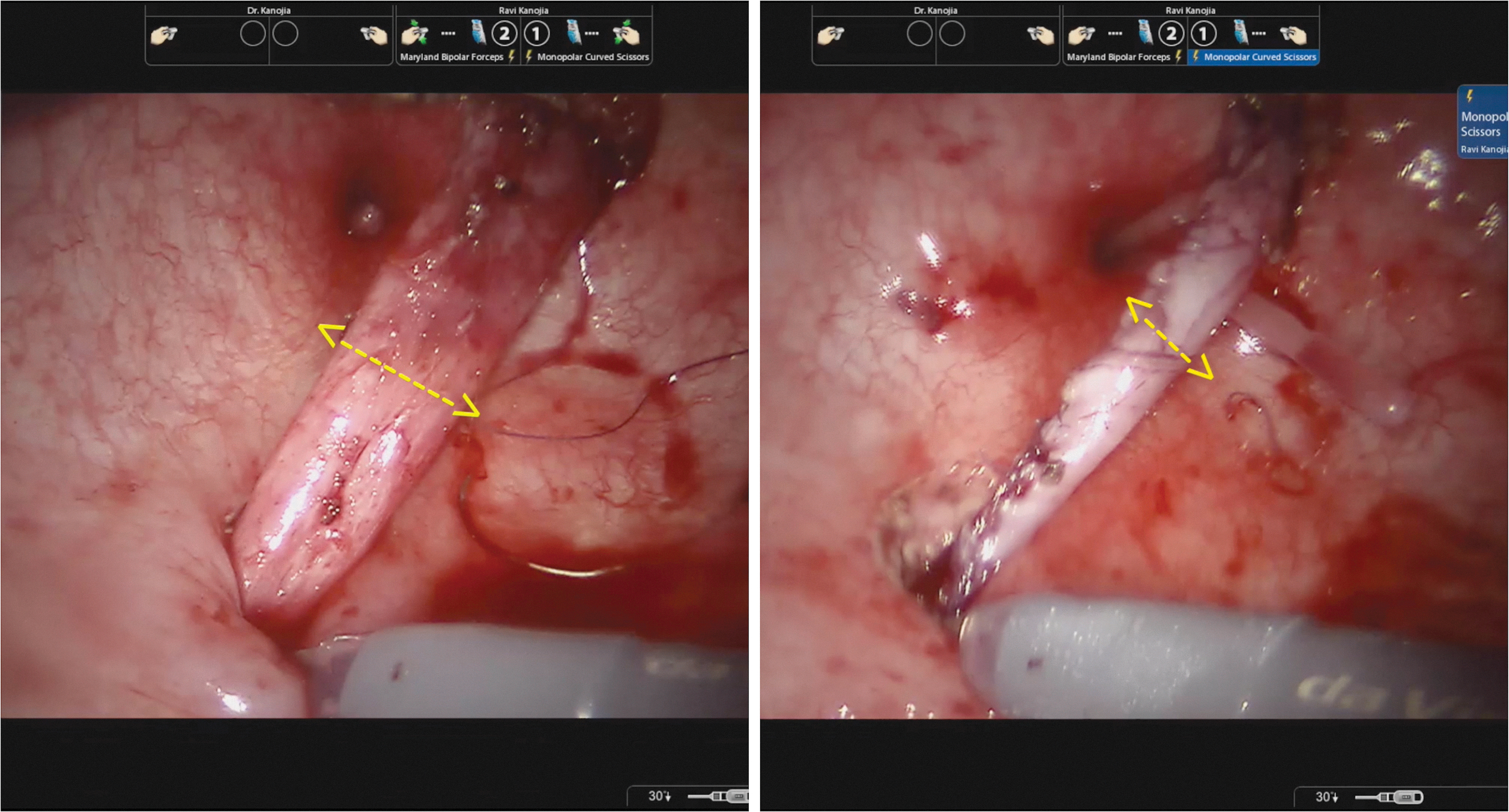
A submucosal tunnel is made with the help of robotic scissors. There is a specific advantage here with the robot because of the wristed instruments. The tunnel is started just above the ureteral hiatus of the opposite side. The opposite ureter is intubated with the feeding tube for identification thus preventing injury to it. The ureter is drawn into the tunnel, and with adequate mobilization, the ureter will not retract into the tunnel if left unattached. The terminal 2–3 mm of the ureter is trimmed to freshen the edges, and a neo-ureterocystostomy is created (Fig. 4). Effort is made with first couple of stitches to include the detrusor for fixing the ureter.

Ureter is pulled through the tunnel, and the terminal part is trimmed before mucosal anastomosis.
The original hiatus from where the ureter was mobilized is closed in two layers: First the detrusor with vicryl and then closure of mucosa with catgut. For bilateral procedures the same steps are repeated on the other side. Except that first both the ureters are mobilized and then placed in tunnel one by one. There can be space and tunnel length problem for second ureter hence the ureter which is more dilated is reimplanted first so that it gets all the length in tunnel it needs. Once both ureters are reimplanted the neo hiatus will be above the original hiatus of the opposite ureter. The two reimplanted ureters are now drained by appropriate sized stents. The tip of the stent is tied with the tip of the Foley so that once the bladder catheter is taken out the stent will come out avoiding the need of cystoscopy in follow-up.
Ureteral tapering
Dilated ureters are difficult to reimplant hence excision ureteral tapering is done after mobilization. The tip of the mobilized ureter is anchored to the roof of the bladder, and ureter is tapered over a 10F feeding tube (Fig. 5).
Excision ureteral tapering for dilated ureter. The tapered ureter is easily pulled into submucosal tunnel.
Some miscellaneous points
Since there is no assistant port every time a cutting operation is done there will be an instrument exchange for inserting either the robotic or lap scissor. There is frequent buildup of smoke and camera lens fogging. The patient side assistant should be well trained and should be able to do all the instrument handling without too much of manipulation and has to constantly look around for instrument collision, wire entanglement, handling the tubes through the urethra, and communicating with the surgeon.
Port closure
Once the procedure is completed the robot is undocked and the anchoring sutures (except the mucosa anchoring sutures) are divided. The port is then made to slide out gently. The surgeon will see the bladder mucosa, which can be closed with two to three sutures. Same steps are followed for all three ports. Once all the hitch stitches are released the bladder falls down to its normal place in pelvis.
Postoperative period and follow-up
The patient is allowed orals after 4 hours and is discharged the next day with oral antibiotics. He goes home with the catheter attached to a leg bag. The urinary catheter is removed after 7 days, and the stents come out with the catheter. A follow-up review is scheduled at 3 months. A VCUG after surgery is not mandatory and can be ordered depending on the relief of symptoms and parental consent. A follow-up renal scan is done after 1 year.
Results
Four patients (2 females) were operated. Total of 5 U were reimplanted (one bilateral). Ureteral tapering was done in 1 patient as he had large dilated ureter. Mean port placement time was 25 minutes with 12 minutes of docking time. Mean console time was 70 minutes for unilateral cases and 100 minutes for the bilateral case. Postoperative VCUG was done in all patients as these were learning curve cases. There was resolution of reflux in all patients. The mean follow-up duration of these patients is 9 months, and all four are asymptomatic.
Discussion
The timeline of pediatric Vesicoscopic reimplantation (VR) dates back to 2001 when Gill et al., 5 described cross trigonal reimplantation. He did vesicoscopy with glycine filled in bladder and used a scope in urethra for visualization. They reported 3 patients aged 10, 11, and 32 years. Later, Yeung et al., 6 described the use of CO2 pneumovesicum in 2005 and described the methods which are used in current time. Since then several large series of VR have been reported. Jayanthi reported 182 patients and reported >98% success rate. 3 Several modifications of the technique have been published and mostly are about individual alterations made in the technique of port placement. 7 In presented series we have followed what is described by Abraham et al., 4 as it is inexpensive and does not require additional expensive instrumentation. Robotic vesicoscopic reimplantation was first described by Peters and Woo in 2005. 8 He described the procedure in 5 patients. They reported success in all patients. The only other series after this on RAVR was by Marchini et al. in 20119 who reported 19 patients as a part of comparative study with open and extravesical reimplantation. None of the above two articles dealt with the technique in detail.
Vesicoscopic reimplantation is a technically challenging procedure. Port placement is the first technical hurdle, and various methods have been described. The technique with the use of curved urethral dilator is easy and reproducible. Other authors have described methods such as T-fasteners, use of cystoscopy, and so on, 7 which are cumbersome. In VR, steps like mobilization of ureter, creating tunnel, and suturing inside the small space of bladder are difficult and have a long learning curve. The Robot here gives technical advantage of added dexterity with the wristed instruments. Dissection and suturing are much easier with the robot than with laparoscopic instruments.
Disadvantages with RAVR are generic to any robotic procedure as longer setup time, need for trained patient side assistant, and added expense. With the newer version of DaVinci system Xi model, there is an instrument size disadvantage as it has all 8 mm instruments. The older Si version has a choice of 5 and 8 mm instruments, and we used 5 mm. With Xi system, it is a compulsion to place three 8 mm ports in bladder, which can raise the need of somewhat longer duration of catheterization as larger defects in bladder are closed at the end of procedure. This is arbitrary and we think that a week of catheter is sufficient with 8 or 5 mm bladder port closures. We are anyways keeping the catheter for a week because the stent is tied to it else catheter can be removed within 48 hours of surgery. Longer catheter duration is a trade-off for avoiding a subsequent cystoscopy and operating room visit for the patient.
Argument can be made in favor of robotic extravesical reimplantation as reported in several series.10,11 Extravesical reimplantation has the advantage of significantly lesser setup time and operative time. However, concerns have been raised about neurovesicle dysfunction in these patients, specially in patients where bilateral reimplantation was done.12,13 Intravesicle reimplantation altogether eliminates the possibility of damage to neural structures behind the bladder and causes minimal changes in bladder dynamics.
A larger data set is needed to establish clinical superiority of robotic VR over other comparable methods and this study does not provide that.
To conclude RAVR is a feasible and safe method of replicating Cohen's reimplantation. There is a learning curve with the procedure, and nuances related to the technique need to be learned by the surgeon willing to do it. This is the third report on RAVR and provides the necessary technical details required by a robotic surgeon to replicate this procedure.
Footnotes
Ethical Approval
Not required, retrospective study with review of operative technique.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.